Azithromycin dihydrate eq. to Azithromycin.
Pharmacotherapeutic group: Antibacterial (Macrolide).
Pharmacology: Azithromycin: Azithromycin is a macrolide antibiotic belonging to the azalide group. The molecule is constructed by adding a nitrogen atom to the lactone ring of Erythromycin A. The chemical name of Azithromycin is 9-deoxy-9a-aza-methyl-9a-homoerythromycin A. The molecular weight is 749.0 The mechanism of action of Azithromycin is based upon the suppression of bacterial protean synthesis by means of binding to the ribosomal 50s sub-unit and inhibition of peptide translocation.
Mechanism of resistance: Resistance of Azithromycin may be inherent or acquired. There are three main mechanisms of resistance in bacteria: target site alteration, alteration in antibiotic transport and modification of the antibiotic.
Complete cross resistance exists among
Streptococcus pneumonia, betahemolytic streptococcus of group A,
Enterococcus faecalis and
Staphylococcus aureus, including Methicilin resistance
S. aureus (MRSA) to Erythromycin, Azithromycin, other macrolides, and Lincosamides.
Breakpoints:
Azithromycin susceptibility breakpoints for typical bacterial pathogens are:
NCCLS:
Susceptible ≤ 2 mg/L; resistant to ≥ 8 mg/L
Haemophilus spp.: susceptible ≤ 4 mg/L
Streptococcus pneumonia and
Streptococcus pyogenes: susceptible ≤ 0.5 mg/L; resistant ≥ 2 mg/L.
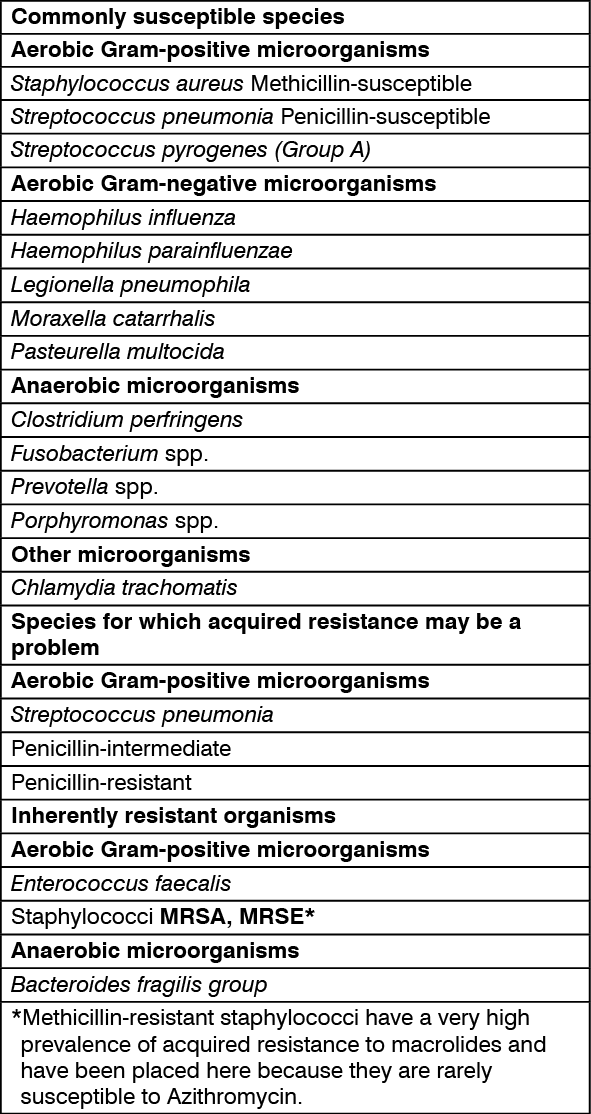
Susceptibility:
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable. (See table.)
 Click on icon to see table/diagram/image
Pharmacokinetics: Absorption:
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: approximately 37%.
Distribution: ranges from 12% to 0.5 microgram/mL up to 52% at 0.05 microgram Azithromycin/mL serum.
Elimination: 2-4 days.
Azithromycin is indicated for the treatment of bronchitis, community-acquired pneumonia, sinusitis, pharyngitis/tonsilitis, otitis media, skin and soft tissue infections, and uncomplicated genital infections due to Chlamydia trachomatis. Considerations should be given to official guidance regarding the appropriate use of antibacterial agents.
Oral.
Single daily dose: Azithromycin capsules (250 mg) should be taken at least 1 hour before or 2 hours after food.
Children over 45 Kg body weight and adults, including elderly patients: The total dose of Azithromycin is 1500 mg which should be given over three days (500 mg once daily). In uncomplicated genital infections due to Chlamydia trachomatis, the dose is 1000 mg as a single oral dose.
