Pharmacotherapeutic group: HMG-CoA reductase inhibitors.
ATC Code: C10A A08.
Pharmacology: Pharmacodynamics: Mechanism of Action: Pitavastatin competitively inhibits HMG-CoA reductase, the rate-limiting enzyme in the biosynthesis of cholesterol, and inhibits cholesterol synthesis in the liver. As a result the expression of LDL receptors in the liver is increased, promoting the uptake of circulating LDL from the blood, decreasing total cholesterol (TC) and LDL-cholesterol (LDL-C) concentrations in the blood. Its sustained inhibition of hepatic cholesterol synthesis reduces VLDL secretion into the blood, reducing plasma triglyceride (TG) levels.
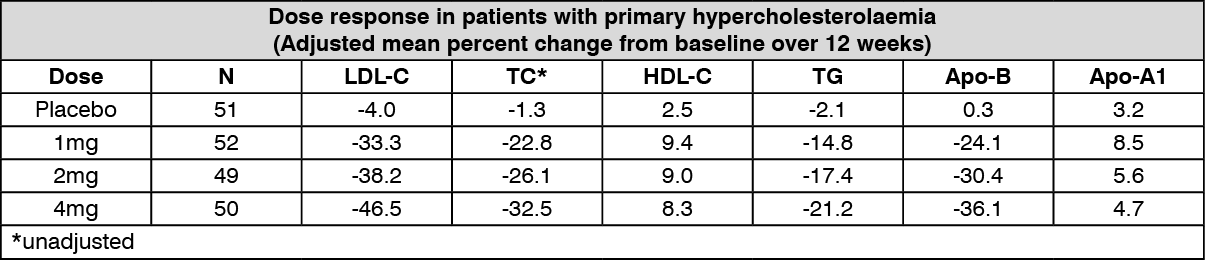
Pharmacodynamic Effects: LIVALO reduces elevated LDL-C, total cholesterol and triglycerides and increases HDL-cholesterol (HDLC). It reduces Apo-B, and produces variable increases in Apo-A1 (see table). It also reduces non-HDL-C and elevated TC/HDL-C, and Apo-B/Apo-A1 ratios. (See table.)
 Click on icon to see table/diagram/image
Clinical efficacy:
Click on icon to see table/diagram/image
Clinical efficacy: In controlled clinical studies which enrolled a total of 1687 patients with primary hypercholesterolaemia and mixed dyslipidaemia, including 1239 patients treated at the therapeutic doses (mean baseline LDL-C about 4.8 mmol/L), LIVALO consistently reduced LDL-C, TC, non-HDL-C, TG and Apo-B concentrations and elevated HDL-C and Apo-A1 concentrations. TC/HDL-C and Apo-B/Apo-A1 ratios were reduced. LDL-C was reduced by 38 to 39% with LIVALO 2mg and 44 to 45% with LIVALO 4mg. The majority of patients taking 2mg achieved the European Atherosclerosis Society (EAS) treatment target for LDL-C (<3 mmol/L).
In a controlled clinical trial in 942 patients aged ≥65 years (434 treated with LIVALO 1mg, 2mg or 4mg) with primary hypercholesterolaemia and mixed dyslipidaemia (mean baseline LDL-C about 4.2 mmol/L), LDL-C values were reduced by 31%, 39.0% and 44.3%, respectively, and about 90% of patients reached the EAS treatment target. More than 80% of the patients were taking concomitant medications, but the incidence of adverse events was similar in all treatment groups and fewer than 5% of patients withdrew from the study due to adverse events. Safety and efficacy findings were similar in patients in the different age subgroups (65- 69, 70-74, and ≥75 years).
In controlled clinical trials which enrolled a total of 761 patients (507 treated with LIVALO 4mg) who had primary hypercholesterolaemia or mixed dyslipidaemia, with 2 or more cardiovascular risk factors (mean baseline LDL-C about 4.1 mmol/L), or mixed dyslipidaemia with type 2 diabetes (mean baseline LDL-C about 3.6 mmol/L), approximately 80% achieved the relevant EAS target (either 3 or 2.5 mmol/L, depending on risk). LDL-C was reduced by 44% and 41%, respectively, in the patient groups.
