Pharmacotherapeutic group: Antipsychotics, other antipsychotics.
ATC code: N05AX13.
Pharmacology: Pharmacodynamics: Mechanism of Action: Paliperidone, the active ingredient in INVEGA, is a psychotropic agent belonging to the chemical class of benzisoxazole derivatives (atypical neuroleptic antipsychotic). INVEGA contains a racemic mixture of (+)- and (-)-paliperidone.
Paliperidone is a centrally active dopamine D
2 antagonist with predominant serotonergic 5-HT
2A antagonistic activity. Paliperidone is also active as an antagonist at α1 and α2 adrenergic receptors and H
1 histaminergic receptors. Paliperidone has no affinity for cholinergic muscarinic or β1- and β2-adrenergic receptors. The pharmacological activity of the (+)- and (-)- paliperidone enantiomers is qualitatively and quantitatively similar.
The mechanism of action of paliperidone, as with other drugs having efficacy in schizophrenia, is unknown. However, it has been proposed that the drug's therapeutic activity in schizophrenia is mediated through a combination of dopamine Type 2 (D
2) and serotonin Type 2 (5HT
2A) receptor antagonism. Antagonism at receptors other than D
2 and 5HT
2A may explain some of the other effects of paliperidone.
Polysomnography: Centrally-acting medications through their mechanism of action, drug-release profile, and/or time of dose administration may affect sleep. To evaluate the impact of morning dosing of INVEGA on sleep architecture and continuity, a placebo-controlled study was conducted in 36 subjects with schizophrenia in which INVEGA 9 mg or placebo was administered once daily for 14 days. The following observations were made (mean data compared with placebo): reduced latency to persistent sleep by 41.0 (SE 18.70) minutes, decreased sleep onset latency by 35.2 (SE 14.99) minutes, decreased number of awakenings after sleep onset by 7.0 (SE 3.88) events, increased total sleep time by 52.8 (SE 24.01) minutes, increased sleep period time by 41.7 (SE 18.75) minutes, and increased sleep efficiency index by 11.0% (SE 5.00). There was also a statistically significant decrease (relative to placebo) in Stage 1 sleep of 11.9 (SE 4.44) minutes and increase in Stage 2 sleep of 50.7 (SE 17.67) minutes. No clinically relevant effect on REM sleep was observed.
Effect on QT/QTc interval and cardiac electrophysiology: The effects of paliperidone on the QT interval were evaluated in two randomized, double-blind, multicenter, phase 1 studies in adults with schizophrenia and schizoaffective disorder, and in three placebo- and active-controlled 6-week, fixed-dose efficacy trials in adults with schizophrenia.
In the first phase 1 study (n = 141), subjects were randomized to receive either 7 days of immediate-release oral paliperidone once daily (titrated from 4 to 8 mg) or a single dose of moxifloxacin (400 mg). The 8 mg once daily dose of immediate-release oral paliperidone (n = 44) achieved a mean steady-state peak plasma concentration greater than twice the exposure observed with the maximum recommended INVEGA dose of 12 mg (C
max ss = 113 and 45 ng/mL, respectively). In the model-adjusted day-averaged linear-derived QT correction (QTcLD), there was a mean increase of 5.5 msec (90% CI: 3.66; 7.25) in the INVEGA treatment group (n = 44).
In the second phase 1 study (n = 109), subjects were randomized to receive either placebo, the maximum recommended INVEGA dose (12 mg once daily), subsequently titrated to a dose above the recommended range (18 mg once daily), or an active control from the same pharmacologic class of drugs (400 mg quetiapine twice daily). The primary comparison in this 10-day noninferiority study was between INVEGA 12 mg and quetiapine. The least squares mean change from baseline in QTcLD at each individual's observed t
max was estimated to be 5.1 ms lower for 12 mg INVEGA (mean C
max 34 ng/mL) compared with 400 mg quetiapine twice daily (mean C
max 1183 ng/mL) (90% CI: -9.2; -0.9), meeting the prespecified noninferiority criterion of 10 ms. The mean change from baseline in QTcLD at each individual's observed t
max was estimated to be 2.3 ms lower for 18 mg INVEGA (mean C
max 53 ng/mL) compared with 400 mg quetiapine twice daily (mean C
max 1183 ng/mL) (90% CI: -6.8; 2.3).
