


 Sign Out
Sign Out


Clinical Trial Data: The safety of INVEGA in the treatment of schizophrenia was evaluated in 1205 adult subjects with schizophrenia who participated in 3 double-blind, placebo-controlled 6-week trials, of whom 850 subjects received INVEGA at fixed doses ranging from 3 mg to 12 mg once daily.
The safety of INVEGA was evaluated in 314 adolescent subjects 12-17 years of age with schizophrenia who received INVEGA in the dose range of 1.5 mg to 12 mg/day in two Phase 3 studies, including 201 subjects in a 6-week, double-blind, placebo-controlled trial and subjects treated for up to 2 years in an open-label, single-arm safety trial.
The safety of INVEGA in the treatment of acute manic and mixed episodes associated with bipolar I disorder was evaluated in a total of 3 clinical trials in adults (n = 1257). The conditions and duration of treatment with INVEGA varied across these studies and included (in overlapping categories) placebo- and active-controlled, double-blind, and fixed- and flexible-dose studies. Of the 1257 adult subjects, 739 subjects received INVEGA in the dose range of 3 mg to 12 mg once daily and 376 subjects received placebo.
The safety of INVEGA was also evaluated in 622 adult subjects with schizoaffective disorder who participated in two double-blind, placebo-controlled, 6-week trials. In one of these trials, 206 subjects were assigned to one of two dose levels of INVEGA 6 mg with the option to reduce to 3 mg (n = 108) or 12 mg with the option to reduce to 9 mg (n = 98) once daily. In the other study, 214 subjects received flexible doses of INVEGA (3-12 mg once daily). Both studies included subjects who received INVEGA either as monotherapy or in combination with antidepressants and/or mood stabilizers.
The information in this section was derived from pooled data.
The majority of adverse reactions were mild to moderate in severity.
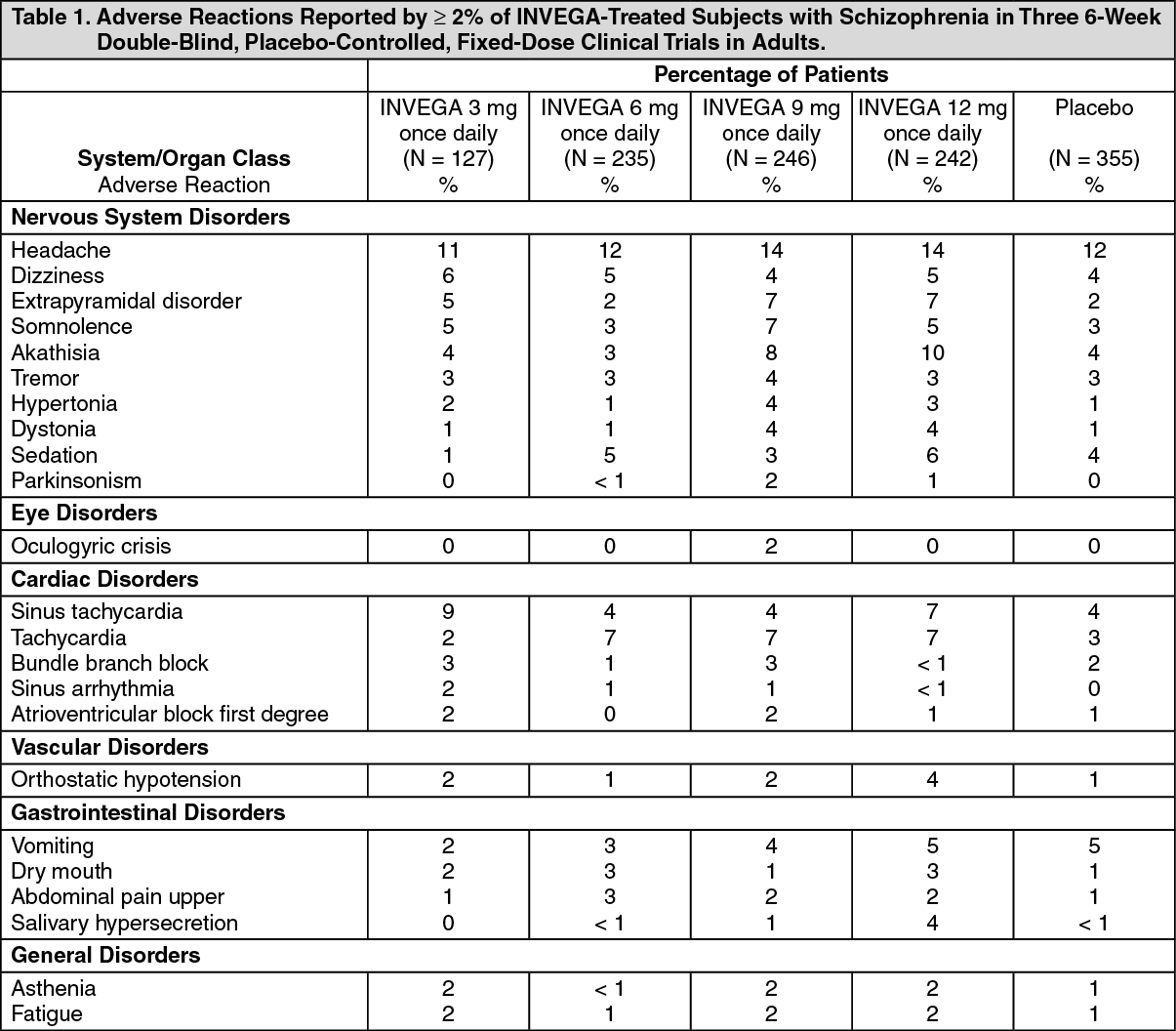