In long term studies of up to 60 weeks duration in primary hypercholesterolaemia and mixed dyslipidaemia, EAS target attainment has been maintained by persistent and stable reductions of LDL-C, and HDL-C concentrations have continued to increase. In a study in 1346 patients who had completed 12 weeks of statin therapy (LDL-C reduction 42.3%, EAS target attainment 69%, HDL-C elevation 5.6%), values after a further 52 weeks of treatment with pitavastatin 4mg were LDL-C reduction 42.9%, EAS target attainment 74%, HDL-C elevation 14.3%.
In an extension to the two year surveillance study conducted in Japan (LIVES-01, see Adverse Reactions), 6582 patients with hypercholesterolaemia who had received treatment with pitavastatin 1, 2, or 4mg for 2 years, were continued on treatment for a further 3 years (5 years total treatment). During this 5 year study, LDL-C reduction (-30.5%) was maintained from 3 months for the duration of the study, HDL-C values increased by 1.7% at 3 months to 5.7% at 5 years, with greater HDL-C increases seen in patients with lower baseline HDL-C values (<40 mg/dL), e.g. serum levels increased by 11.9% at 3 months to 28.9% after 5 years were observed.
Atherosclerosis: The JAPAN-ACS study compared the effects of 8 to 12 month's treatment with pitavastatin 4mg or atorvastatin 20mg on coronary plaque volume in 251 patients undergoing percutaneous coronary intervention for Acute Coronary Syndrome, guided by intravascular ultrasound. This study demonstrated approximately 17% reduction in plaque volume for both treatments (-16.9 ± 13.9% with pitavastatin and -18.1 ± 14.2% with atorvastatin). Non-inferiority was proven between pitavastatin and atorvastatin and vice versa. In both cases, plaque regression was associated with negative vessel remodelling (113.0 to 105.4 mm
3). There was no significant correlation between LDL-C reduction and plaque regression in this study, in contrast to the findings in placebo-controlled studies.
The beneficial effects on mortality and morbidity have not yet been evaluated.
Diabetes Mellitus: In an open-label prospective controlled study in 1269 Japanese patients with impaired glucose tolerance randomised to lifestyle modification with or without LIVALO 1mg or 2mg daily, 45.7% of patients in the control group developed diabetes in comparison to 39.9% of patients in the LIVALO group over a 2.8 year period, hazard ratio 0.82 [95% CI 0.68-0.99].
A meta-analysis of 4815 non-diabetic patients included in randomised controlled double-blind studies of at least 12-weeks duration (weighted mean follow-up 17.3 weeks [SD 17.7 weeks]) demonstrated a neutral effect for LIVALO on the risk of new-onset diabetes (0.98% of control patients and 0.50% of LIVALO patients developed diabetes, relative risk 0.70 [95% CI 0.30-1.61]) whilst 6.5% (103/1579) of control patients were treated with placebo; the rest were treated with statins including atorvastatin, pravastatin and simvastatin.
Paediatric population: In a double-blind, randomized, multi-centre, placebo-controlled study NK-104-4.01EU (n=106; 48 male and 58 female) children and adolescent patients (≥6 years of age and <17 years of age) with high-risk hyperlipidaemia (fasting plasma LDL-C levels ≥160 mg/dL (4.1 mmol/L), or LDL-C ≥130 mg/dL (3.4 mmol/L) with additional risk factors) received pitavastatin 1mg, 2mg, 4mg or placebo daily for 12 weeks. At study entry, the majority of the patients were diagnosed with heterozygous familial hypercholesterolaemia, approximately 41% of the patients were 6 to <10 years old and approximately 20%, 9%, 12%, and 9% were Tanner stage II, III, IV, and V, respectively. Mean LDL-C was reduced 23.5%, 30.1%, and 39.3% by pitavastatin 1, 2 and 4 mg, respectively, compared to 1.0% for placebo.
