Pharmacotherapeutic group: antihaemorrhagics, fibrinogen.
ATC code: B02BB01.
Pharmacology: Pharmacodynamics: Human fibrinogen (coagulation factor I), in the presence of thrombin, activated coagulation factor XIII (FXIIIa) and calcium ions, is converted into a stable and elastic three-dimensional fibrin haemostatic clot.
The administration of human fibrinogen provides an increase in plasma fibrinogen level and can temporarily correct the coagulation defect of patients with fibrinogen deficiency.
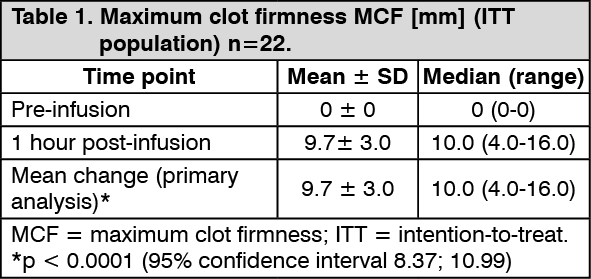
An open-label, prospective, randomized, controlled, two-arm cross-over single-dose pharmacokinetic phase 2 study in 22 patients with congenital fibrinogen deficiency (afibrinogenaemia) (see Pharmacology: Pharmacodynamics under Actions) also evaluated the maximum clot firmness (MCF) as a surrogate marker for haemostatic efficacy (FORMA-01). MCF was determined by thromboelastometry (ROTEM) testing. For each patient, MCF was determined before (baseline) and one hour after the single-dose administration of FIBRYGA. MCF values were significantly higher after administration of FIBRYGA than at baseline (see the table as follows). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
A prospective, open label, uncontrolled, multicentre phase 3 study (FORMA-02) was conducted in 25 patients with congenital fibrinogen deficiency (afibrinogenaemia and hypofibrinogenaemia), ranging in age from 12 to 54 years (6 adolescents, 19 adults). This included the treatment of 89 bleeding episodes and 12 surgical procedures. There was significant change from baseline in the MCF as measured by ROTEM and fibrinogen plasma levels. The median dose of FIBRYGA per infusion for the treatment of bleeding episodes was 57.5 mg/kg and the median total dose was 59.4 mg/kg. The median total dose of FIBRYGA per surgery was 85.8 mg/kg. Overall haemostatic efficacy was rated as successful (rating of good or excellent efficacy) for 98.9% of the treated bleeding episodes and for 100% of the surgeries by an independent adjudication committee using an objective scoring system.
Another prospective, open label, uncontrolled, multicentre phase 3 study (FORMA-04) was conducted in 14 children with congenital fibrinogen deficiency (afibrinogenaemia and hypofibrinogenaemia), ranging in age from 1 to 10 years (6 <6 years of age and 8 between 6 and <12 years of age). This included the treatment of 10 bleeding episodes and 3 surgical procedures, as well as single dose pharmacokinetics. There was a significant change from baseline in the MCF as measured by ROTEM and fibrinogen plasma levels. The median dose of FIBRYGA per infusion for treatment of bleeding episodes was 70.2 mg/kg and the median total dose was 73.9 mg/kg. The median total dose of FIBRYGA per surgery was 108 mg/kg. Overall haemostatic efficacy was rated as successful (rating of good or excellent efficacy) for 100 % of the treated bleeding episodes and of the surgeries by an independent adjudication committee using an objective scoring system.