Double-Blind, Placebo-Controlled Data - Schizophrenia - adults: Adverse reactions reported by ≥ 2% of INVEGA-treated subjects in the three 6-week double-blind, placebo-controlled, fixed-dose schizophrenia trials in adults are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
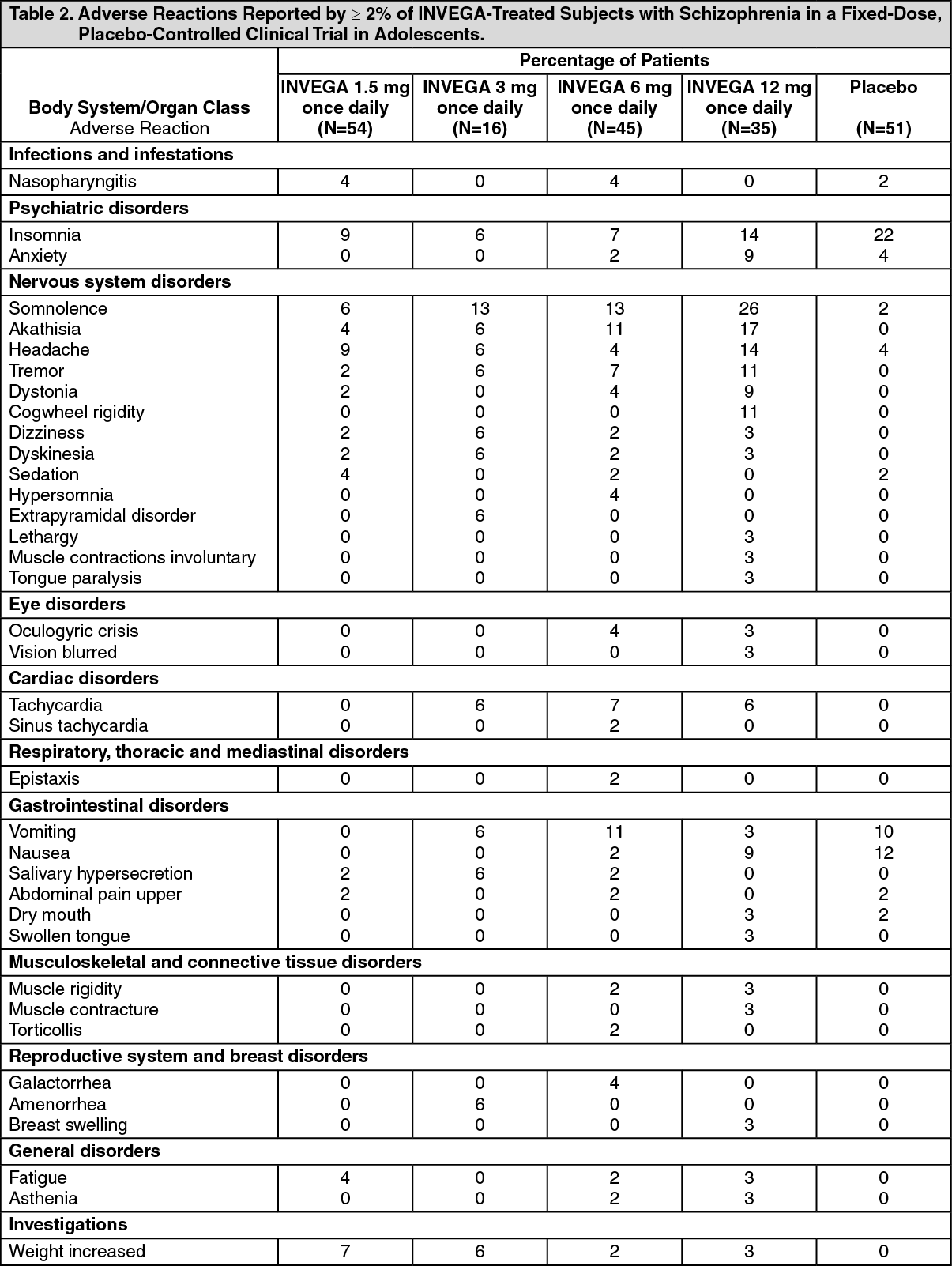
Click on icon to see table/diagram/imageDouble-Blind, Placebo-Controlled Data - Schizophrenia - Adolescents: Adverse reactions reported by ≥ 2% of INVEGA-treated adolescent subjects 12-17 years of age with schizophrenia in a fixed-dose, placebo-controlled study are shown in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
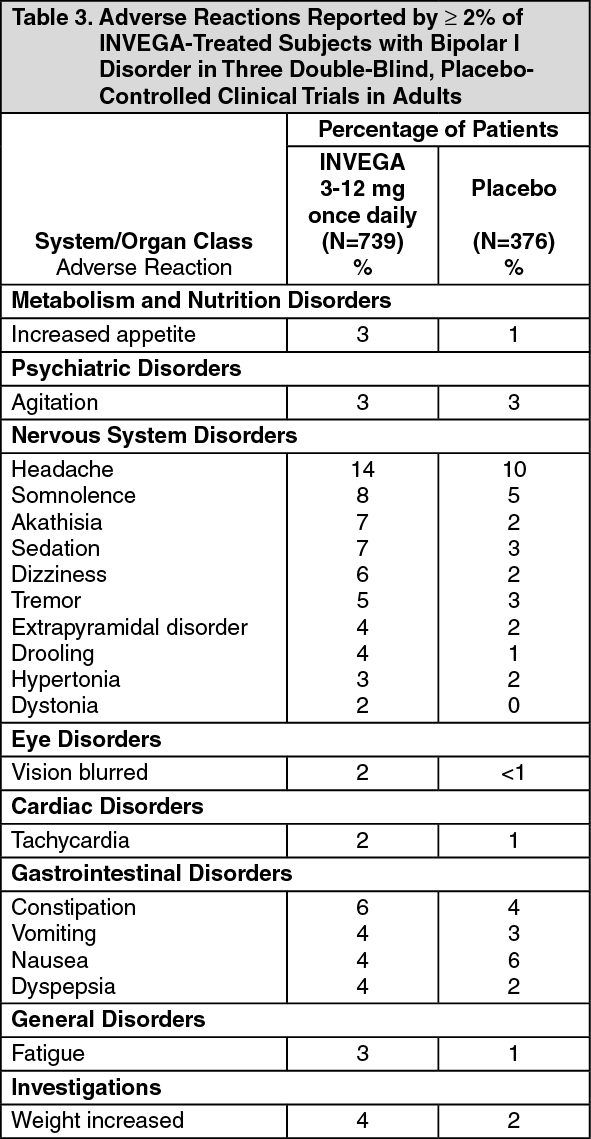
Click on icon to see table/diagram/imageDouble-Blind, Placebo-Controlled Data - Bipolar Disorder - Adults: Adverse reactions reported by ≥ 2% of INVEGA-treated subjects in the three double-blind, placebo-controlled bipolar disorder trials in adults are shown in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
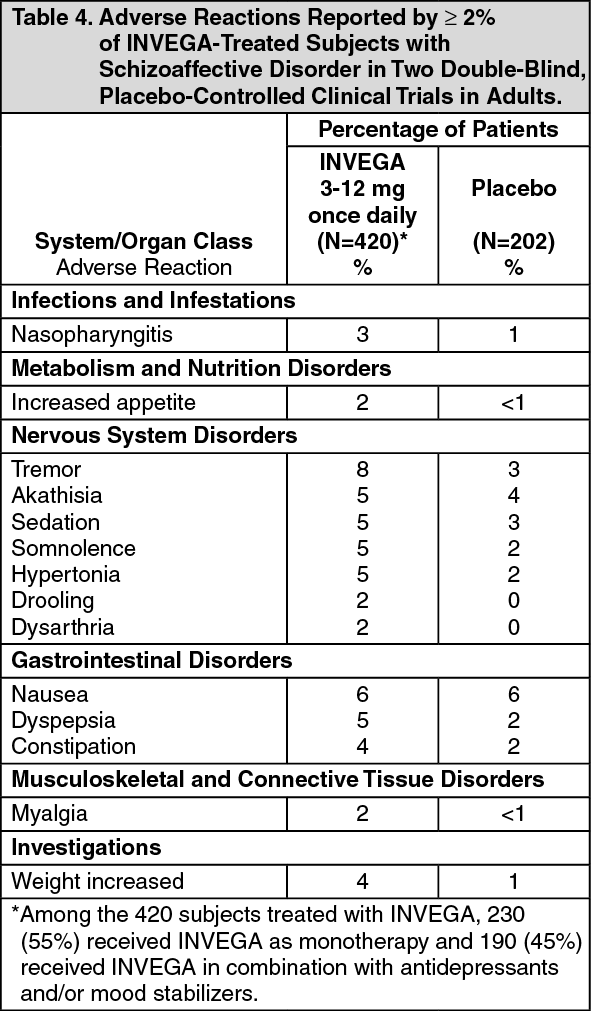
Click on icon to see table/diagram/imageDouble-Blind, Placebo-Controlled Data - Schizoaffective Disorder - Adults: Adverse reactions reported by ≥ 2% of INVEGA-treated subjects in the two placebo-controlled schizoaffective disorder trials in adults are shown in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMonotherapy versus Combination Therapy: The designs of the two placebo-controlled, 6-week, double-blind trials in adult subjects with schizoaffective disorder included the option for subjects to receive antidepressants (except monoamine oxidase inhibitors) and/or mood stabilizers (lithium, valproate, or lamotrigine). In the subject population evaluated for safety, 230 (55%) subjects received INVEGA as monotherapy and 190 (45%) subjects received INVEGA in combination with antidepressants and/or mood stabilizers. When comparing these 2 subpopulations, only nausea occurred at a greater frequency (≥3% difference) in subjects receiving INVEGA as monotherapy.