In a 52-week open-label extension and safety study NK-104-4.02EU (n=113, including 87 patients from the 12-week placebo-controlled study; 55 male and 58 female) children and adolescent patients (≥6 years of age and <17 years of age) with high-risk hyperlipidaemia received pitavastatin for 52 weeks. All patients started treatment with pitavastatin 1mg daily, and the dose of pitavastatin may have been up-titrated to 2mg and 4 mg to achieve an optimum LDL-C treatment target of <110 mg/dL (2.8 mmol/L) based on LDL-C values at Week 4 and Week 8. At study entry, approximately 37% of the patients were 6 to <10 years old and approximately 22%, 11%, 12%, and 13% were Tanner stage II, III, IV, and V, respectively. The majority of patients (n=103) were up-titrated to 4mg pitavastatin daily. Mean LDL-C was reduced 37.8% at the Week 52 endpoint. In total, 47 patients (42.0%) achieved the AHA minimal LDL-C target of <130 mg/dL and 23 patients (20.5%) achieved the AHA ideal LDL-C target of <110 mg/dL at Week 52. The reduction in mean LDL-C at the Week 52 endpoint was 40.2% for patients ≥6 to <10 years of age (n=42), 36.7% for patients ≥10 to <16 years of age (n=61), and 34.5% for patients ≥16 to <17 years of age (n=9). Patient gender did not appear to have an effect on response. In addition mean TC was decreased 29.5% and mean TG was decreased 7.6% at the Week 52 endpoint.
HIV population: The efficacy of pitavastatin and other statins on LDL-C is reduced in patients with hypercholesterolaemia associated with HIV infection or its treatment compared to patients with primary hypercholesterolaemia and mixed dyslipidaemia without HIV.
In the INTREPID trial, a total of 252 HIV-infected patients with dyslipidaemia (n=126 per arm) entered a 4-week wash-out/dietary lead-in period, and then were randomized to a once daily dose of pitavastatin 4 mg or pravastatin 40 mg for 52 weeks. The primary efficacy endpoint was assessed at Week 12.
The fasting serum LDL-C decreased by 31% and 30% in the pitavastatin treatment group and 21% and 20% in the pravastatin treatment group over 12 and 52 weeks, respectively (LS mean treatment difference -9.8%, P <0.0001 at Week 12, and -8.4% P = 0.0007 at Week 52). There was a statistically significant treatment difference in the mean percent change from Baseline to Weeks 12 and 52 for the secondary efficacy endpoints of TC, non-HDL-C, and Apo B, with a greater decrease in the pitavastatin treatment group than in the pravastatin treatment group for each parameter. No new safety signals or adverse experiences with pitavastatin 4 mg were observed. At Week 52, virological failure (defined as an HIV-1 RNA viral load value >200 copies/mL and a >0.3-log increase from Baseline) was reported for 4 subjects (3.2%) in the pitavastatin group and 6 subjects (4.8%) in the pravastatin group, with no statistically significant differences between treatments.
Pharmacokinetics: Absorption: Pitavastatin is rapidly absorbed from the upper gastrointestinal tract and peak plasma concentrations are achieved within one hour after oral administration. Absorption is not affected by food. Unchanged drug undergoes enterohepatic circulation and is well absorbed from the jejunum and ileum. The absolute bioavailability of pitavastatin is 51%.
Distribution: Pitavastatin is more than 99% protein bound in human plasma, mainly to albumin and alpha 1-acid glycoprotein, and the mean volume of distribution is approximately 133 L. Pitavastatin is actively transported into hepatocytes, the site of action and metabolism, by multiple hepatic transporters including OATP1B1 and OATP1B3. Plasma AUC is variable with an approximately 4-fold range between the highest and lowest values. Studies with SLCO1B1 (the gene which encodes OATP1B1) suggests that polymorphism of this gene could account for much of the variability in AUC. Pitavastatin is not a substrate for p-glycoprotein.