The prospective, randomised, controlled study FORMA-05 investigated the haemostatic efficacy and safety of FIBRYGA by comparison with cryoprecipitate as fibrinogen supplementation sources in patients developing acquired fibrinogen deficiency during cytoreductive surgery for the extensive abdominal malignancy pseudomyxoma peritonei. The study included 43 adult patients in the Per Protocol (PP) analysis set, 21 patients treated with FIBRYGA and 22 patients treated with cryoprecipitate. Intraoperative fibrinogen supplementation was performed pre-emptively (i.e. after 60-90 minutes in surgery, when excessive blood loss was observed, but before 2 litres of blood had been lost) with doses of 4 g of FIBRYGA or of 2 pools of 5 units of cryoprecipitate, repeated as needed. During the 7.8 ± 1.7 hours of surgery, 6.5 ± 3 g of FIBRYGA (89 ± 39 mg/kg bw) and 4.1 ± 2.2 pools of 5 units of cryoprecipitate were used, respectively. A median of 1 unit and 0.5 units RBC were administered intraoperatively to the patients treated with FIBRYGA and cryoprecipitate, respectively, with a median of 0 units RBC during the first 24 hours post-operatively in both groups (see the table as follows). No fresh frozen plasma or platelet concentrates were transfused during the study Haemostatic therapy based on fibrinogen supplementation was rated as successful for 100% of the surgeries in both groups by an independent adjudication committee using an objective scoring system. (See Table 2.)
Click on icon to see table/diagram/image
Paediatric population: In congenital fibrinogen deficiency, FIBRYGA was administered in two clinical studies (FORMA-02 and FORMA-04) in 20 patients from 1 to <18 years of age, of which 6 adolescents 12 to <18 years of age, 8 children 6 to <12 years of age and 6 children 1 to <6 years of age. Haemostatic efficacy was assessed as successful by an independent adjudication committee for all bleeding episodes treated (10 bleeding episodes in adolescents, 5 in children 6 to <12 years of age and 5 in children 1 to <6 years of age) and prophylaxis was also assessed as successful for the 4 surgeries performed in these patients (1 in adolescents and 3 in children 1 to <6 years of age).
Pharmacokinetics: Human fibrinogen is a normal constituent of human plasma and acts like endogenous fibrinogen. In plasma, the biological half-life of fibrinogen is 3-4 days. FIBRYGA is administered intravenously and is immediately available in a plasma concentration corresponding to the dosage administered.
An open-label, prospective, randomised, controlled, two-arm cross-over phase 2 study in 22 patients with congenital fibrinogen deficiency (afibrinogenaemia), ranging in age from 12 to 53 years (6 adolescents, 16 adults), compared the single-dose pharmacokinetic properties of FIBRYGA with those of another commercially available fibrinogen concentrate in the same patients (FORMA-01).
Each patient received a single intravenous 70 mg/kg dose of FIBRYGA and the comparator product. Blood samples were drawn to determine the fibrinogen activity at baseline and up to 14 days after the infusion. The pharmacokinetic parameters of FIBRYGA in the per protocol (PP) analysis (n=21) are summarised in the table as follows. (See Table 3.)
Click on icon to see table/diagram/image
The incremental in vivo recovery (IVR) was determined from levels obtained up to 4 hours post-infusion. The median incremental IVR was 1.8 mg/dL (range, 1.08-2.62 mg/dL) increase per mg/kg. The median IVR indicates that a dose of 70 mg/kg will increase the patient's fibrinogen plasma concentration by approximately 125 mg/dL.
Pharmacokinetics in specific populations: No statistically relevant difference in fibrinogen activity was observed between male and female study participants.
Paediatric population: Pharmacokinetic data in adolescents from 12 to less than 18 years of age was obtained in the FORMA-02 study. In the PP analysis, a small difference between the half-life for adolescents (n=5) and for adults (n=16) was observed, with 72.8 ± 16.5 hours as compared to 76.9 ± 26.1 hours, respectively. Clearance was almost identical in the two age groups, i.e., 0.68 ± 0.18 mL/hr/kg and 0.66 ± 0.21 mL/hr/kg, respectively.
The pharmacokinetic properties of FIBRYGA were further investigated in the FORMA-04 study in 13 children less than 12 years of age with congenital fibrinogen deficiency (afibrinogenaemia). Each patient received a single intravenous 70 mg/kg dose of FIBRYGA. The pharmacokinetic parameters of FIBRYGA are summarised in the table as follows. The median incremental IVR was 1.4 mg/dL (range, 1.3-2.1 mg/dL) increase per mg/kg. (See Table 4.)