Over 45 Kg: Dose as per adults.
Renal failure: No dose adjustment is necessary in patients with mild to moderate (GFR 10-80 mL/min) or severe (GFR < 10 mL/min) renal impairment.
Hepatic failure: Since Azithromycin is metabolized in the liver and excreted in the bile, the drug should not be given to patients suffering from severe liver disease. No studies have been conducted regarding treatment of such patients with Azithromycin.
Adverse events experienced in higher than recommended doses were similar to those seen at normal doses. The typical symptoms of an overdose with macrolide antibiotics include reversible loss of hearing, severe nausea, vomiting and diarrhea. In the event of overdose, the administration of medicinal charcoal and general symptomatic treatment and supportive measures are indicated as required.
Azithromycin is contraindicated in patients with a known hypersensitivity to the active substance or any macrolides antibiotics. Because of the theoretical possibility of ergotism, Floctil and ergot derivatives should not also be co-administered.
Hypersensitivity: As with Erythromycin and other macrolides, rare serious allergic reactions, including angioedema and anaphylaxis (rarely fatal), dermatologic reactions including Stevens-Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN) (rarely fatal), and Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) have been reported. Some of these reactions with Azithromycin have resulted in recurrent symptoms and required a longer period of observation and treatment.
If an allergic reaction occurs, the drug should be discontinued and appropriate therapy should be instituted. Physicians should be aware that reappearance of the allergic symptoms may occur when symptomatic therapy is discontinued.
Prolongation of the QT interval: Prolonged cardiac repolarization and QT interval, imparting a risk of developing cardiac arrhythmia and torsades de pointes, have been seen in treatment with macrolides, including Azithromycin. Prescribers should consider the risk QT prolongation, which can be fatal when weighing the risks and benefits of Azithromycin for at-risk groups including: Patients with congenital or documented QT prolongation;
Patients currently receiving treatment with other active substances known to prolong QT interval, such as antiarrhythmics of Class IA and III, antipsychotic agents, antidepressants, and fluoroquinolones;
Patients with electrolyte disturbance, particularly in cases of hypokalemia and hypomagnesemia;
Patients with clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency;
Elderly patients: elderly patients may be more susceptible to drug-associated effects on the QT interval.
As with any antibiotic preparation, there is a possibility that superinfections could occur (e.g. fungal infection).
Streptococcal infection: Penicillin is usually the first choice for treatment of pharyngitis/ tonsillitis due to Streptococcus pyrogenes and also for prophylaxis of acute rheumatic fever.
Azithromycin is in general effective against streptococcus in oropharynx, but no data are available that demonstrate the efficacy of Azithromycin in preventing acute rheumatic fever. In patients with severe renal impairment (GFR <10 mL/min) a 33% increase in systemic exposure to Azithromycin was observed.
Infantile hypertrophic pyloric stenosis (IHPS) has been reported following the use of Azithromycin in infants (treatment up to 42 days of life). Parents and caregivers should be informed to contact their physician if vomiting and/or irritability with feeding occurs.
In the event of severe acute hypersensitivity reactions, such as anaphylaxis, severe cutaneous adverse reactions (SCARs) [e.g. Stevens-Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS) & acute generalized exanthematous pustulosis (AGEP), Floctil should be discontinued immediately and appropriate treatment should be urgently initiated.
Animal reproduction studies have demonstrated that Azithromycin crosses the placenta, but have revealed no evidence of harm to the fetus. There are no adequate and well controlled studies in pregnant women. Since animal studies are not always predictive to human response, Azithromycin should be used during pregnancy only if adequate are not available.
No data on secretion of Azihtromycin in breast milk are available, so that Azithromycin should only be used in lactating women where adequate alternatives are not available.
Rare: Blood and lymphatic system disorders (thrombocytopenia).
Psychiatric disorders (aggressiveness, agitation, anxiety and nervousness).
Nervous system disorders (insomnia and hyperactivity).
Ear and labyrinth disorders.
Cardiac disorders (palpitations and arrhythmias).
Vascular disorders (hypotension).
GI disorders (constipation, discoloration of the tongue, pancreatitis).
Hepato-biliary disorders (hepatitis, jaundice).
Skin and subcutaneous tissue disorders (angioneurotic edema, photosensitivity, urticaria).
Renal and urinary disorders (interstitial nephritis and acute renal failure).
General disorders (anaphylaxis).
Common: GI disorders (nausea, vomiting, diarrhea, abdominal discomfort).
Uncommon: Nervous system disorders (dizziness/ vertigo, somnolence, headache, convulsions taste perversion, syncope).
GI disorders (loose stools, flatulence, digestive disorders, anorexia, dyspepsia).
Skin and subcutaneous tissue disorders (allergic reactions including pruritus and rash).
