


 Sign Out
Sign Out

Mechanism of Action: Fabry disease is an X-linked genetic disorder of glycosphingolipid metabolism. Deficiency of the lysosomal enzyme α-galactosidase A leads to progressive accumulation of glycosphingolipids, predominantly GL-3, in many body tissues, starting early in life and continuing over decades. Clinical manifestations of Fabry disease include renal failure, cardiomyopathy, and cerebrovascular accidents. Accumulation of GL-3 in renal endothelial cells may play a role in renal failure.
Fabrazyme is intended to provide an exogenous source of α-galactosidase A in Fabry disease patients. Non-clinical and clinical studies evaluating a limited number of cell types indicate that Fabrazyme will catalyze the hydrolysis of glycosphingolipids including GL-3.
Clinical Studies: The safety and efficacy of Fabrazyme were assessed in four clinical studies in patients with Fabry disease.
Study 1 was a randomized, double-blind, placebo-controlled, multi-national, multi-centre study of 58 Fabry patients (56 males and 2 females), ages 16 to 61 years, all naive to enzyme replacement therapy. Patients received either 1.0 mg/kg of Fabrazyme or placebo every two weeks for five months (20 weeks) for a total of 11 infusions. All patients were pretreated with acetaminophen and an antihistamine to decrease or prevent infusion reactions. Oral steroids were an additional option to the pretreatment regimen for patients who exhibited severe or recurrent infusion reactions. The primary efficacy endpoint of GL-3 inclusions in renal interstitial capillary endothelial cells, was assessed by light microscopy and was graded on an inclusion severity score ranging from 0 (normal or near normal) to 3 (severe inclusions).
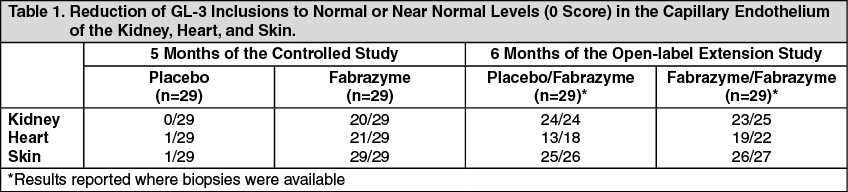
A GL-3 inclusion score of 0 was achieved in 20 of 29 (69%) patients treated with Fabrazyme compared to 0 of 29 treated with placebo (p<0.001). Similar reductions in GL-3 inclusions were observed in the capillary endothelium of the heart and skin (see Table 1). No differences between groups in symptoms or renal function were observed during this five month study. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAll 58 patients in the Study 1 participated in an open-label extension study of Fabrazyme at 1.0 mg/kg every two weeks, which continued for an additional 54 months. At the end of six months of open-label treatment, most patients achieved a GL-3 inclusion score of 0 in capillary endothelium (see Table 2). GL-3 was decreased to normal or near normal levels in mesangial cells, glomerular capillary endothelium, interstitial cells, and non-capillary endothelium. GL-3 deposition was still present in vascular smooth muscle cells, tubular epithelium and podocytes at variably reduced levels. Forty-four of the 58 patients completed 54 months of the open-label extension study. Thirty-six of these 44 patients underwent follow-up skin biopsy, and 31 of these patients showed sustained GL-3 clearance in the capillary endothelium of the skin. Follow-up heart and kidney biopsies were assessed in only 8 of the 44 patients, which showed sustained GL-3 clearance in the capillary endothelium of the kidney in 8 patients, and sustained GL-3 clearance in the capillary endothelium of the heart in 6 patients. Plasma GL-3 levels were reduced to normal levels (≤7.03 μg/mL determined by LC/MS/MS) and remained at normal levels after up to 60 months of treatment. The reduction of GL-3 inclusions suggests that Fabrazyme may ameliorate disease expression; however, the relationship of GL-3 inclusion reduction to specific clinical manifestations of Fabry disease has not been established.
Study 2 was randomized (2:1 Fabrazyme to placebo), double blind, placebo-controlled, multi-national, multi-center study of 82 patients (72 males and 10 females), ages 20 to 72 years, all naive to enzyme replacement therapy. Patients received either 1.0 mg/kg of Fabrazyme or placebo every two weeks for up to a maximum of 35 months (median 18.5 months). There was significant difference in post-baseline plasma GL-3 levels in the Fabrazyme-treated patients compared to the placebo. The reduction in plasma GL-3 levels in the Fabrazyme group was significant at one year (p<0.0001) and at two years (p=0.0019). Fourteen patients (8 in Fabrazyme-treated and 6 in placebo) had skin biopsies at first infusion and final visit. All Fabrazyme-treated patients had capillary endothelium and deep vessel endothelium scores of zero at the final visit. Four (4) of 6 placebo patients had non-zero capillary endothelium scores (p=0.0150), and 6 of 6 had non-zero deep vessel endothelium scores (p=0.0003).
Sixty-seven patients who participated in Study 2 were subsequently entered into an open-label extension study in which all patients received 1.0 mg/kg of Fabrazyme every two weeks for up to a maximum of 18 months. There was a statistically significant reduction in mean plasma GL-3 levels with durability in effect through the additional 18 months of treatment in the extension study from pretreatment baseline.
