Pharmacotherapeutic group: Immunosuppressants, Selective immunosuppressants.
ATC code: L04AA34.
Pharmacology: Pharmacodynamics: Mechanism of action: Alemtuzumab, is a recombinant DNA-derived humanised monoclonal antibody directed against the 21-28 kD cell surface glycoprotein CD52. Alemtuzumab is an IgG1 kappa antibody with human variable framework and constant regions, and complementary-determining regions from a murine (rat) monoclonal antibody. The antibody has an approximate molecular weight of 150 kD.
Alemtuzumab binds to CD52, a cell surface antigen present at high levels on T (CD3
+) and B (CD19
+) lymphocytes, and at lower levels on natural killer cells, monocytes, and macrophages. There is little or no CD52 detected on neutrophils, plasma cells, or bone marrow stem cells. Alemtuzumab acts through antibody-dependent cellular cytolysis and complement-mediated lysis following cell surface binding to T and B lymphocytes.
The mechanism by which LEMTRADA exerts its therapeutic effects in MS is not fully elucidated. However, research suggests immunomodulatory effects through the depletion and repopulation of lymphocytes, including: Alterations in the number, proportions, and properties of some lymphocyte subsets post-treatment; Increased representation of regulatory T cell subsets; Increased representation of memory T- and B-lymphocytes; Transient effects on components of innate immunity (i.e., neutrophils, macrophages, NK cells).
The reduction in the level of circulating B and T cells by LEMTRADA and subsequent repopulation, may reduce the potential for relapse, which ultimately delays disease progression.
Pharmacodynamic effects: LEMTRADA depletes circulating T and B lymphocytes after each treatment course with the lowest observed values occurring 1 month after a course of treatment (the earliest post-treatment time point in phase 3 studies). Lymphocytes repopulate over time with B-cell recovery usually completed within 6 months.
CD3
+ and CD4
+ lymphocyte counts rise more slowly towards normal, but generally do not return to baseline by 12-months post-treatment. Approximately 40% of patients had total lymphocyte counts reaching the lower limit of normal (LLN) by 6 months after each treatment course, and approximately 80% of patients had total lymphocyte counts reaching the LLN by 12 months after each course.