The mean change from baseline in QTcLD at each individual's observed t
max was estimated to be 1.5 ms higher (90% CI: -3.3; 6.2) for 12 mg INVEGA and 8.0 ms higher (90% CI: 3.1; 12.9) for 400 mg quetiapine twice daily compared with the mean change from baseline in QTcLD at median observed t
max (of the active drug in the comparison) in the concurrent placebo arm. The mean change from baseline in QTcLD at each individual's observed t
max was estimated to be 4.9 ms higher (90% CI: -0.5; 10.3) for paliperidone ER 18 mg and 7.5 ms higher (90% CI: 2.5; 12.5) for quetiapine 400 mg twice daily compared with the mean change from baseline in QTcLD at median observed t
max (of the active drug in the comparison) in the concurrent placebo arm.
None of the subjects had a change from baseline exceeding 60 msec or a QTcLD exceeding 500 msec at any time during either of these studies.
For the three fixed-dose efficacy studies, extensive electrocardiography (ECG) measurements were taken at 15 time points on specified days (including the times of expected C
max) using a standardized methodology. Mean QTcLD increase did not exceed 5 msec in any treatment group at any time point, based on pooled data from 836 subjects treated with INVEGA, 357 subjects treated with olanzapine, and 350 subjects treated with placebo. One subject each in the INVEGA 12 mg and olanzapine groups had a change exceeding 60 msec at one time-point during these studies (increases of 62 and 110 msec, respectively).
Clinical Efficacy: Schizophrenia - adults: The efficacy of INVEGA was established in three placebo-controlled, double-blind, 6-week trials in subjects who met DSM-IV criteria for schizophrenia. An active control (olanzapine) was included for assay sensitivity purposes. INVEGA doses, which varied across the three studies, ranged from 3 to 15 mg once daily. Efficacy was evaluated using the Positive and Negative Syndrome Scale (PANSS); the primary endpoint was decrease in total PANSS scores. An examination of population subgroups did not reveal any evidence of differential responsiveness on the basis of age, race, or gender. Secondary endpoints were also assessed, including Personal and Social Performance (PSP) and the Clinical Global Impression - Severity (CGI-S) scale. The PSP is a validated clinician-rated scale that measures four areas of personal and social functioning (socially useful activities including work and study, personal and social relationships, self care, and disturbing and aggressive behaviors). The CGI-S is an independent investigator-rated assessment of overall severity of illness. In a pooled analysis of these three studies, each dose of INVEGA was superior to placebo on the PSP and CGI-S. In addition, the effect on PSP was distinct from the improvement in symptoms as measured by the primary endpoint, total PANSS. Further evaluation of the open-label extensions of these three studies showed that flexibly-dosed INVEGA (3 to 15 mg once daily) for up to 52 weeks was associated with continued improvement on PSP.
In a long-term trial designed to assess the maintenance of effect, INVEGA was significantly more effective than placebo in maintaining symptom control and delaying recurrence of schizophrenia. In this study, adults who met DSM-IV criteria for schizophrenia and who remained clinically stable on an established dose of INVEGA during an 8-week period of open-label treatment (doses ranging from 3 to 15 mg once daily) after having been treated for an acute episode for the previous 6 weeks with INVEGA (doses ranging from 3 to 15 mg once daily) were then randomized in a double-blind manner to either continue on INVEGA at their achieved stable dose or to placebo until they experienced a recurrence of schizophrenia symptoms. The trial was stopped early for efficacy reasons based on an interim analysis that achieved predefined criteria by showing a significantly longer time to recurrence in patients treated with INVEGA compared to placebo (p = 0.0053). Based on final analysis (including also those patients included after the cut-off point for the interim analysis), the rate of recurrence events was 22.1% in the INVEGA group compared with 51.5% in the placebo group. A significant improvement in symptoms was achieved at the end of the open-label stabilization phase (decrease in PANSS total scores of 38 [SD ± 16.03] points), but after randomization to double-blind treatment, the patients receiving placebo deteriorated significantly more than those on INVEGA (p < 0.001). INVEGA was also significantly more effective than placebo in maintaining personal and social performance. During the double-blind phase of this study as measured by the CGI-S scale, there was worsening on the overall severity of psychosis in the placebo group, while patients treated with INVEGA remained clinically stable.
Schizophrenia - adolescents: The efficacy of INVEGA in adolescent subjects with schizophrenia was established in a randomized, double-blind, parallel-group, placebo-controlled, 6-week study using a fixed-dose weight-based treatment group design over the dose range of 1.5 to 12 mg/day. Subjects were 12-17 years of age and met DSM-IV criteria for schizophrenia, with diagnosis confirmation using the Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SADS-PL).