Study 3 (Pediatric Study) was an open-label, uncontrolled, multi-national, multi-center study to evaluate safety, pharmacokinetics, and pharmacodynamics of Fabrazyme treatment in 16 pediatric patients with Fabry disease (14 males, 2 females), who were ages 8 to 16 years at first treatment. All patients received Fabrazyme 1.0 mg/kg every two weeks for up to 48 weeks. At baseline, all 14 males had elevated plasma GL-3 levels (i.e., >7.03 μg/mL), whereas the two female patients had normal plasma GL-3 levels.
Twelve of the 14 male patients, and no female patients, had GL-3 inclusions observed in the capillary endothelium on skin biopsies at baseline. At Weeks 24 and 48 of treatment, all 14 males had plasma GL-3 within the normal range. The 12 male patients with GL-3 inclusions in capillary endothelium at baseline achieved GL-3 inclusion scores of 0 at Weeks 24 and 48 of treatment. The two female patients' plasma GL-3 levels remained normal through study Week 48.
No new safety concerns were identified in pediatric patients in this study, and the overall safety and efficacy profile of Fabrazyme treatment in pediatric patients was found to be consistent with that seen in adults. Immunologic responses in pediatric patients may differ from those in adults, as IgG seroconversion in pediatric patients was associated with prolonged half-life concentrations of Fabrazyme, a phenomenon rarely observed in adult patients (see Pharmacology under Actions, Adverse Reactions, and Pediatric Use under Precautions).
Study 4 was an open-label, re-challenge study to evaluate the safety of Fabrazyme treatment in patients who had a positive skin test to Fabrazyme or who had tested positive for Fabrazyme-specific IgE antibodies. In this study, six adult male patients, who had experienced multiple or recurrent infusion reactions during previous clinical trials with Fabrazyme, were re-challenged with Fabrazyme administered as a graded infusion, for up to 52 weeks of treatment (see Immunogenicity and Rechallenge under Precautions). The initial two re-challenge doses of Fabrazyme were administered as a 0.5 mg/kg dose per week at an initial infusion rate of 0.01 mg/min for the first 30 minutes (1/25th the usually recommended maximum infusion rate). The infusion rate was doubled every 30 minutes thereafter, as tolerated, for the remainder of the infusion up to a maximum rate of 0.25 mg/min. If the patient tolerated the infusion, the dose was increased to 1.0 mg/kg every two weeks (usually recommended dose), and the infusion rate was increased by slow titration upwards (see Dosage & Administration).
Four of the six patients treated in this study received at least 26 weeks of study medication, and two patients discontinued prematurely due to recurrent infusion reactions (see Immunogenicity and Rechallenge under Precautions).
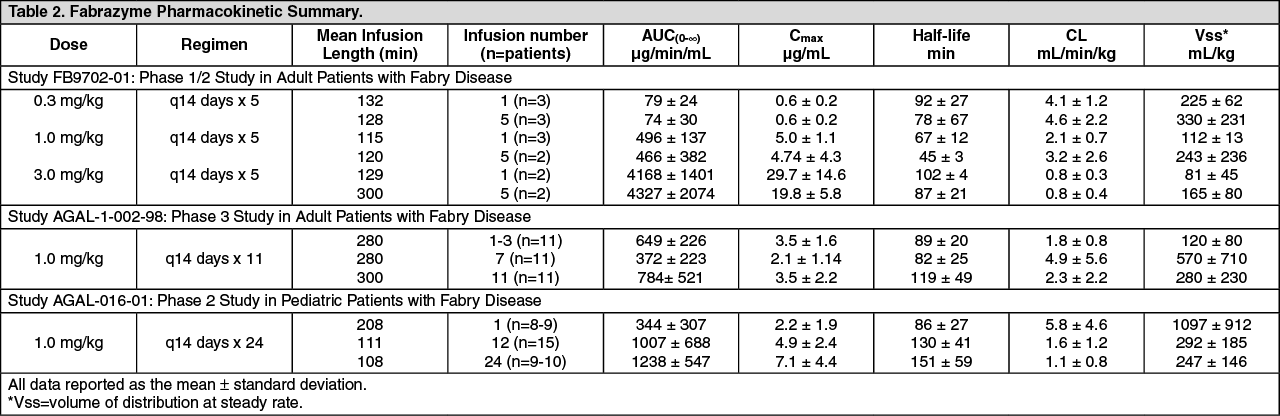
Pharmacokinetics: Plasma pharmacokinetic profiles of Fabrazyme were characterized at 0.3, 1.0, and 3.0 mg/kg in adult patients with Fabry disease. The area under the plasma concentration-time curve (AUC∞) and the clearance (CL) did not increase proportionately with increasing doses, demonstrating that the enzyme follows non-linear pharmacokinetics (Table 2). Plasma pharmacokinetic profiles were also characterized in adult patients with Fabry disease given 1.0 mg/kg Fabrazyme every 14 days for a total of 11 infusions. Refer to Table 2 as follows for more details.
In 15 pediatric Fabry patients (ranging in age from 8 to 16 years old and weighing between 27.1 to 64.9 kg) who were dosed with 1.0 mg/kg every 14 days, Fabrazyme pharmacokinetics were not weight-dependent (Table 2). Fabrazyme concentrations were about 5-times higher after IgG seroconversion, without any detectable impact on GL-3 clearance.
IgG seroconversion in pediatric patients was associated with prolonged half-life and plasma concentrations of Fabrazyme, a phenomenon rarely observed in adult patients. A possible cause for this prolongation likely pertains to the ability of antibodies to potentially act as "carriers" for their antigens (see Pediatric Use under Precautions and Immunogenicity under Adverse Reactions). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image