Neutrophils, monocytes, eosinophils, basophils, and natural killer cells are only transiently affected by LEMTRADA.
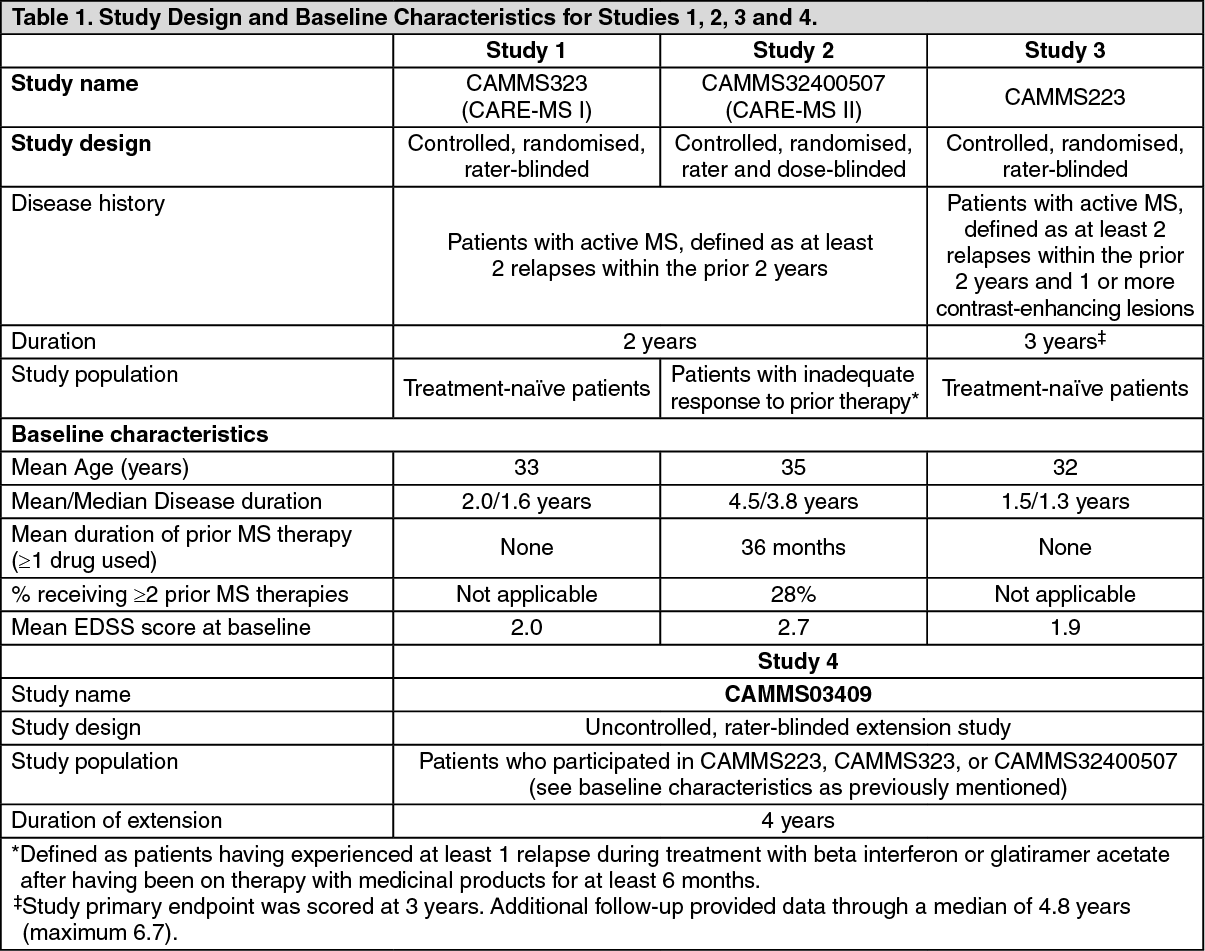
Clinical efficacy and safety: The safety and efficacy of LEMTRADA in MS were evaluated in 3 randomised, rater-blinded, active-comparator clinical trials and 1 uncontrolled, rater-blinded extension study in patients with RRMS.
Study design/demographics for Studies 1, 2, 3 and 4 are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Results for Studies 1 and 2 are shown in Table 2. (See Table 2 and figure.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Relapse severity: In alignment with the effect on relapse rate, supportive analyses from Study 1 (CAMMS323) showed that LEMTRADA 12 mg/day led to significantly fewer LEMTRADA-treated patients experiencing severe relapses (61% reduction, p=0.0056) and significantly fewer relapses that led to steroid treatment (58% reduction, p<0.0001) compared to IFNB-1a.
Supportive analyses from Study 2 (CAMMS32400507) showed that LEMTRADA 12 mg/day led to significantly fewer LEMTRADA-treated patients experiencing severe relapses (48% reduction, p=0.0121), and significantly fewer relapses that led to steroid treatment (56% reduction, p<0.0001) or to hospitalization (55 % reduction, p=0.0045) compared to IFNB-1a.
Confirmed disability improvement (CDI): Time to onset of CDI was defined as a decrease of at least one point on the EDSS from a baseline EDSS score ≥ 2 that was sustained for at least 6 months. CDI is a measure for sustained disability improvement.
29% of patients treated with LEMTRADA reached CDI in Study 2, while only 13% of subcutaneous IFNB-1a treated patients reached this endpoint. The difference was statistically significant (p=0.0002).
Study 3 (phase 2 study CAMMS223) evaluated the safety and efficacy of LEMTRADA in patients with RRMS over the course of 3 years. Patients had an EDSS from 0-3.0, at least 2 clinical episodes of MS in the prior 2 years, and ≥1 gadolinium-enhancing lesion at study entry. Patients had not received prior therapy for MS. Patients were treated with LEMTRADA 12 mg/day (N=108) or 24 mg/day (N=108) administered once per day for 5 days at Month 0 and for 3 days at Month 12 or subcutaneous IFNB-1a 44 μg (N=107) administered 3 times per week for 3 years. Forty-six patients received a third course of LEMTRADA treatment at 12 mg/day or 24 mg/day for 3 days at Month 24.