Dose-Related Adverse Reactions: In the placebo-controlled, 6-week high- and low-dose study in adult subjects with schizoaffective disorder, dystonia, dysarthria, and nasopharyngitis occurred more frequently (i.e., a difference of at least 3%) in subjects who received higher doses of INVEGA compared with subjects who received lower doses. Hypertonia occurred more frequently in subjects who received lower doses of INVEGA compared with subjects who received higher doses.
Other Clinical Trial Data: Paliperidone is the active metabolite of risperidone, therefore the adverse reaction profiles of these compounds (including both the oral and injectable formulations) are relevant to one another. This subsection includes additional Adverse reactions reported with paliperidone and/or risperidone in clinical trials.
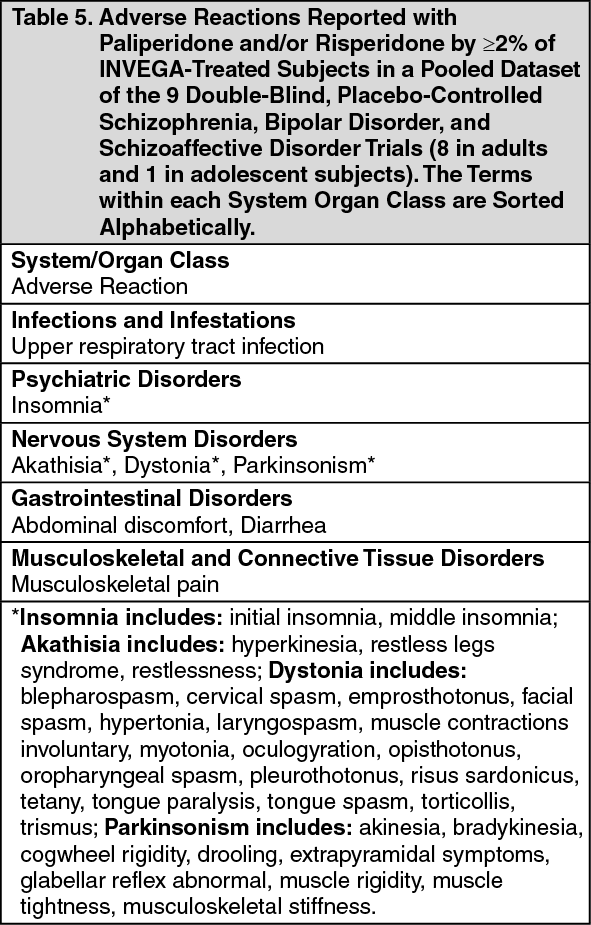
Adverse reactions reported with paliperidone and/or risperidone by ≥ 2% of INVEGA-treated subjects in a pooled dataset of the 9 double-blind, placebo-controlled schizophrenia, bipolar disorder, and schizoaffective disorder trials (8 in adults and 1 in adolescent subjects) are shown in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdverse reactions reported with paliperidone and/or risperidone by <2% of INVEGA-treated subjects in a pooled dataset of the 9 double-blind, placebo-controlled schizophrenia, bipolar disorder, and schizoaffective disorder trials (8 in adults and 1 in adolescent subjects) are shown in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
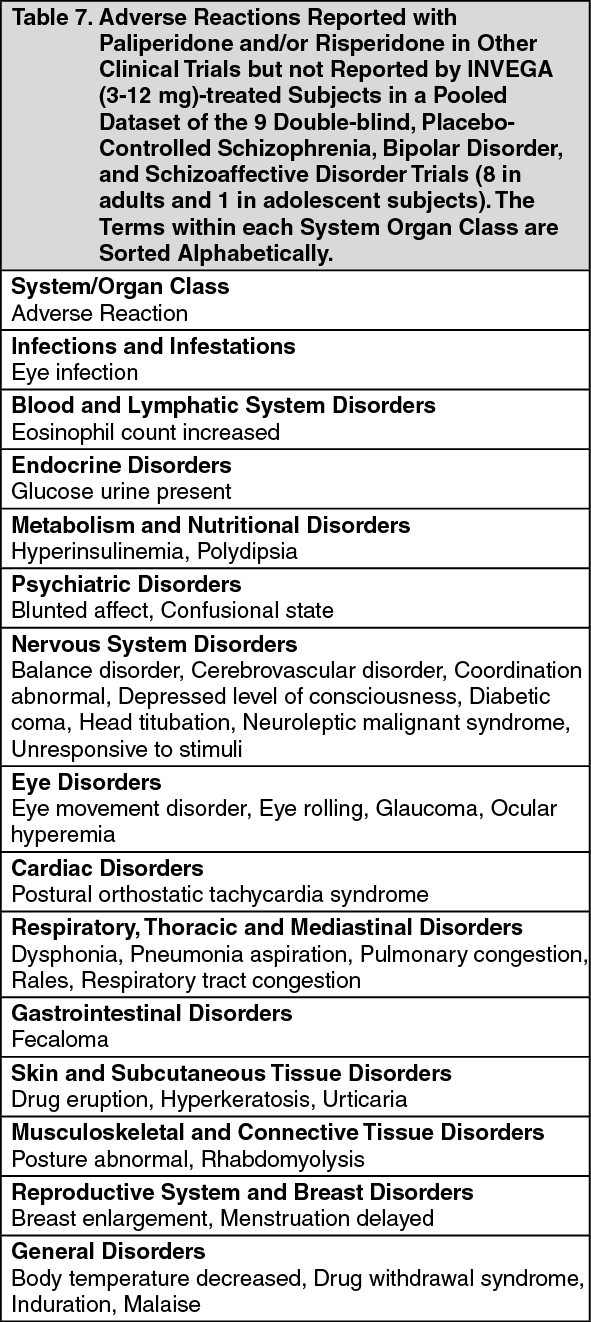
