HBsAg, recombinant DNA produced in yeast cells.
10 μg dose vaccine: 1 dose (0.5 ml) contains: Hepatitis B surface antigen 1, 2: 10 micrograms.
1 Adsorbed on aluminium hydroxide, hydrated. Total: 0.25 milligrams Al3+.
2 Produced in yeast cells (Saccharomyces cerevisiae) by recombinant DNA technology.
20 μg dose vaccine: 1 dose (1 ml) contains: Hepatitis B surface antigen1, 2: 20 micrograms.
1 Adsorbed on aluminium hydroxide, hydrated. Total: 0.50 milligrams Al3+.
2 Produced in yeast cells (Saccharomyces cerevisiae) by recombinant DNA technology.
The vaccine is highly purified, and exceeds the WHO requirements for recombinant hepatitis B vaccines. No substances of human origin are used in its manufacture.
Upon storage, a fine white deposit with a clear colourless supernatant may be observed.
Excipients/Inactive Ingredients: Sodium chloride, sodium phosphate dihydrate, sodium dihydrogen phosphate, water for injections.
Polysorbate 20 is present as residual from the manufacturing process.
Pharmaco-therapeutic group: Hepatitis B vaccine.
ATC code: J07BC01.
Pharmacology: Pharmacodynamics: Engerix-B induces specific humoral antibodies against HBsAg (anti-HBs antibodies). Anti-HBs antibody concentrations ≥ 10 mIU/ml correlates with protection to HBV infection.
Protective efficacy and long-term immune response: At risk groups: In field studies, a protective efficacy between 95% and 100% was demonstrated in neonates, children and adults at risk.
A 95% protective efficacy was demonstrated in neonates of HBeAg positive mothers, immunised according to the 0, 1, 2 and 12 or 0, 1 and 6 schedules without the concomitant administration of HBIg at birth. However, simultaneous administration of HBIg and vaccine at birth increased the protective efficacy to 98%.
Twenty years after primary vaccination during infancy, subjects born to mothers who were HBV carriers, received a challenge dose of Engerix-B. One month later, at least 93% of subjects (N=75) mounted an anamnestic response demonstrating immune memory.
Healthy subjects: The table as follows summarizes seroprotection rates (i.e. percentages of subjects with anti-HBs antibody concentrations ≥ 10 mIU/ml) obtained in clinical studies with the different schedules mentioned in Dosage & Administration: (See Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The long-term immune response was assessed in a clinical trial in subjects from 11 years up to and including 15 years of age at the time of primary vaccination. The seroprotection rates obtained with the two different dosages and schedules were evaluated up to 66 months after the first dose of the primary vaccination and are presented in the table as follows: (See Table 2).
Click on icon to see table/diagram/image
These data show that a primary vaccination with Engerix-B vaccine induces circulating anti-HBs antibodies that persist for at least 66 months. After having completed the primary course, at each time point there is no clinically significant difference in the seroprotection rates when comparing the 2 vaccine groups.
All subjects in both vaccine groups (including subjects with anti-HBs antibody concentrations < 10 mIU/ml) received a challenge dose 72 to 78 months after primary vaccination. One month after the challenge dose, all subjects mounted an anamnestic response to the challenge dose and were shown to be seroprotected (i.e. anti-HBs antibody concentrations ≥ 10 mIU/ml). These data suggest that protection against hepatitis B may still be conferred through immune memory in all subjects who responded to primary vaccination but lost seroprotection level of anti-HBs antibodies.
Long-term persistence was assessed in a clinical study in subjects (N=292) aged 15 to 16 years, vaccinated in the first 2 years of life with 3 doses of Engerix B. The anti-HBs seroprotection was 65.4% at 14 years [range 13.5-15.5 years] after primary vaccination. At this time point, all subjects (including subjects with anti-HBs antibody concentrations < 10 mIU/ml) received a challenge dose. One month after the challenge dose, 97.9% of subjects were shown to be seroprotected. An anamnestic response was observed in 92.9% of subjects seronegative before the challenge dose (N=84) and in 98.6% of subjects seropositive before the challenge dose (N=207).
Patients with renal insufficiency including patients undergoing haemodialysis: (See Table 3).
Click on icon to see table/diagram/image
Patients with type II diabetes: (See Table 4).
Click on icon to see table/diagram/image
Reduction in the incidence of hepatocellular carcinoma in children: A significant reduction in the incidence of hepatocellular carcinoma has been observed in children aged 6-14 years following a nationwide hepatitis B vaccination in Taiwan. There was a significant decline in the prevalence of hepatitis B antigen, the persistence of which is an essential factor in the development of hepatocellular carcinoma.
Toxicology: Non-Clinical Information: Appropriate safety tests have been performed.