Eligible subjects were randomly assigned to 1 of 4 treatment groups: a placebo group or INVEGA Low, Medium, or High dose groups. Doses were administered based on body weight to minimize the risk of exposing lower-weight adolescents to high doses of INVEGA. Subjects weighing between 29 kg and less than 51 kg at the baseline visit were randomly assigned to receive placebo or 1.5 mg (Low dose), 3 mg (Medium dose), or 6 mg (High dose) of INVEGA daily, and subjects weighing at least 51 kg at the baseline visit were randomly assigned to receive placebo or 1.5 mg (Low dose), 6 mg (Medium dose), or 12 mg (High dose) of INVEGA daily. Dosing was in the morning without regard to meals.
Efficacy was evaluated using PANSS. This study demonstrated the efficacy of INVEGA in adolescent subjects with schizophrenia when given at daily doses of 3, 6, and 12 mg in body weight-based treatment groups. The minimum effective dose for INVEGA in this population was 3 mg/day.
Schizoaffective Disorder: The efficacy of INVEGA (3 mg to 12 mg once daily) in the treatment of schizoaffective disorder was established in two placebo-controlled, 6-week trials in non-elderly adult subjects who met DSM-IV criteria for schizoaffective disorder, as confirmed by the Structured Clinical Interview for DSM-IV Disorders. In one of these trials, efficacy was assessed in 203 subjects who were assigned to one of two dose levels of INVEGA 6 mg with the option to reduce to 3 mg (n = 105) or 12 mg with the option to reduce to 9 mg (n = 98) once daily. In the other study, efficacy was assessed in 211 subjects who received flexible doses of INVEGA (3-12 mg once daily). Both studies included subjects who received INVEGA either as monotherapy or in combination with antidepressants and/or mood stabilizers. Dosing was in the morning without regard to meals. Studies were carried out in the United States, Eastern Europe, Russia, and Asia.
Efficacy was evaluated using the Positive and Negative Syndrome Scale (PANSS), a validated multi-item inventory composed of five factors to evaluate positive symptoms, negative symptoms, disorganized thoughts, uncontrolled hostility/excitement, and anxiety/depression.
The higher dose group of INVEGA in the 2 dose-level study (12 mg/day with option to reduce to 9 mg/day), and the INVEGA group in the flexible-dose study (dosed between 3 and 12 mg/day, mean modal dose of 8.6 mg/day) were each superior to placebo in the PANSS. In the lower dose group of the 2 dose-level study (6 mg/day with option to reduce to 3 mg/day), INVEGA was not significantly different from placebo as measured by the PANSS.
Taking the results of both studies together, INVEGA improved the symptoms of schizoaffective disorder at endpoint relative to placebo when administered either as monotherapy or in combination with antidepressants and/or mood stabilizers. An examination of population subgroups did not reveal any evidence of differential responsiveness on the basis of gender, age, or geographic region. There were insufficient data to explore differential effects based on race.