At 3 years, LEMTRADA reduced the risk of 6-month CDW by 76% (hazard ratio 0.24 [95% CI: 0.110, 0.545], p<0.0006) and reduced the ARR by 67% (rate ratio 0.33 [95% CI: 0.196, 0.552], p<0.0001) as compared to subcutaneous IFNB-1a. LEMTRADA 12 mg/day led to significantly lower EDSS scores (improved compared to baseline) through 2 years of follow up, compared with IFNB-1a (p<0.0001).
In the subgroup of RRMS patients with 2 or more relapses in the prior year and at least 1 Gd-enhanced T1 lesion at baseline, the annualised relapse rate was 0.26 (95% CI: 0.20, 0.34) in the Lemtrada treated group (n= 205) and 0.51 (95% CI: 0.40, 0.64) in the IFNB-1a group (n = 102) (p<0.0001). This analysis includes data from Phase 3 studies only (CAMMS324 and CAMMS323) due to differences in the MRI acquisition algorithms between the Phase 2 and Phase 3 studies. These results were obtained from a post hoc analysis and should be interpreted cautiously.
Long-term efficacy data: Study 4, was a Phase 3, multicenter, open-label, rater-blinded, efficacy and safety extension study for patients with RRMS who participated in Study 1, 2, or 3 (prior phase 3 and 2 studies) to assess long-term efficacy and safety of LEMTRADA. The study provides efficacy and safety through a median of 6 years from entry into Studies 1 and 2. Patients in the extension study (Study 4) were eligible to receive additional as-needed LEMTRADA treatment course(s) upon documentation of resumed disease activity, defined as the occurrence of ≥1 MS relapse and/or ≥2 new or enlarging brain or spinal lesions on magnetic resonance imaging (MRI). Additional course(s) of LEMTRADA were administered at 12 mg/day for 3 consecutive days (36 mg total dose) at least 12 months after the prior treatment course.
91.8% of the patients treated with LEMTRADA 12 mg in Studies 1 and 2 entered Study 4. 82.7% of these patients completed the study. Approximately half (51.2%) of patients initially treated with LEMTRADA 12 mg/day in Study 1 or 2 who enrolled in Study 4, received only the initial 2 courses of LEMTRADA and no other disease modifying treatment throughout 6 years of follow-up.
46.6% of the patients initially treated with LEMTRADA 12 mg/day in Study 1 or 2 received additional courses upon documented evidence of MS disease activity (relapse and/or MRI) and the treating physician's decision to retreat. No characteristics at study entry identified patients who would later receive one or more additional courses.
Through 6 years from initial LEMTRADA treatment, patients continuing in follow-up showed rates of MS relapse, brain lesion formation on MRI, and brain volume loss consistent with LEMTRADA's treatment effects during Studies 1 and 2 as well as predominantly stable or improved disability scores. Including follow-up in Study 4, patients originally treated with LEMTRADA in Studies 1 and 2, respectively, had ARRs 0.17 and 0.23, CDW was seen in 22.3% and 29.7%, while 32.7% and 42.5% achieved CDI. In each year of Study 4, patients from both studies continued to show a low risk of forming new T2 (27.4% to 33.2%) or gadolinium-enhancing lesions (9.4% to 13.5%), and the median annual percent change in brain parenchymal fraction ranged from 0.19% to -0.09%.
Among patients who received one or two additional LEMTRADA treatment courses, improvements were seen in relapse rate, MRI activity and mean disability scores following a first or second LEMTRADA retreatment (Courses 3 and 4) when compared with outcomes in the preceding year. For these patients, the ARR declined from 0.79 in the year prior to Course 3 to 0.18 one year after, and the mean EDSS score from 2.89 to 2.69. The percentage of patients with new or enlarging T2 lesions declined from 50.8% the year prior to Course 3 to 35.9% one year after, and new gadolinium-enhancing lesions from 32.2% to 11.9%. Similar improvements in ARR, mean EDSS score, and T2 and gadolinium-enhancing lesions were seen after Course 4 when compared with the prior year. These improvements were subsequently maintained, but no firm conclusions can be made with regards to the longer-term efficacy (e.g. 3 and 4 years after additional treatment courses) because many patients completed the study before reaching these time points.