Biotransformation: Unchanged pitavastatin is the predominant drug moiety in plasma. The principal metabolite is the inactive lactone which is formed via an ester-type pitavastatin glucuronide conjugate by UDP glucuronosyltransferase (UGT1A3 and 2B7). In vitro studies, using 13 human cytochrome P450 (CYP) isoforms, indicate that the metabolism of pitavastatin by CYP is minimal; CYP2C9 (and to a lesser extent CYP2C8) is responsible for the metabolism of pitavastatin to minor metabolites.
Elimination: Unchanged pitavastatin is rapidly cleared from the liver in the bile, but undergoes enterohepatic recirculation, contributing to its duration of action. Less than 5% of pitavastatin is excreted in the urine. The plasma elimination half-life ranges from 5.7 hours (single dose) to 8.9 hours (steady state) and the apparent geometric mean oral clearance is 43.4 L/h after single dose.
Effect of food: The maximum plasma concentration of pitavastatin was reduced by 43% when it was taken with a high-fat meal, but AUC was unchanged.
Special populations: Elderly: In a pharmacokinetic study which compared healthy young and elderly (≥65 years) volunteers, pitavastatin AUC was 1.3-fold higher in elderly subjects. This has no effect on the safety or efficacy of LIVALO in elderly patients in clinical trials.
Gender: In a pharmacokinetic study which compared healthy male and female volunteers, pitavastatin AUC was increased 1.6-fold in women. This has no effect on the safety or efficacy of LIVALO in women in clinical trials.
Race: There was no difference in the pharmacokinetic profile of pitavastatin between Japanese and Caucasian healthy volunteers when age and body weight was taken into account.
Paediatric population: There are limited pharmacokinetic data in children and adolescents. In study NK-104-4.01EU (see Pharmacodynamics previously mentioned) sparse sampling revealed a dose-dependent effect on pitavastatin plasma concentrations at 1 hour post dose. There was also indication that concentration at 1 hour post dose were (inversely) related to body weight and may be higher in children than adults.
Renal insufficiency: For patients with moderate renal disease and those on haemodialysis increases in AUC values were 1.8-fold and 1.7-fold respectively (see Dosage & Administration).
Hepatic insufficiency: For patients with mild (Child-Pugh A) hepatic impairment AUC was 1.6 times that in healthy subjects, while for patients with moderate (Child-Pugh B) hepatic impairment AUC was 3.9-fold higher. Dose restrictions are recommended in patients with mild and moderate hepatic impairment (see Dosage & Administration). LIVALO is contraindicated in patients with severe hepatic impairment.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on results from conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity carcinogenic potential, toxicity to reproduction. Indications of renal toxicity were seen in monkeys at exposures greater than those reached in adult humans administered the maximum daily dose of 4mg and urinary excretion plays a far greater role in the monkey than in other animal species. In vitro studies with liver microsomes indicate that a monkey-specific metabolite may be implicated. The renal effects observed in monkeys are unlikely to have clinical relevance for humans, however the potential for renal adverse reactions cannot be completely excluded.
Pitavastatin had no effect on fertility or reproductive performance and there was no evidence of teratogenic potential. However, maternal toxicity was observed at high doses. A study in rats indicated maternal mortality at or near term accompanied by fetal and neonatal deaths at doses of 1 mg/kg/day (approximately 4 fold greater than the highest dose in humans on an AUC basis). To determine the juvenile toxicity of pitavastatin, it was administered via oral to rats from post-natal 28-day through 56-day with a 28-day non-dosing recovery phase. As the result, the no-observed-adverse-effect level was 7.5 mg/kg/day though the decrease in body weights was observed at 15 mg/kg/day. There was no effect of pitavastatin on developmental, functional, or neurological indices to juvenile rats at any dose level.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