Click on icon to see table/diagram/imageAdverse reactions reported with paliperidone and/or risperidone in other clinical trials but not reported by INVEGA (3-12 mg)-treated subjects in a pooled dataset of the 9 double-blind, placebo-controlled schizophrenia, bipolar disorder, and schizoaffective disorder trials (8 in adults and 1 in adolescent subjects) are shown in Table 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageElderly: The safety of INVEGA was evaluated in 81 elderly subjects with schizophrenia (65 years of age and older) who received either flexible doses (n = 76) or fixed doses (n = 5) of INVEGA in a range of 3 to 12 mg once daily for a duration of up to 6 weeks during double-blind, placebo-controlled trials. Although this dataset does not allow for a systematic direct comparison between elderly and non-elderly subjects, the safety profile was similar in the two populations. However, based on these limited data and consistent with general clinical practice, a greater sensitivity of older individuals to adverse reactions cannot be ruled out.
Events of Particular Interest to the Class: Extrapyramidal Symptoms (EPS). Pooled data from the three 6-week double-blind, placebo-controlled, fixed-dose schizophrenia studies (see Pharmacology: Pharmacodynamic: Clinical Efficacy under Actions) showed no differences in treatment-emergent EPS between placebo (11%) and INVEGA 3 and 6 mg doses (13% and 10%, respectively). Dose-relatedness for EPS was seen with the two higher doses of INVEGA (25% and 26% for the 9 and 12 mg doses, respectively). EPS included a pooled analysis of the following terms: dyskinesia, dystonia, hyperkinesia, Parkinsonism, and tremor. Pooled data from the two 6-week, double-blind, placebo-controlled studies in subjects with schizoaffective disorder (see Pharmacology: Pharmacodynamics: Clinical Efficacy under Actions) showed similar results.