Engerix-B is indicated for active immunisation against HBV infection caused by all known subtypes in subjects of all ages considered at risk of exposure to HBV. It can be expected that hepatitis D will also be prevented by immunisation with Engerix-B as hepatitis D (caused by the delta agent) does not occur in the absence of hepatitis B infection.
Immunisation against hepatitis B is expected in the long term to reduce not only the incidence of this disease, but also its chronic complications such as chronic active hepatitis B and hepatitis B associated cirrhosis.
In areas of low prevalence of hepatitis B, immunisation is particularly recommended for those belonging to groups identified at increased risk of infection (see as follows), however, universal immunisation of all infants and adolescents will contribute to the control of hepatitis B on a population basis.
In areas of intermediate and high prevalence of hepatitis B, with most of the population at risk of acquiring the HBV, the best strategy is to provide universal immunisation of neonates, infants, children and adolescents, as well as adults belonging to groups at increased risk of infection.
The WHO, the US Immunisation Practices Advisory Committee (ACIP) and the American Academy of Paediatrics advocate that the vaccination of new-borns and/or the vaccination of adolescents is the optimal strategy for the control of hepatitis B in all countries.
Groups identified at increased risk of infection: Health Care Personnel.
Patients frequently receiving blood products.
Personnel and residents of institutions.
Persons at increased risk due to their sexual behaviour.
Illicit users of addictive injectable drugs.
Travellers to areas with a high endemicity of HBV.
Infants born of mothers who are HBV carriers.
Persons originating from areas with a high endemicity of HBV.
Patients with sickle-cell anaemia.
Patients who are candidates for organ transplantation.
Household contacts of any of the previously mentioned groups and of patients with acute or chronic HBV infection.
Subjects with chronic liver disease (CLD) or at risk of developing CLD (e.g. Hepatitis C virus carriers, persons who abuse alcohol).
Others: Police personnel, fire brigade personnel, armed forces personnel and anybody who through their work or personal lifestyle may be exposed to HBV.
20 μg dose vaccine: The 20 μg dose (in 1 ml suspension) is intended for use in subjects 20 years of age and older.
10 μg dose vaccine: The 10 μg dose (in 0.5 ml suspension) is intended for use in neonates, infants and children up to and including the age of 19 years.
However, the 20 μg vaccine can also be used in subjects from 11 years up to and including 15 years of age as a 2-dose schedule in situations when there is a low risk of hepatitis B infection during the vaccination course and when compliance with the complete vaccination course can be assured (see Pharmacology: Pharmacodynamics under Actions).
Primary immunisation schedules: All subjects: A 0, 1 and 6 months schedule gives optimal protection at month 7 and produces high antibody titres. An accelerated schedule, with immunisation at 0, 1 and 2 months, will confer protection more quickly and is expected to provide better patient compliance. With this schedule, a fourth dose should be administered at 12 months to assure long term protection as titres after the third dose are lower than those obtained after the 0, 1, 6 months schedule. In infants, this schedule will allow for simultaneous administration of hepatitis B with other childhood vaccines.
Subjects 20 years of age and above: In exceptional circumstances in adults, where an even more rapid induction of protection is required, e.g. persons travelling to areas of high endemicity and who commence a course of vaccination against hepatitis B within one month prior to departure, a schedule of three intramuscular injections given at 0, 7 and 21 days may be used. When this schedule is applied, a fourth dose is recommended 12 months after the first dose (see Pharmacology: Pharmacodynamics under Actions for seroconversion rates).
Subjects from 11 years up to and including 15 years of age: The 20 μg vaccine may be administered in subjects from 11 years up to and including 15 years of age according to a 0, 6 months schedule. However, in this case, protection against hepatitis B infections may not be obtained until after the second dose (see Pharmacology: Pharmacodynamics under Actions). Therefore, this schedule should be used only when there is a low risk of hepatitis B infection during the vaccination course and when completion of the two-dose vaccination course can be assured. If both conditions cannot be assured (for instance patients undergoing haemodialysis, travellers to endemic regions and close contacts of infected subjects), the three-dose or the accelerated schedule of the 10 μg vaccine should be used.
Patients with renal insufficiency including patients undergoing haemodialysis 16 years of age and above: The primary immunisation schedule for patients with renal insufficiency including patients undergoing haemodialysis is four double doses (2 x 20 μg) at elected date, 1 month, 2 months and 6 months from the date of the first dose. The immunisation schedule should be adapted in order to ensure that the anti-HBs antibody titre remains equal to or higher than the accepted protective level of 10 mIU/ml.
