Pharmacotherapeutic group: Sex hormones and modulators of the genital system, Estrogens, Natural and semisynthetic estrogens, plain; Estradiol.
ATC Code: G03CA03.
Pharmacology: Pharmacodynamics/Pharmacokinetics: Lenzetto provides systemic estrogen replacement therapy by releasing estradiol, the major estrogenic hormone secreted by the ovaries. The active ingredient, synthetic 17beta-estradiol, is chemically and biologically identical to endogenous human estradiol. It substitutes for the loss of estrogen production in menopausal women and alleviates menopausal symptoms.
Absorption: When Lenzetto was applied to the skin, the average drying time was 90 sec (median = 67 sec).
In a multiple-dose study, postmenopausal women were treated for 14 days with one, two or three 90-microliter sprays of Lenzetto on the inner forearm. Serum concentrations of estradiol appeared to reach a steady-state after 7-8 days of application of Lenzetto.
Following morning administration, blood levels remained relatively stable and within the therapeutic range throughout the 24-hour period following administration with peak levels between 2 AM and 6 AM.
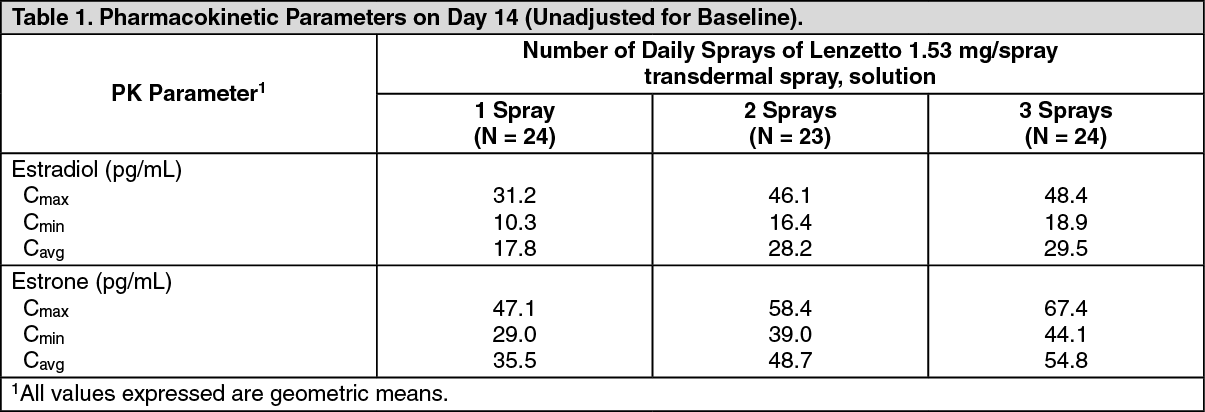
In a clinical study, postmenopausal women were treated for 12 weeks with one, two or three 90-microliter sprays of Lenzetto on the inner forearm and blood levels of estradiol were measured at Week 4, 8 and 12. The estradiol exposure increased with increasing dose (one, two, three sprays respectively) but the increase was slightly less than proportional to dose.
Pharmacokinetic parameters for estradiol and estrone from one, two or three 90-microliter sprays of Lenzetto were further examined in a clinical study and are described in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
A second pharmacokinetic study assessed serum estradiol concentrations in 20 postmenopausal women treated for 18 days with three 90-microliter sprays of Lenzetto on the inner forearm. In this study, application of sunscreen one hour prior to the application of Lenzetto caused no significant difference in absorption of estradiol. When sunscreen was applied one hour after the application of Lenzetto, there was approximately a 10% decrease in the absorption of estradiol (see Precautions).
Studies suggest that compared to applying it to the inner surface of the forearm, absorption of estradiol is similar when Lenzetto is applied to the skin of the thigh but is lower when applied to the skin of the abdomen.
Estradiol transfer during administration of Lenzetto: In a clinical trial, 20 postmenopausal women who were treated with three 90-microliter sprays of estradiol transdermal spray (1.53 mg/spray) to their inner forearm, once daily, were assessed for transfer risk, by holding their forearm to the inner forearm of a male for 5 minutes an hour after treatment. During the clinical study, no significant transfer of estradiol was observed. Information on the transfer within one hour is not available (see Precautions).
Elevated skin temperature: A bioavailability study assessed the effect of increased ambient temperature in 24 healthy postmenopausal women with 2 sprays on the forearm. In this study, increased ambient temperature of 35°C for 4 hours caused similar rate and extent of absorption with approximately 10% differences compared to data obtained at room temperature.
Overweight and obese women: To evaluate the influence of obesity on the absorption, a single-dose, comparative bioavailability study was carried out. The study was performed to compare the rate and extent of absorption of estradiol 1.53 mg/spray (90 microliter) in obese and normal weight women under normal temperature conditions after application of two sprays on the forearm. Based on the point estimates of baseline corrected unconjugated estradiol and unconjugated estrone, the extent and rate of absorption are approximately 33-38% and 15-17% lower while the median peak of absorption is observed 12 to 14 hours earlier. For baseline corrected total estrone, the extent and rate of absorption are approximately 7% lower and approximately 22% higher respectively, in obese post-menopausal females. The Tmax is delayed by approximately 6 hours in obese post-menopausal females for this analyte.
Distribution: Estrogens circulate in blood largely bound to sex hormone binding globulin (SHBG) and albumin.
Biotransformation: Estradiol is converted reversibly to estrone, and both can be converted to estriol, which is the major urinary metabolite. Estrogens also undergo enterohepatic recirculation via sulfate and glucuronide conjugation in the liver, biliary secretion of conjugates into the intestine, and hydrolysis in the gut followed by reabsorption. In postmenopausal women, a significant proportion of the circulating estrogens exist as sulfate conjugates, especially estrone sulfate, which serves as a circulating reservoir for the formation of more active estrogens.
Elimination: Estradiol, estrone and estriol are excreted in the urine along with glucuronide and sulfate conjugates. Serum concentrations of estradiol, estrone and estrone sulfate returned to baseline levels in more than one week after discontinuation of therapy once steady-state had been achieved.
Toxicology: Preclinical safety data: Conventional studies of general toxicity data revealed no additional risks in addition to what has already been reflected in the PI. Long-term continuous administration of natural and synthetic estrogens in certain animal species increases the frequency of carcinomas of the breast, uterus, cervix, vagina, testes and liver (see Precautions).
Animal studies with estradiol or estradiol valerate have shown embryolethal effects even at relatively low doses; malformation of urogenitalia and feminisation of male foetuses.
Octisalate is included in the formulation as an excipients to enhance skin penetration. Octisalate has been widely used in commercial dermal products for many years. Despite the absence of many formal toxicity studies, octisalate is unlikely to represent any special hazard for humans as both the acute oral toxicity of octisalate and that the subchronic toxicity following dermal or oral route of administration are low. Tests for photo-toxicity and photo-contact allergy in man were negative. Furthermore, tests for mutagenicity, clastogenicity, photo-mutagenicity and photo-clastogenicity, using bacterial and tissue culture tests systems were negative.
An effect of octisalate on human reproduction or carcinogenic actions are unlikely based on the hormone activity and genotoxicity studies conducted and bearing in mind the limited dermal penetration of octisalate, the relatively small dose of octisalate in the product (8.5%) and the absence of any reported effects from the extensive human use in sunscreens and cosmetics.
Environmental risk assessment studies have shown that the active ingredient estradiol hemihydrate may pose a risk for aquatic environment, especially for fish.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