Weight Gain: In the pooled data from the three placebo-controlled, 6-week, fixed-dose adult schizophrenia studies (see Pharmacology: Pharmacodynamics: Clinical Efficacy under Actions), the proportions of subjects meeting a weight gain criterion of ≥ 7% of body weight were compared, revealing a similar incidence of weight gain for INVEGA 3 mg and 6 mg (7% and 6%, respectively) compared with placebo (5%), and a higher incidence of weight gain for INVEGA 9 mg and 12 mg (9% and 9%, respectively).
Weight gain in adolescent subjects with schizophrenia was assessed in a 6-week, double-blind, placebo-controlled study and an open-label extension with a median duration of exposure to INVEGA of 182 days. In the double-blind, placebo-controlled study, a higher percentage of INVEGA low dose (6%), medium dose (13%), and high dose (13%) treated subjects [see Pharmacology: Pharmacodynamic under Actions] had an increase in body weight of ≥ 7% from baseline compared with placebo-treated subjects (2%). In the open-label long-term study the proportion of total subjects treated with INVEGA with an increase in body weight of ≥ 7% from baseline was 33%. When treating adolescent patients with INVEGA, weight gain should be assessed against that expected with normal growth. When taking into consideration the median duration of exposure to INVEGA in the open-label study (182 days) along with expected normal growth in this population, an assessment of standardized scores relative to normative data provides a more clinically relevant measure of changes in weight. The mean change from open-label baseline to endpoint in standardized score for weight was 0.1 (4% above the median of normative data). Based on comparison to the normative data, these changes are not considered to be clinically significant.
In the pooled data from the two placebo-controlled, 6-week studies in adult subjects with schizoaffective disorder (see Pharmacology: Pharmacodynamics: Clinical Efficacy under Actions), a higher percentage of INVEGA-treated subjects (5%) had an increase in body weight of ≥ 7% compared with placebo-treated subjects (1%). In the study that examined high- and low-dose groups, the increase in body weight of ≥ 7% was 3% in the low-dose group, 7% in the high-dose group, and 1% in the placebo group.
Laboratory Tests: Serum Prolactin. Based on pooled data from the three 6-week double-blind, placebo-controlled, fixed-dose schizophrenia studies (see Pharmacology: Pharmacodynamics: Clinical Efficacy under Actions), increases in serum prolactin were observed in subjects of both genders who received INVEGA. Maximum mean increases of serum prolactin concentrations were generally observed on Day 15 of treatment, but remained above baseline levels at study endpoint.
Clinical Trials: Adverse reactions in a Long-Term, Placebo-Controlled Study: The safety of INVEGA was also evaluated in a long-term trial designed to assess the maintenance of effect with INVEGA in adults with schizophrenia (see Pharmacology: Pharmacodynamics: Clinical Efficacy under Actions). In general, the types, frequencies, and severities of adverse reactions reported during the initial 14-week open-label phase of this study were comparable to those reported in the 6-week, placebo-controlled, fixed-dose studies. The adverse reactions reported during the long-term double-blind phase of this study were similar in type and severity to those observed in the initial 14-week open-label phase, but occurred at generally lower frequencies.
Postmarketing Data: In addition to the adverse reactions reported during clinical trials and listed previously, the following adverse reactions have been reported during postmarketing experience with paliperidone and/or risperidone (Table 8). In the table, the frequencies are provided according to the following convention: Very common: ≥ 1/10, Common: ≥ 1/100 and < 1/10, Uncommon: ≥ 1/1000 and < 1/100, Rare: ≥ 1/10000 and < 1/1000, Very rare: < 1/10000, including isolated reports, Not known: Cannot be estimated from the available data.
In Table 8, adverse reactions are presented by frequency category based on spontaneous reporting rates, when known. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form