General: Particular attention should be paid to the specific dosing instructions for each proprietary Low Molecular Weight Heparin, as different units of measurement (units or mg) are used to express doses. Nadroparin should therefore not be used interchangeably with other low molecular weight heparins during ongoing treatment. In addition, care should be taken to use the correct formulation of nadroparin, either single or double strength, as this will affect the dosing regimen.
Graduated syringes are intended for use when dose adjustment for body weight is necessary.
Platelet count must be monitored throughout nadroparin treatment (see Precautions).
Specific recommendations regarding the timing of nadroparin dosing surrounding spinal/epidural anaesthesia or spinal lumbar puncture should be followed (see Precautions).
Adults: Prophylaxis of Thromboembolic Disorders: General Surgery: The recommended dose of nadroparin is 0.3 ml (2,850 anti-Xa IU) administered subcutaneously 2 to 4 hours before surgery, and then once daily on subsequent days. Treatment should be continued for at least seven days, and throughout the risk period, until the patient is ambulant.
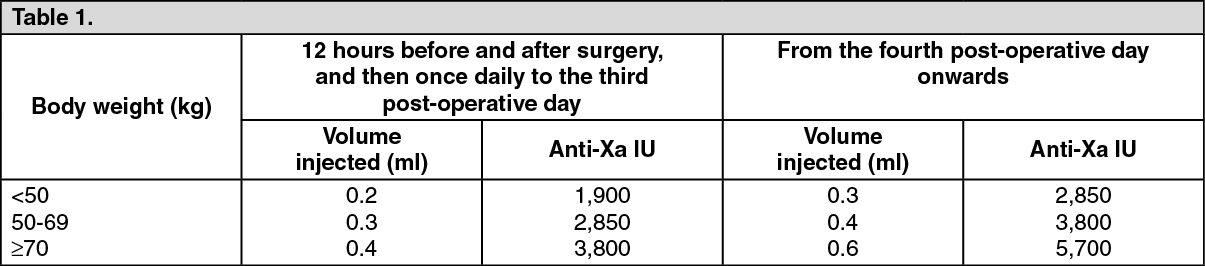
Orthopaedic Surgery: Nadroparin is administered subcutaneously and the dose is adjusted for body weight according to the table as follows. This is based on a target dose of 38 anti-Xa IU per kg body weight, and is increased by 50% on the fourth post-operative day. The initial dose is administered 12 hours before surgery and a second dose 12 hours after the end of surgery. Treatment is then continued once daily throughout the risk period and until the patient is ambulant. The minimum treatment period is 10 days. (See Table 1.)
 Click on icon to see table/diagram/image
High-risk medical patients (respiratory failure and/or respiratory infection and/or cardiac failure), immobilised due to acute illness or hospitalised in an intensive care unit:
Click on icon to see table/diagram/image
High-risk medical patients (respiratory failure and/or respiratory infection and/or cardiac failure), immobilised due to acute illness or hospitalised in an intensive care unit: Nadroparin is administered subcutaneously once daily. The dose should be adjusted for body weight according to the table as follows. Treatment should be continued throughout the risk period of thromboembolism. (See Table 2.)
Click on icon to see table/diagram/image
In elderly patients, dose reduction to 0.3 ml (2,850 Anti-Xa IU) may be appropriate.
Treatment of Thromboembolic Disorders: In the treatment of thromboembolic disorders, oral anticoagulant therapy should be initiated as soon as possible unless contraindicated. Treatment with nadroparin should not be stopped before the International Normalised Ratio target is reached.
It is recommended that nadroparin is administered subcutaneously twice daily (every 12 hours) for a usual duration of 10 days. The dose should be adjusted for body weight according to the table as follows, which is based on a target dose of 86 anti-Xa IU per kg body weight. (See Table 3.)
Click on icon to see table/diagram/image
Prevention of Clotting During Haemodialysis: In the prevention of clotting during haemodialysis, the dose of nadroparin must be optimised for each individual patient, also taking into account the technical conditions of the dialysis.
Nadroparin is usually given as a single dose into the arterial line at the start of each session. For patients without increased risk of haemorrhage the following initial doses are suggested according to body weight and are usually sufficient for a four hour session: (see Table 4.)
Click on icon to see table/diagram/image
Doses should be halved in patients with an increased risk of haemorrhage.
An additional smaller dose may be given during dialysis for sessions lasting longer than four hours. The dose in subsequent dialysis sessions should be adjusted as necessary according to the observed effect.
Patients should be carefully monitored throughout each dialysis session for signs of bleeding or clotting in the dialysis circuit.
Treatment of Unstable Angina and Non-Q Wave Myocardial Infarction: It is recommended that nadroparin is administered subcutaneously twice daily (every 12 hours). The usual duration of treatment is six days. In clinical studies in patients with unstable angina and non-Q wave myocardial infarction, nadroparin was administered in combination with up to 325 mg aspirin per day.
The initial dose is administered as a bolus injection intravenous (i.v.) and subsequent doses given by subcutaneous injection. The dose should be adjusted for body weight according to the table as follows, which is based on a target dose of 86 anti-Xa IU per kg body weight. (See Table 5.)
Click on icon to see table/diagram/image
Paediatric Population: Nadroparin is not recommended in children and adolescents as there are insufficient safety and efficacy data to establish dosage in patients aged less than 18 years.