Musculoskeletal and connective tissue disorders (arthralgia).
Reproductive system and breast disorder (vaginitis).
Post-marketing experience: Hepatobiliary disorders: Hepatitis and cholestatic jaundice have been reported, as well as rare cases of hepatic necrosis and hepatic failure, in which in rare instances have resulted in death.
Cardiac disorders: Palpitations and arrhythmias including ventricular tachycardia have been reported. There have been rare reports of QT prolongation and Torsades de Pointes.
Skin and subcutaneous tissue disorders: Allergic reactions including pruritus, rash, photosensitivity, edema, urticaria, and angioedema. Rarely, serious cutaneous adverse reactions including erythema multiformes, SJS, TEN and DRESS have been reported. Frequency not known: Severe cutaneous adverse reactions (SCARs) including Steven-Johnson Sydndrome (SJS), toxic epidermaly necrolysis (TEN), drug reaction with eosinophilia and systemic symptoms (DRESS) and acute generalized exanthematous pustulosis (AGEP).
Gastrointestinal disorders: Infantile hypertrophic pyloric stenosis.
Antacids: In patients receiving Azithromycin and antacids, Floctil should be taken at least 1 hour or 2 hours after the antacid.
Carbamazepine: In a pharmacokinetic interaction study in healthy volunteers, no significant effect was observed on the plasma levels of Carbamazepine or its active metabolite.
Cimetidine: A single dose of Cimetidine administered 2 hours before Floctil had no effect on the pharmacokinetics of Azithromycin.
Cyclosporin: In a pharmacokinetic study with healthy volunteers that were administered a 500 mg/day oral dose of Azithromycin for 3 days and were then administered a single 10 mg/kg oral dose of Cyclosproine Cmax and AUC0-5 were found to be significantly elevated (by 24% and 21% respectively), however no significant changes were seen in AUC0-∞. Consequently, caution should be exercised before considering co-administration of these two drugs. If co-administration is necessary, Cyclosporin levels should be monitored and the dose adjusted accordingly.
Digoxin: Some of the macrolide antibiotics have been reported to impair the metabolism of Digoxin (in the gut) in some patients. Therefore, in patients receiving concomitant Floctil and Digoxin the possibility of raised Digoxin levels should be borne in mind, and Digoxin levels monitored.
Ergot derivatives: Because of the theoretical possibility of ergotism, Floctil and ergot derivatives should not be co-administered.
Methylprednisolone: In a pharmacokinetic interaction study in healthy volunteers, Floctil had no significant effect on the pharmacokinetics of Methylprednisolone.
Terfenadine: Because of the occurrence of serious dysarrhythmias secondary to prolongation of the QTc interval in patients receiving other anti-infectives in conjunction with Terfenadine, pharmacokinetic interaction studies have been performed. These studies have reported no evidence of an interaction between Azithromycin and Terfenaine. There have been rare cases reported where the possibility of such an interaction could not be entirely excluded; however there was no specific evidence that such an interaction had occurred. As with other macrolides, Floctil should be administered with caution in combination with Terfenadine.
Theophylline: Theophylline levels may be increased in patients taking Floctil.
Coumarin-type oral anticoagulants: In a pharmacodynamic interaction study, Floctil did not alter the anticoagulant effect of a single 15 mg dose of Warfarin administered to healthy volunteers. There have been reports received in the post-marketing period of potentiated anticoagulation subsequent to co-administration of Azithromycin and Coumarin-type oral anticoagulants. Although a causal relationship has not been established, consideration should be given to the frequency of monitoring prothrombin time when Azithromycin is used in patients receiving Coumarin-type oral anticoagulants.
Zidovudine: Single 1000 mg doses and multiple 1200 mg or 600 mg doses of Azithromycin did not affect the plasma pharmacokinetics or urinary excretion of Zidovudine or its glucuronide metabolite. However, administration of Azithromycin increased the concentrations of phosphorylated Zidovudine, the clinically active metabolite, in peripheral blood mononuclear cells. The clinical significance of this finding is unclear, but it may be of benefit to patients.
Didanosine: Co-administration of daily doses of 1200 mg Azithromycin with Didanosine in 6 subjects did not appear to affect the pharmacokinetics of Didanosine as compared with placebo.
Rifabutin: Co-administration of Azithromycin and Rifabutin did not affect the serum concentration of either drug. Neutropenia was observed in subjects receiving concomitant treatment of Azithromycin and Rifabutin. Although neutropenia has been associated with the use of Rifabutin, a causal relationship to combination with Azithromycin has not been established.
Store at temperature of not more than 30°C.
J01FA10 - azithromycin ; Belongs to the class of macrolides. Used in the systemic treatment of infections.
Floctil cap 250 mg
10 × 6's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