Click on icon to see table/diagram/image
Lower incremental in vivo recovery (IVR), faster clearance and shorter half-life were observed in children aged 1 to less than 12 years of age, compared to adults and adolescents. As higher doses of FIBRYGA were administered for the treatment of bleeding episodes in children aged 1 to less than 12 years of age, higher doses may be required in this age group.
Toxicology: Preclinical safety data: The safety of FIBRYGA has been demonstrated in several non-clinical safety pharmacology (cardiovascular effects, thrombogenic potential) and toxicology studies (acute toxicity, local tolerance). The non-clinical data reveal no special hazard for humans based on these studies. In the venous stasis test (Wessler test) FIBRYGA proved to be non-thrombogenic at doses up to 400 mg/kg body weight.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image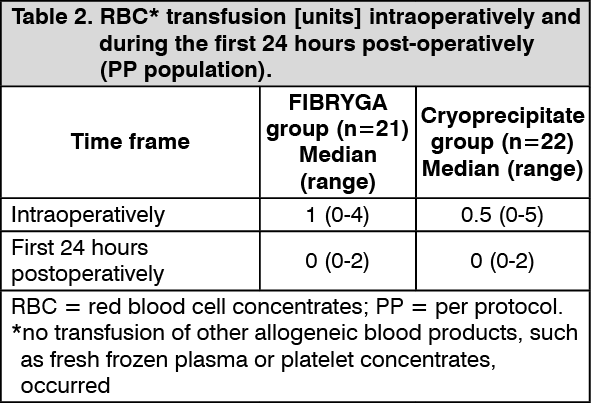 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image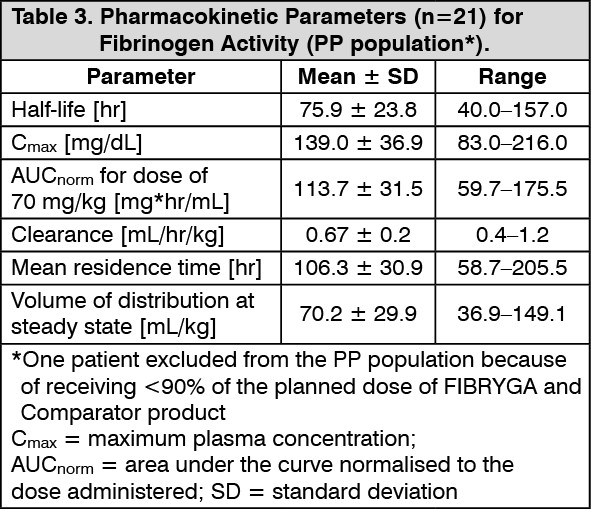 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image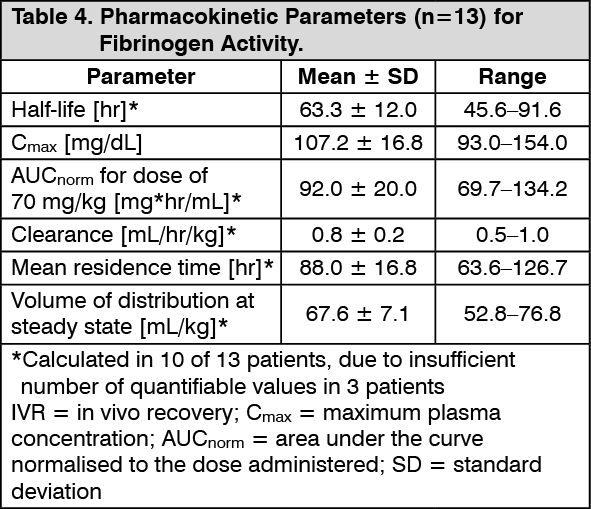 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