Elderly: Prophylaxis of thromboembolic disorders in surgery, prevention of clotting in haemodialysis and treatment of Unstable Angina and Non-Q Wave Myocardial Infarction and VTE: No dosage adjustment is necessary in the elderly, unless renal function is impaired. It is recommended that renal function is assessed before initiating treatment (see Renal Impairment as follows and Pharmacology: Pharmacokinetics under Actions).
Prophylaxis of thromboembolic disorders in high risk medical patients (respiratory failure and/or respiratory infection and/or cardiac failure), immobilised due to acute illness or hospitalised in an intensive care unit: In elderly patients, dose reduction to 0.3 mL (2,850 Anti-Xa IU) may be appropriate.
Renal Impairment: Prophylaxis of thromboembolic disorders: Dose reduction is not required in patients with mild renal impairment (creatinine clearance greater than or equal to 50 ml/min).
Moderate and severe renal impairment is associated with increased exposure to nadroparin. These patients are at increased risk of thromboembolism and haemorrhage.
If a dose reduction is considered appropriate by the prescribing physician, taking into account the individual risk factors for haemorrhage and thromboembolism in patients with moderate renal impairment (creatinine clearance greater than or equal to 30 ml/min and less than 50 ml/min) the dose should be reduced by 25 to 33% (see Precautions and Pharmacology: Pharmacokinetics under Actions).
The dose should be reduced by 25 to 33% in patients with severe renal impairment (creatinine clearance less than 30 ml/min) (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Treatment of thromboembolic disorders, unstable angina and non-Q wave myocardial infarction: Dose reduction is not required in patients with mild renal impairment (creatinine clearance greater than or equal to 50 ml/min).
Moderate and severe renal impairment is associated with increased exposure to nadroparin. These patients are at increased risk of thromboembolism and haemorrhage.
If a dose reduction is considered appropriate by the prescribing physician, taking into account the individual risk factors for haemorrhage and thromboembolism in patients with moderate renal impairment (creatinine clearance greater than or equal to 30 ml/min and less than 50 ml/min) the dose should be reduced by 25 to 33% (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Nadroparin is contraindicated in patients with severe renal impairment (creatinine clearance less than 30 ml/min) (see Contraindications).
Hepatic Impairment: There have been no studies conducted in patients with hepatic impairment.
Method of Administration: Nadroparin is not intended for intramuscular injection.
The usual site for subcutaneous injection is on the right or left side of the abdominal wall, but the thigh may be used as an alternative. To avoid loss of the solution when using pre-filled syringes, the air bubble should not be expelled from the syringe before the injection. The needle should be inserted perpendicularly into a pinched-up fold of skin which should be held gently but firmly until injection has been completed. The injection site should not be rubbed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image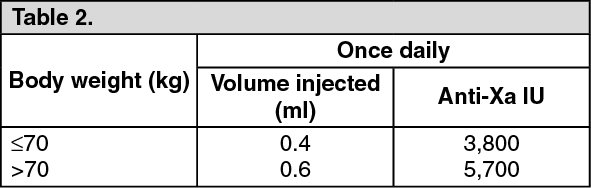 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image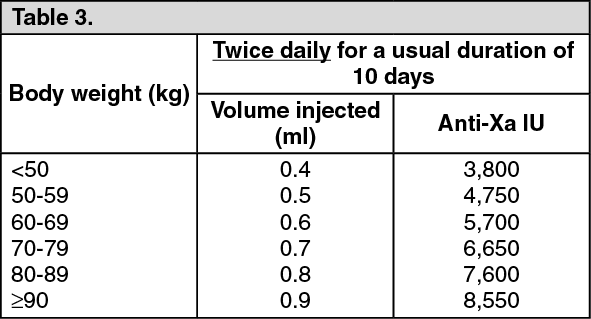 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image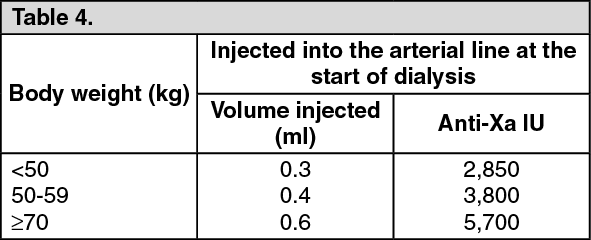 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image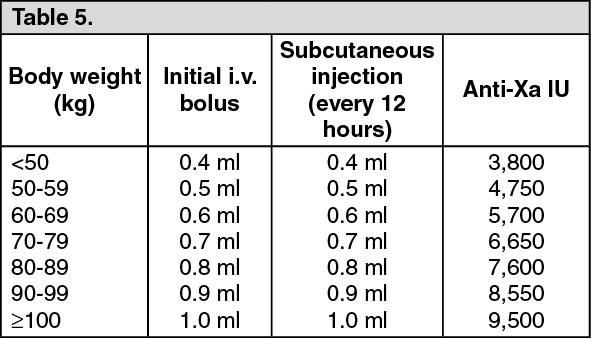 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 2_850 anti-Xa IU1d2c013a-6763-4689-9c01-abfb0080adc2.GIF)

 Sign Out
Sign Out