The benefits and risks of 5 or more treatment courses have not been established.
Immunogenicity: As with all therapeutic proteins, there is potential for immunogenicity. Data reflect the percentage of patients whose test results were considered positive for antibodies to alemtuzumab using an enzyme-linked immunosorbent assay (ELISA) and confirmed by a competitive binding assay. Positive samples were further evaluated for evidence of
in vitro inhibition using a flow cytometry assay. Patients in clinical trials in MS had serum samples collected 1, 3, and 12 months after each treatment course for determination of anti-alemtuzumab antibodies. Approximately 85% of patients receiving LEMTRADA tested positive for anti-alemtuzumab antibodies during the study, with ≥90% of these patients testing positive also for antibodies that inhibited LEMTRADA binding
in vitro. Patients who developed anti-alemtuzumab antibodies did so by 15 months from initial exposure. Through 2 treatment courses, there was no association of the presence of anti-alemtuzumab or inhibitory anti-alemtuzumab antibodies with a reduction in efficacy, change in pharmacodynamics, or the occurrence of adverse reactions, including infusion associated reactions. High titer anti-alemtuzumab antibodies observed in some patients were associated with incomplete lymphocyte depletion following a third or fourth treatment course, but there was no clear impact of anti-alemtuzumab antibodies on the clinical efficacy or safety profile of LEMTRADA.
The incidence of antibodies is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including inhibitory antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medicines, and underlying disease. For these reasons, comparison of the incidence of antibodies to LEMTRADA with the incidence of antibodies to other products may be misleading.
Pharmacokinetics: The pharmacokinetics of alemtuzumab were evaluated in a total of 216 patients with RRMS who received intravenous infusions of either 12 mg/day or 24 mg/day on 5 consecutive days, followed by 3 consecutive days 12 months following the initial treatment course. Serum concentrations increased with each consecutive dose within a treatment course, with the highest observed concentrations occurring following the last infusion of a treatment course. Administration of 12 mg/day resulted in a mean C
max of 3014 ng/ml on Day 5 of the initial treatment course, and 2276 ng/ml on Day 3 of the second treatment course. The alpha half-life approximated 4-5 days and was comparable between courses leading to low or undetectable serum concentrations within approximately 30 days following each treatment course.
Alemtuzumab is a protein for which the expected metabolic pathway is degradation to small peptides and individual amino acids by widely distributed proteolytic enzymes. Classical biotransformation studies have not been conducted.
Conclusions cannot be made with available data on the effect of race and gender on the pharmacokinetics of alemtuzumab. The pharmacokinetics of alemtuzumab in RRMS has not been studied in patients aged 55 years and older.
Toxicology: Preclinical safety data: Carcinogenesis and mutagenesis: There have been no studies to assess the carcinogenic or mutagenic potential of alemtuzumab.
Fertility and reproduction: Treatment with intravenous alemtuzumab at doses up to 10 mg/kg/day, administered for 5 consecutive days (AUC of 7.1 times the human exposure at the recommended daily dose) had no effect on fertility and reproductive performance in male huCD52 transgenic mice. The number of normal sperm was significantly reduced (<10%) relative to controls and the percent abnormal sperm (detached heads or no heads) were significantly increased (up to 3%). However, these changes did not affect fertility and were therefore considered to be non-adverse.
In female mice dosed with intravenous alemtuzumab up to 10 mg/kg/day (AUC of 4.7 times the human exposure at the recommended daily dose) for 5 consecutive days prior to cohabitation with wild-type male mice, the average number of corpora lutea and implantation sites per mouse were significantly reduced as compared to vehicle treated animals. Reduced gestational weight gain relative to the vehicle controls was observed in pregnant mice dosed with 10 mg/kg/day.
