Each tablet contains Metformin Hydrochloride 500mg.
Pharmacology: Pharmacodynamics: Metformin hydrochloride does not stimulate pancreatic beta cells of insulin; insulin secretion must be present for metformin to work properly. Metformin hydrochloride may increase the number and/or affinity of insulin receptors on cell surface membranes, especially at peripheral receptor sites, and help to correct down regulation of the insulin receptor. This effect increases the sensitivity to insulin at receptor and post receptor binding sites and increases uptake peripherally. Insulin concentrations remain unchanged or are slightly reduced as glucose metabolism improves. In addition, metformin's metabolic effects increase hepatic glycogen stores in diabetic patients (but not in non-diabetic patients). Decrease intestinal glucose absorption, and reduce fatty acid oxidation and acetyl co-enzyme A formation. Glucose uptake or free fatty acid oxidation is effects considered to be caused by non-insulin mediated mechanisms.
Pharmacokinetics: Metformin hydrochloride is absorbed over a period of 6 hours with bioavailability between 50%-60% under fasting condition. Presence of food will delay the absorption, lowers the peak concentration by 40% and decreases the bioavailability by 25%. Peak serum concentration at steady state is 1 to 2 mcg/ml, achieved within 2 hours. The main sites of concentration without accumulation are the intestinal mucosa and the salivary glands; also, the erythrocyte mass may be a compartment of distribution. It has a plasma half-life of about 3 hours and it is not bound to plasma proteins. Metformin hydrochloride does not undergo hepatic metabolism and up to 90% of a dose of metformin is excreted unchanged in the urine. About 30% of a dose is eliminated in the feces. Haemodialysis with a clearance of 170 ml/minute prevents accumulation of metformin.
Metformin hydrochloride is indicated in non-insulin-dependent diabetes mellitus (NIDDM) patients to control hyperglycemia that cannot be controlled by diet management, exercise or
weight reduction. It can be used as a monotherapy or as an adjunct to sulfonylureas. Caution and clinical judgement should be used when combining metformin with maximum doses
sulfonylureas for treating non-obese NIDDM patients who clearly are not responding to the sulfonylureas when insulin may be the preferred treatment.
Adult: 500 mg thrice daily with meals, gradually increased if necessary to a maximum of 3 g daily.
Pediatric: Safety and efficacy have not been established.
Geriatrics: Usual adult dose. For some sensitive individuals, lower initial doses may be needed. Maximum doses are not advised for the use in the elderly.
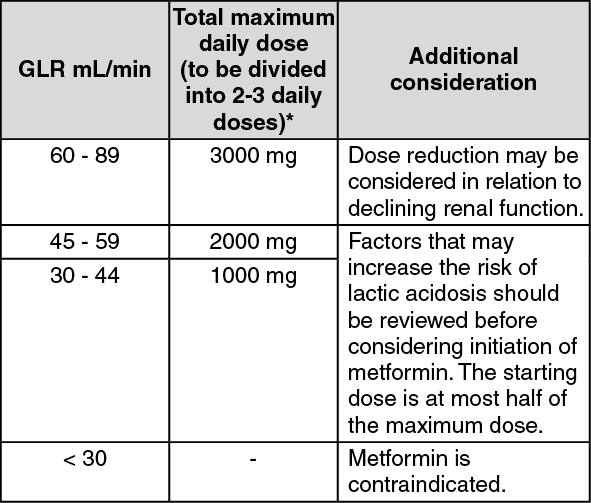
Renal impairment: A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months. (See table.)
 Click on icon to see table/diagram/image
Route of Administration:
Click on icon to see table/diagram/image
Route of Administration: For oral use.
Overdosage of metformin produces hypoglycemia and lactic acidosis.
Hemodialysis with sodium bicarbonate has been used but is controversial because there is a lack of published information concerning outcome and lack of cases of metformin-induced lactic acidosis; peritoneal dialysis also has been used, but hemodialysis is thought to be the preferred method when dialysis is needed, such as in patients with shock syndrome. Dialysis is probably not necessary when renal function could be restored because of metformin's rapid renal elimination. Dialysis solutions commonly contain lactate as the buffering agent and these should not be used in cases of metformin-induced lactic acidosis.
Mild to moderate hypoglycaemia is treated with immediate digestion of a source of sugar, such as glucose gel, glucose tablets, fruit juice, non-diet soft drinks, honey, sugar cubes, or table sugar dissolved in water. A frequently used source of sugar is a glassful of orange juice. Blood glucose should be checked every 15 minutes. Patient should be advised to seek medical assistance promptly. There may be a need to adjust dosage of metforrnin or meal pattern.