Pharmacokinetics: Unless where otherwise stated, the pharmacokinetic information presented in this section are based on data from studies in adults.
The pharmacokinetics of paliperidone following INVEGA administration are dose-proportional within the recommended clinical dose range (3 to 12 mg).
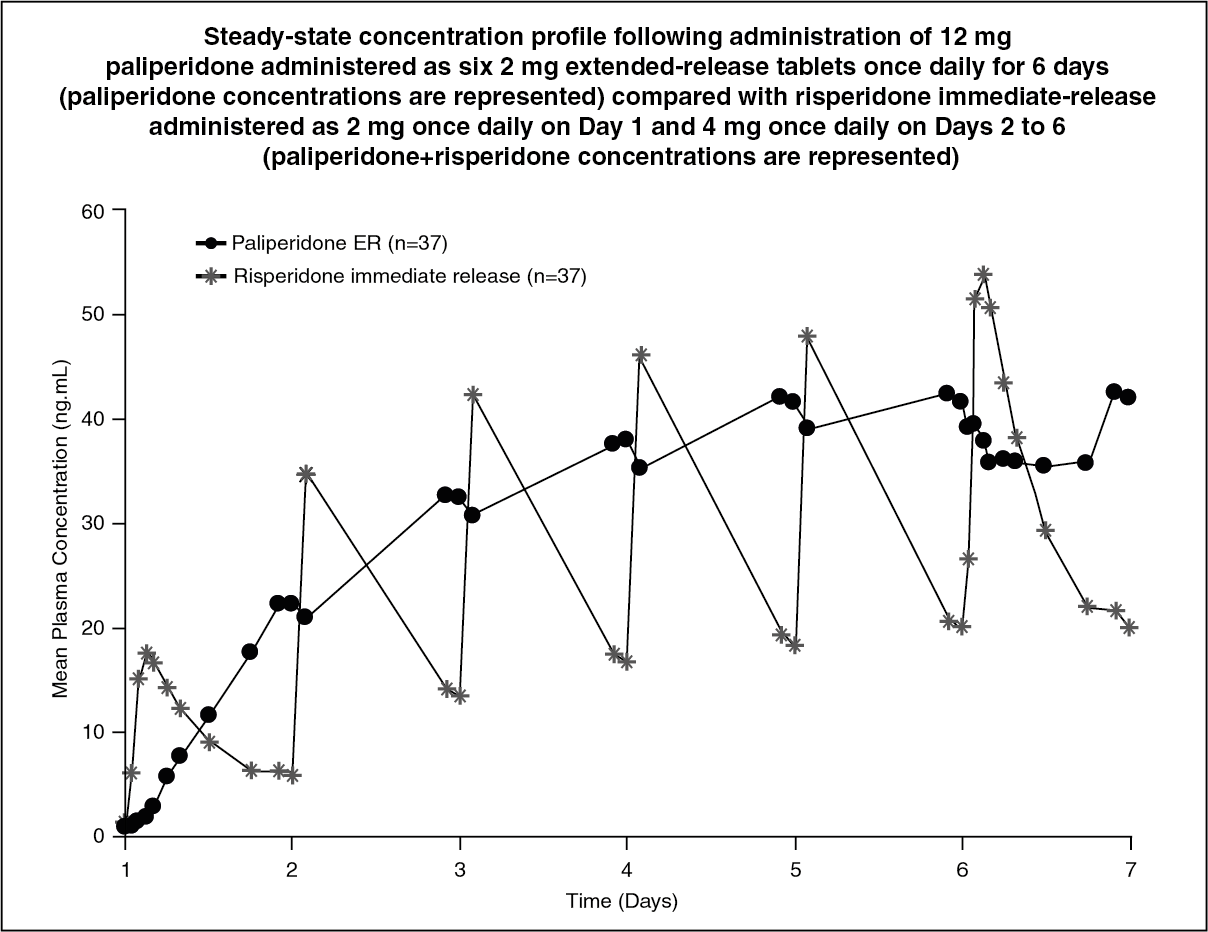
Absorption: Following a single dose of INVEGA, the plasma concentrations of paliperidone steadily rise to reach peak plasma concentration (C
max) in approximately 24 hours after dosing. With once-daily dosing of INVEGA, steady-state concentrations of paliperidone are attained within 4 - 5 days of dosing in most subjects.
The release characteristics of INVEGA result in minimal peak-trough fluctuations as compared to those observed with immediate-release risperidone. In a study comparing the steady-state pharmacokinetics following once-daily administration of 12 mg paliperidone (administered as extended-release tablets) with 4 mg immediate-release risperidone in schizophrenic subjects, the fluctuation indexes were 38% for paliperidone extended-release compared to 125% for risperidone immediate-release (see Figure 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following administration of INVEGA, the (+) and (-) enantiomers of paliperidone interconvert, reaching an AUC (+) to (-) ratio of approximately 1.6 at steady state. The absolute oral bioavailability of paliperidone following INVEGA administration is 28%.
Following administration of a single 15 mg paliperidone extended-release tablet to healthy subjects, confined to bed for 36 hours, with a standard high-fat/high-caloric meal, the C
max and AUC values increased by 42% and 46%, respectively, compared with administration under fasting conditions. In another study involving healthy ambulatory subjects, the C
max and AUC of paliperidone following administration of a single 12 mg paliperidone extended-release tablet with a standard high-fat/high-caloric meal resulted in increases of 60% and 54%, respectively, compared with administration under fasting conditions. Although the presence or absence of food at the time of INVEGA administration may increase or decrease exposure to paliperidone, these changes are not considered clinically relevant. Clinical trials establishing the safety and efficacy of INVEGA were carried out in subjects without regard to the timing of meals. (See Dosage & Administration).
Distribution: Paliperidone is rapidly distributed. The apparent volume of distribution is 487 L. The plasma protein binding of paliperidone is 74%. It binds primarily to α1-acid glycoprotein and albumin.
In vitro, high therapeutic concentrations of diazepam (3 mcg/mL), sulfamethazine (100 mcg/mL), warfarin (10 mcg/mL), and carbamazepine (10 mcg/mL) caused a slight increase in the free fraction of paliperidone at 50 ng/mL. These changes are not expected to be of clinical significance.