A reproductive toxicity study in pregnant mice exposed to intravenous doses of alemtuzumab up to 10 mg/kg/day (AUC 2.4 times the human exposure at the recommended dose of 12 mg/day) for 5 consecutive days during gestation resulted in significant increases in the number of dams with all conceptuses dead or resorbed, along with a concomitant reduction in the number of dams with viable foetuses. There were no external, soft tissue, or skeletal malformations or variations observed at doses up to 10 mg/kg/day.
Placental transfer and potential pharmacologic activity of alemtuzumab were observed during gestation and following delivery in mice. In studies in mice, alterations in lymphocyte counts were observed in pups exposed to alemtuzumab during gestation at doses of 3 mg/kg/day for 5 consecutive days (AUC 0.6 times the human exposure at the recommended dose of 12 mg/day). Cognitive, physical, and sexual development of pups exposed to alemtuzumab during lactation were not affected at doses up to 10 mg/kg/day alemtuzumab.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image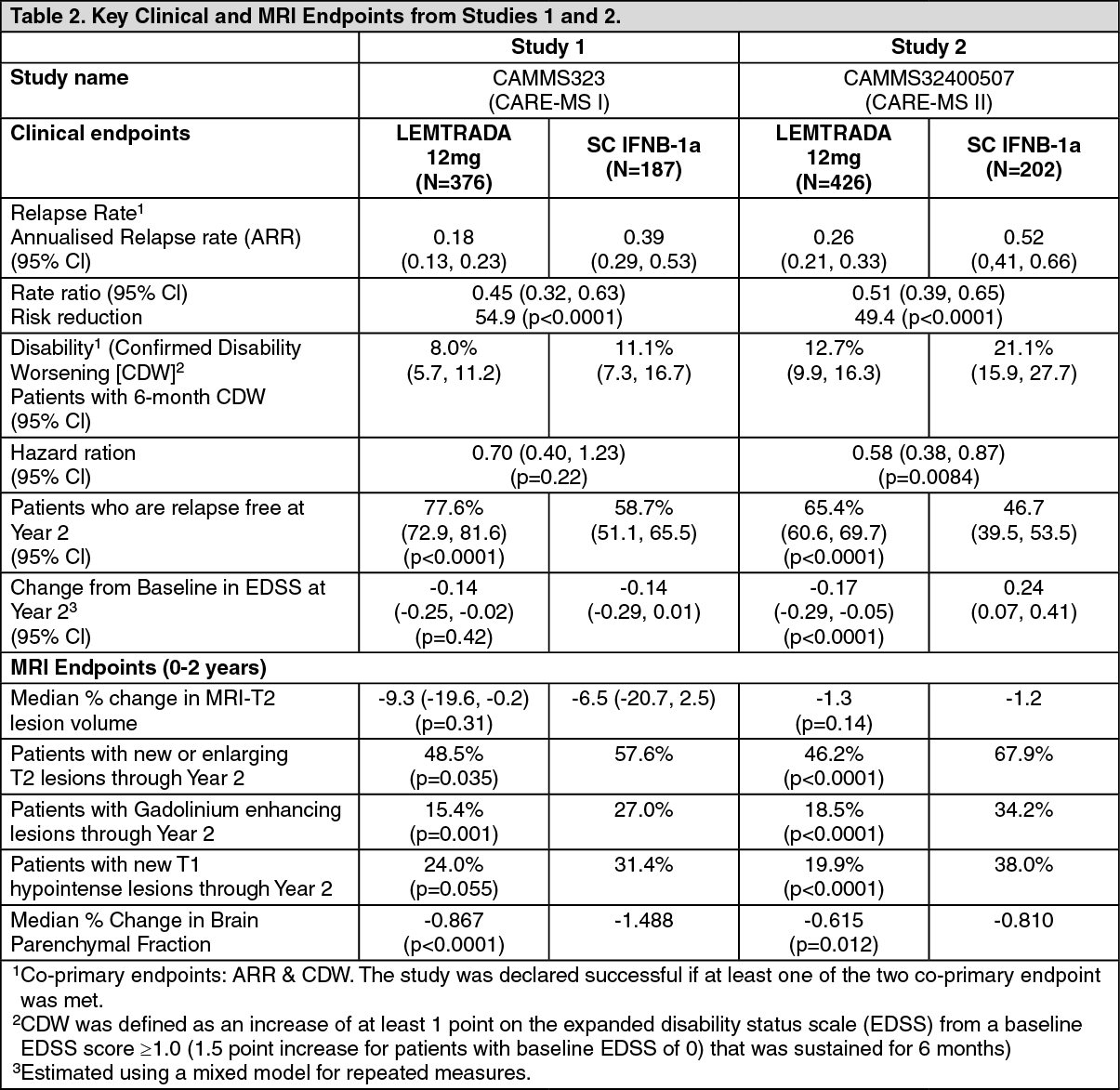 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image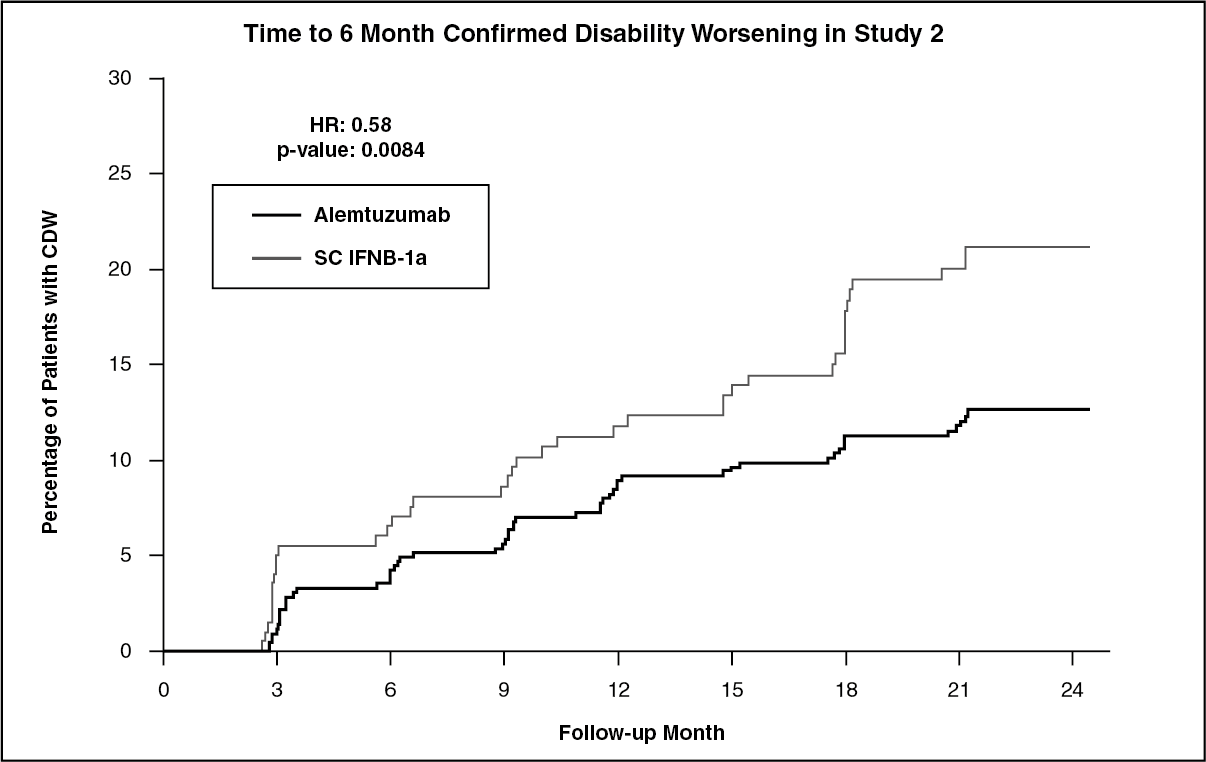 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