Severe hypoglycaemia or acute overdose, including coma, requires emergency medical assistance immediately. Dextrose 50% is given intravenously to stabilise the patient. Then, administer a continuous infusion of 5%-10% dextrose in water to maintain slight hyperglycaemia for up to 12 days. Glucagon, 1-2 mg administered intramuscularly, is useful for fast onset of action to mobilise hepatic glucose stores but may be ineffective or variable in its effect if glycogen stores are depleted and must follow the use of glucose. Diazoxide therapy can be used for nonresponders to glucose therapy or for patients in a coma as an aid to glucose infusion to reduce hypoglycaemia; patient should be monitored for sodium concentration and for hypotension. Emesis can be induced with syrup of ipecac if overdose is recent (within the past 30 minutes) if patient is alert, has an intact gag reflex, and is not obtunded or convulsing. Otherwise, gastric lavage after endotracheal tube placement is required. Vital signs, arterial blood gases, blood glucose, and serum electrolytes (especially calcium, potassium, and sodium) should be monitored as required. Initially, blood glucose concentrations should be monitored as frequently as every 1-3 hours. Blood urea nitrogen and serum creatinine concentrations should also be obtained. Cerebral edema can be managed with mannitol and dexamethasone while patients with hypokalaemia should be given potassium supplements. Patient should be hospitalised for 6-91 hours (mean, 24 hours) because the hypoglycaemia may be recurrent and prolonged. Other supportive measures should also be employed as needed.
Up-to-date information on treatment of overdose can be obtained from The National Poison Centre, Universiti Sains Malaysia.
Severely reduced kidney function (GFR <30 mL/min); Any type of acute metabolic acidosis (such as lactic acidosis, diabetic ketoacidosis); Metformin hydrochloride should not be used in patients with hypersensitivity to metformin.
It is also contraindicated whenever there is any condition needing close blood glucose control, such as severe burns, dehydration, diabetic coma, diabetic ketoacidosis, hyperosmolar nonketotic coma, severe infection, major surgery and severe trauma. Blood glucose is best controlled with insulin in these conditions. There is a higher risk of lactic acidosis when metformin is used in severe hepatic disease, renal disease, shock, pulmonary insufficiency, dehydration, alcoholism and conditions associated with hypoxaemia such as cardiorespiratory insufficiency, cardiovascular collapse, congestive heart failure and acute myocardial infarction. It should not be given to patients undergoing diagnostic or medical examinations using contrast media such as angiography and pyelography.
Metformin hydrochloride should be used with care in conditions that decrease or delay stomach emptying such as diarrhoea, gastroparesis, intestinal obstruction, vomiting or other conditions cause delayed food absorption. Female hormonal changes, high fever, hypercortisolism and psychological stress may predispose to hyperglycaemia while adrenal insufficiency, debilitated physical condition, malnutrition and pituitary insufficiency inherently predispose patients to the risk of developing hypoglycaemia. These conditions warrant a need for more frequent glucose monitoring and for a temporary or permanent adjustment of metformin dosages. Hyperthyroidism aggravates diabetes mellitus by increasing plasma glucose concentrations and glucose absorption and impairing glucose tolerance while hypothyroidism is associated with reduced glucose absorption and altered glucose and lipoprotein metabolism. Glycaemic control may be difficult until the patient is euthyroid.
Serum folic acid and Vitamin B12 concentration determinations are recommended every 1-2 years during long-term metformin therapy because metformin may interfere with their absorption serum glucose concentration should be routinely self-monitored by the patients at home (several times a day or once to several times a week) and by the physicians (every 3 months or more often when patient is not stabilized). Monitoring of urine for the presence of glucose and ketones may be necessary if blood glucose levels exceed 200 mg/dL. Glycosylated hemoglobin (hemoglobin A) reflects the blood glucose control over the preceding 3 months. Monitoring of this parameter should be done every 3 months or as often as necessary; however this does not eliminate the need for daily blood glucose monitoring. Hemoglobin A is falsely elevated in unstable diabetics when the intermediate precursor is elevated (in alcoholism) and falsely lowered in conditions of shortened red blood cell lifespan (in anemia and acute or chronic blood loss) or in patients with hemoglobinopathies (sickle cell). Regular physical examinations are recommended as often as necessary to reassess appropriateness of continuation of metformin therapy. Renal function assessment is recommended annually, and more often for high risk patients.
Metformin hydrochloride may produce false positive diagnostic test results for ketones in urine. The effects of metformin on total serum cholesterol, serum low density lipoproteins and serum triglycerides in NIDDM patients are inconsistent and may depend on weight control. Generally, concentrations of these lipid subfractions may be lowered or unchanged in metformin users. This is thought to be independent of metformin's glucose lowering effect; it may involve suppression of free fatty acid oxidation and lipid oxidation or reduction in the triglyceride content of the LDL and VLDL fractions by metformin.