Metabolism and Elimination: One week following administration of a single oral dose of 1 mg immediate-release
14C-paliperidone, 59% of the dose was excreted unchanged into urine, indicating that paliperidone is not extensively metabolized in the liver. Approximately 80% of the administered radioactivity was recovered in urine and 11% in the feces. Four metabolic pathways have been identified
in vivo, none of which accounted for more than 6.5% of the dose: dealkylation, hydroxylation, dehydrogenation, and benzisoxazole scission. Although
in vitro studies suggested a role for CYP2D6 and CYP3A4 in the metabolism of paliperidone, there is no evidence
in vivo that these isozymes play a significant role in the metabolism of paliperidone. Despite the large variation in the general population with regard to the ability to metabolize CYP2D6 substrates, population pharmacokinetics analyses indicated no discernible difference on the apparent clearance of paliperidone after administration of INVEGA between extensive metabolizers and poor metabolizers of CYP2D6 substrates.
In vitro studies using microsomal preparations of heterologous systems indicate that CYP1A2, CYP2A6, CYP2C9, CYP2C19, and CYP3A5 are not involved in the metabolism of paliperidone. The terminal elimination half-life of paliperidone is about 23 hours.
Special Populations: Adolescents: Paliperidone systemic exposure in adolescent subjects was comparable to that in adults. In adolescents weighing < 51 kg (< 112 lbs), a 23% higher exposure was observed than in adolescents weighing ≥ 51 kg (≥ 112 lbs); this is considered not to be clinically significant. Age alone did not influence the paliperidone exposure.
Elderly: Data from a pharmacokinetic study in elderly subjects (≥ 65 years of age, n = 26) indicated that the apparent steady-state clearance of paliperidone following INVEGA administration was 20% lower compared to that of adult subjects (18 - 45 years of age, n = 28). However, there was no discernable effect of age in the population pharmacokinetic analysis involving schizophrenia subjects after correction of age-related decreases in CrCl.
Renal Impairment: The dose should be reduced in patients with moderate and severe renal impairment (see Dosage & Administration). The disposition of paliperidone was studied in subjects with varying degrees of renal function. Elimination of paliperidone decreased with decreasing creatinine clearance (CrCl). Total clearance of paliperidone was reduced in subjects with impaired renal function by 32% in mild (CrCl = 50 to < 80 mL/min), 64% in moderate (CrCl = 30 to < 50 mL/min), and 71% in severe (CrCl = 10 to < 30 mL/min) renal impairment. The mean terminal elimination half-life of paliperidone was 24, 40, and 51 hours in subjects with mild, moderate, and severe renal impairment, respectively, compared with 23 hours in subjects with normal renal function (CrCl ≥ 80 mL/min).
Hepatic Impairment: Paliperidone is not extensively metabolized in the liver. In a study in subjects with moderate hepatic impairment (Child-Pugh class B), the plasma concentrations of free paliperidone were similar to those of healthy subjects. Paliperidone has not been studied in patients with severe hepatic impairment.
Race: No dosage adjustment is recommended based on race. Population pharmacokinetics analysis revealed no evidence of race-related differences in the pharmacokinetics of paliperidone following INVEGA administration. No differences in pharmacokinetics were observed in a pharmacokinetics study conducted in Japanese and Caucasian subjects.
Gender: The apparent clearance of paliperidone following INVEGA administration is approximately 19% lower in women than men. This difference is largely explained by differences in lean body mass and creatinine clearance between men and women, as a population pharmacokinetics evaluation revealed no evidence of clinically significant gender-related differences in the pharmacokinetics of paliperidone following INVEGA administration after correction for lean body mass and creatinine clearance.
Smoking Status: Based on
in vitro studies utilizing human liver enzymes, paliperidone is not a substrate for CYP1A2; smoking should, therefore, not have an effect on the pharmacokinetics of paliperidone. Consistent with these
in vitro results, population pharmacokinetic evaluation has not revealed any differences between smokers and non-smokers.
Toxicology: Non-Clinical Information: As with other drugs that antagonize dopamine D
2 receptors, paliperidone elevated serum prolactin levels in repeat-dose toxicity studies.
In a 7-week juvenile toxicity study with oral doses of paliperidone of 0.16, 0.63, and 2.5 mg/kg/day, which are 0.12, 0.5, and 1.8 times the maximum recommended human dose of 12 mg/day for adolescents on a mg/m2 basis, no effects on growth, sexual maturation, and reproductive performance were observed. Doses up to 2.5 mg/kg/day did not impair neurobehavioral development in males and females, except for an effect on learning and memory in female rats treated at 2.5 mg/kg/day. This effect was not observed after discontinuation of treatment.
In a 40-week study in juvenile dogs treated with oral risperidone (which is extensively converted to paliperidone) at doses of 0.31, 1.25, and 5 mg/kg/day, sexual maturation was not adversely affected at 0.31 and 1.25 mg/kg/day. Long bone growth was not affected at 0.31 mg/kg/day; effects were observed at 1.25 and 5 mg/kg/day.
Carcinogenicity: The carcinogenic potential of paliperidone, an active metabolite of risperidone, was assessed based on studies with risperidone conducted in mice and rats. Risperidone was administered at doses up to 10 mg/kg/day for 18 months to mice and for 25 months to rats. There were statistically significant increases in pituitary gland adenomas, endocrine pancreas adenomas, and mammary gland adenocarcinomas. An increase in mammary, pituitary, and endocrine pancreas tumors has been found in rodents after chronic administration of other antipsychotic drugs and is considered to be mediated by prolonged dopamine D
2 antagonism. The relevance of these tumor findings in rodents in terms of human risk is unknown.
Mutagenicity: No evidence of mutagenic potential for paliperidone was found in the Ames reverse mutation test, the mouse lymphoma assay, or the rat micronucleus test.
Fertility: Although paliperidone treatment resulted in prolactin- and CNS-mediated effects, the fertility of male and female rats was not affected. At a maternally toxic dose, female rats showed a slightly lower number of live embryos.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image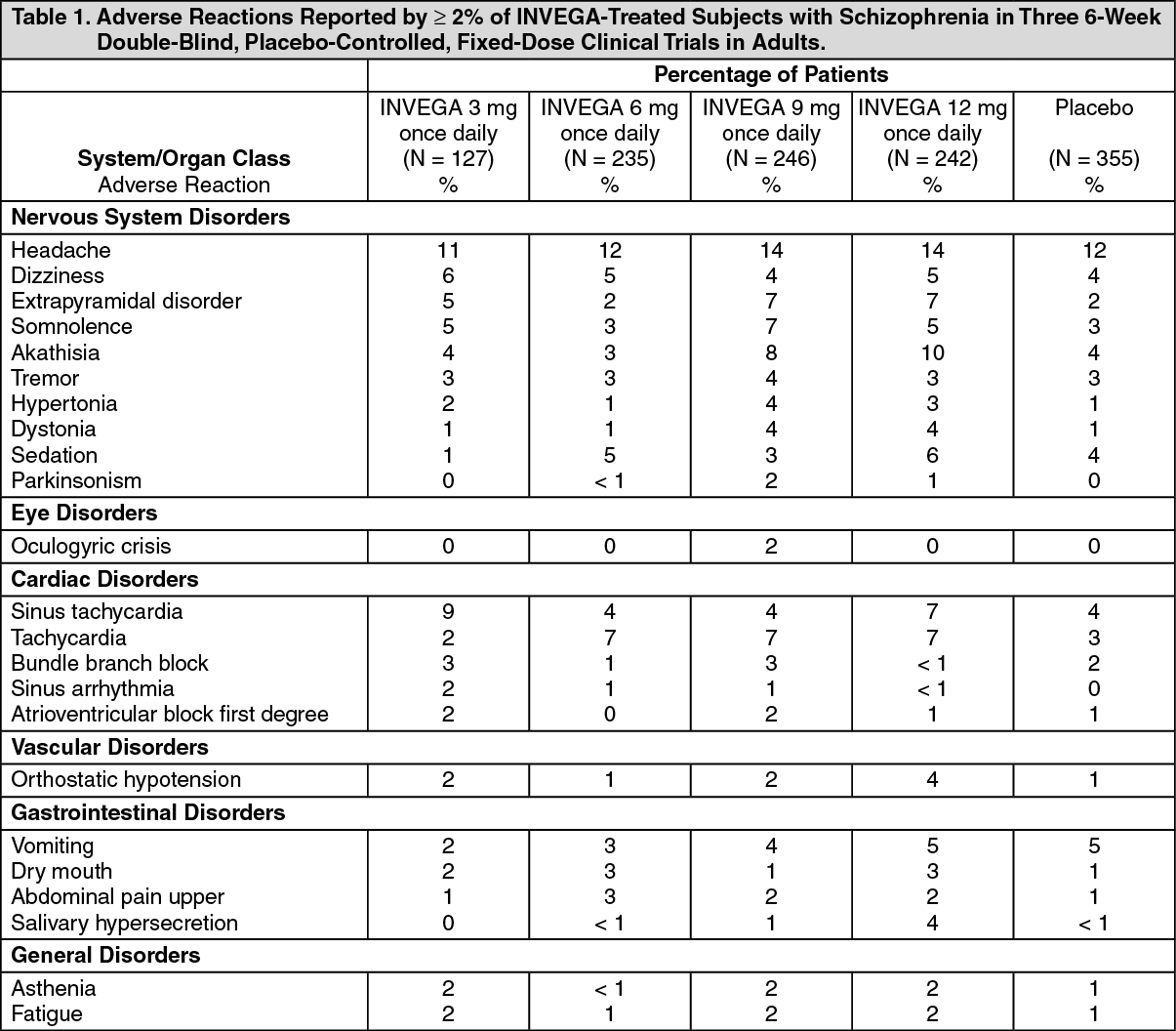 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image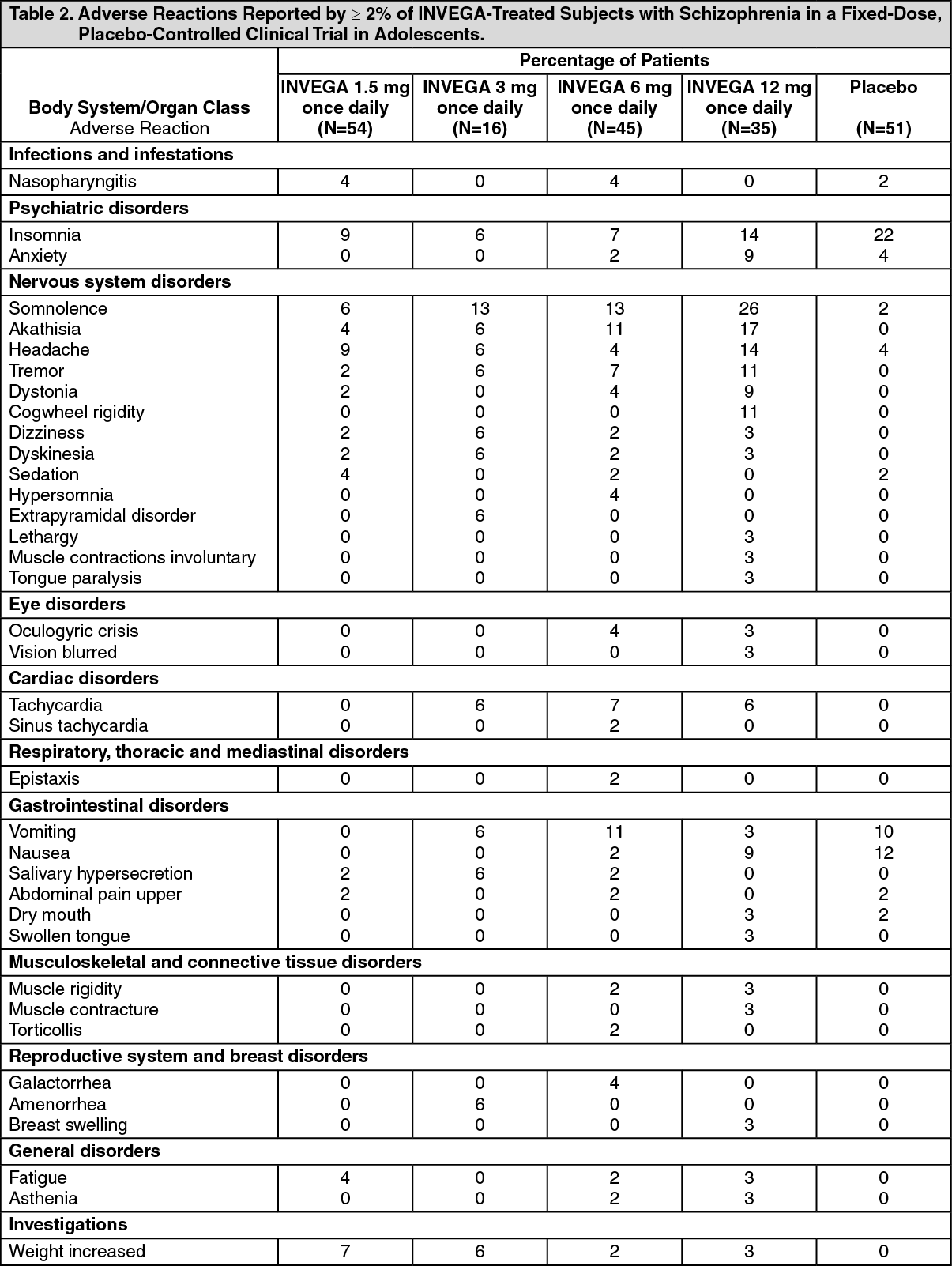 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image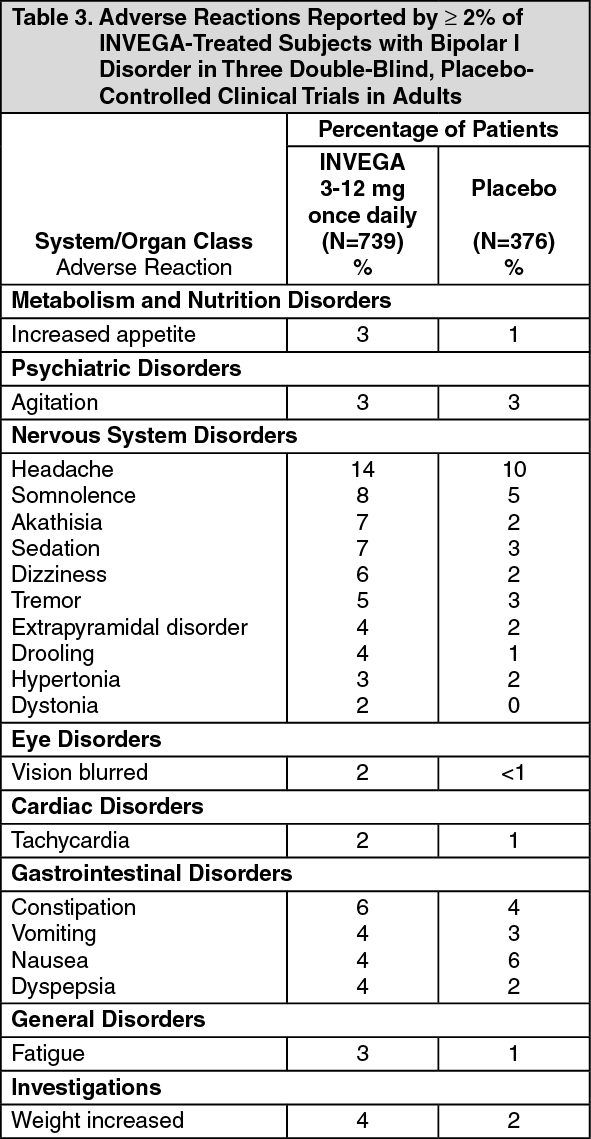 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image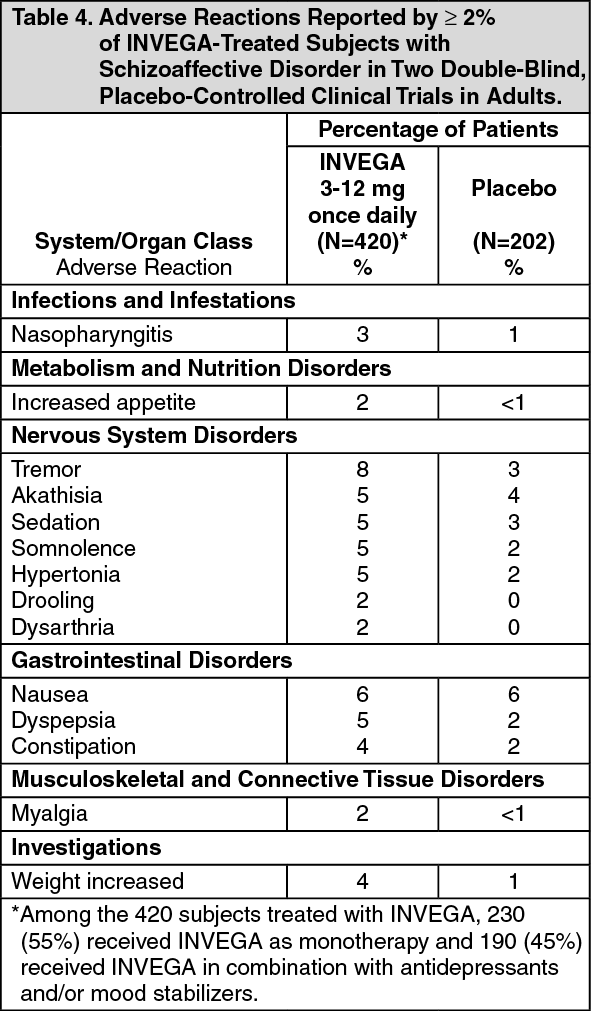 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