Serum high density lipoprotein (HDL) may be slightly increased or unchanged. Fasting serum lactate may increase to the upper range of normal, or to show no change with therapeutic doses; although the source is unknown, any small increase is thought to be due to glucose metabolism in the splanchnic beds, not in skeletal muscle.
Lactic acidosis: Lactic acidosis, a very rare but serious metabolic complication, most often occurs at acute worsening of renal function or cardiorespiratory illness or sepsis. Metformin accumulation occurs at acute worsening of renal function and increases the risk of lactic acidosis. In case of dehydration (severe diarrhoea or vomiting, fever or reduced fluid intake), metformin should be temporarily discontinued and contact with a health care professional is recommended. Medicinal products that can acutely impair renal function (such as antihypertensives, diuretics and NSAIDs) should be initiated with caution in metformin-treated patients. Other risk factors for lactic acidosis are excessive alcohol intake, hepatic insufficiency, inadequately controlled diabetes, ketosis, prolonged fasting and any conditions associated with hypoxia, as well as concomitant use of medicinal products that may cause lactic acidosis. Patients and/or care-givers should be informed of the risk of lactic acidosis. Lactic acidosis is characterised by acidotic dyspnoea, abdominal pain, muscle cramps, asthenia and hypothermia followed by coma. In case of suspected symptoms, the patient should stop taking metformin and seek immediate medical attention. Diagnostic laboratory findings are decreased blood pH (< 7.35), increased plasma lactate levels (>5 mmol/L) and an increased anion gap and lactate/pyruvate ratio.
Renal function: GFR should be assessed before treatment initiation and regularly there after [See Dosage & Administration]. Metformin is contraindicated in patients with GFR <30 mL/min and should be temporarily discontinued in the presence of conditions that alter renal function [See Contraindications].
Use in Pregnancy: Uncontrolled diabetes during pregnancy (gestational or permanent) is associated with increased risk of congenital abnormalities and perinatal mortality. When the patient plans to become pregnant and during pregnancy, it is recommended that diabetes is not treated with metformin but insulin to be used to maintain blood glucose levels as close to normal as possible, to reduce the risk of malformations of the foetus.
Use in Lactation: Metformin is excreted into human breast milk. No adverse effects were observed in breastfed newborns/infants. However, as only limited data are available, breast-feeding is not recommended during metformin treatment. A decision on whether to discontinue breast-feeding should be made, taking into account the benefit of breast- feeding and the potential risk to adverse effects on the child.
The most common side effects are anorexia, dyspepsia, flatulence, headache, metallic taste, nausea and vomiting as well as weight loss. Metformin interferes with the absorption of Vitamin B12 by competitive inhibition of calcium-dependant binding of the intrinsic factor-Vitamin B12 complex to its receptor; anemia in predisposed individuals may be possible. Rarely, megaloblastic anemia and hypoglycemia occur. However, hypoglycemia does not usually occur with use of metformin unless predisposing factors are present, such as unusual fasting, concurrent use of other antidiabetic agents, or toxic doses of metformin. Lactic acidosis is a potentially fatal complication. However, the risk is minimal with use of metformin unless in patients with contra-indications to therapy. Patients usually presented not with symptoms of lactic acidosis but rather with acute symptoms of other problems that resulted in metformin accumulation because of renal function impairment or failure and in conditions such as myocardial infarction or hepatic disease.
Excessive intake or chronic ingestion of alcohol may elevate blood lactate concentrations or increase the risk of developing hypoglycemia, especially when alcohol is ingested without meals. Cimetidine inhibits renal tubular secretion and thus increasing plasma metformin concentration. Other cationic medications excreted by renal tubular transport, such as amiloride, calcium channel blockers, digoxin, morphine, procainamide, quinidine, quinine, ranitidine, triamterene, trimethoprim and vancomycin have the potential to increase metformin's plasma concentration or interfere with renal clearance; careful monitoring of blood glucose would be appropriate. Oral contraceptives, corticosteroids, diuretics, estrogens, isoniazid, nicotinic acid, phenothiazines, phenytoin, sympathomimetics and thyroid hormones may contribute to hyperglycaemia while clofibrate, monoamine oxidase inhibitors, probenecid, propranolol, rifabutin, rifampicin, salicylates, sulfonamides and sulphonylureas may cause hypoglycaemia.
Store in a dry place below 30°C. Protect from light.
A10BA02 - metformin ; Belongs to the class of biguanides. Used in the treatment of diabetes.
Glucoxit tab 500 mg
10 × 10's;100 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