Patients with renal insufficiency including patients undergoing haemodialysis up to and including 15 years of age, including neonates: Patients with renal insufficiency, including patients undergoing haemodialysis, have a reduced immune response to hepatitis B vaccines. Either the 0, 1, 2 and 12 months or the 0, 1, 6 months schedule of Engerix-B 10 μg can be used. Based on adult experience, vaccination with a higher dosage of antigen may improve the immune response. Consideration should be given to serological testing following vaccination. Additional doses of vaccine may be needed to ensure a protective anti-HBs level ≥ 10 mIU/ml.
Known or presumed exposure to HBV: In circumstances where exposure to HBV has recently occurred (e.g. needlestick with contaminated needle), the first dose of Engerix-B can be administered simultaneously with HBIg which however must be given at a separate injection site (see Interactions). The 0, 1, 2-12 months immunisation schedule should be advised.
Neonates born of mothers who are HBV carriers: The immunisation with Engerix-B (10 μg) of these neonates should start at birth, and one of the two immunisation schedules have to be followed. Either the 0, 1, 2 and 12 months or the 0, 1 and 6 months schedule can be used; however, the former schedule provides a more rapid immune response. When available, HBIg should be given simultaneously with Engerix-B at a separate injection site as this may increase the protective efficacy.
These immunisation schedules may be adjusted to accommodate local immunisation practices with regard to the recommended age of administration of other childhood vaccines.
Booster dose: The need for a booster dose in healthy individuals who have received a full primary vaccination course has not been established; however, some official vaccination programmes currently include a recommendation for a booster and these should be respected.
For haemodialysis and other immunocompromised patients, booster doses are recommended in order to ensure an antibody level of ≥ 10 mIU/ml.
Booster data are available. The booster dose is as well tolerated as the primary vaccination course.
Method of Administration: Engerix-B should be injected intramuscularly in the deltoid region in adults and children or in the anterolateral thigh in neonates, infants and young children. Exceptionally, the vaccine may be administered subcutaneously in patients with thrombocytopenia or bleeding disorders.
Engerix-B should not be administered in the buttock or intradermally since this may result in a lower immune response.
Cases of overdose have been reported during post-marketing surveillance. Adverse events reported following overdosage were similar to those reported with normal vaccine administration.
Engerix-B should not be administered to subjects with known hypersensitivity to any component of the vaccine, or to subjects having shown signs of hypersensitivity after previous Engerix-B administration.
HIV infection is not considered as a contraindication for hepatitis B vaccination.
As with other vaccines, the administration of Engerix-B should be postponed in subjects suffering from acute severe febrile illness. The presence of a minor infection, however, is not a contra-indication for immunisation.
Because of the long incubation period of hepatitis B it is possible for unrecognised infection to be present at the time of immunisation. The vaccine may not prevent hepatitis B infection in such cases.
The vaccine will not prevent infection caused by other pathogens known to infect the liver such as hepatitis A, hepatitis C and hepatitis E virus.
The immune response to hepatitis B vaccines is related to a number of factors, including older age, male gender, obesity, smoking habits and route of administration. In subjects who may respond less well to the administration of the hepatitis B vaccines (e.g. more than 40 years of age etc.), additional doses may be considered.
In patients with renal insufficiency including patients undergoing haemodialysis, HIV infected patients and persons with an impaired immune system, adequate anti-HBs antibody titres may not be obtained after the primary immunisation course and such patients may therefore require administration of additional doses of vaccine. (see Patients with renal insufficiency including patients undergoing haemodialysis under Dosage & Administration).
As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of rare anaphylactic reactions following the administration of the vaccine.
Syncope (fainting) can occur following, or even before, any vaccination as a psychogenic response to the needle injection. It is important that procedures are in place to avoid injury from faints.
Engerix-B should not be administered in the buttock or intradermally since this may result in a lower immune response.
Engerix-B should under no circumstances be administered intravascularly.
As with any vaccine, a protective immune response may not be elicited in all vaccinees (see Pharmacology: Pharmacodynamics under Actions).
The potential risk of apnoea and the need for respiratory monitoring for 48-72h should be considered when administering the primary immunisation series to very premature infants (born ≤ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. As the benefit of vaccination is high in this group of infants, vaccination should not be withheld or delayed.
Effects on Ability to Drive and Use Machines: The vaccine is unlikely to produce an effect on the ability to drive and use machines.
Pregnancy: Adequate human data on use during pregnancy and adequate animal reproduction studies are not available.
However, as with all inactivated viral vaccines one does not expect harm for the foetus.
Engerix-B should be used during pregnancy only when clearly needed, and the possible advantages outweigh the possible risks for the foetus.
Lactation: Adequate human data on use during lactation and adequate animal reproduction studies are not available.
No contraindication has been established.
The safety profile presented as follows is based on data from more than 5300 subjects.
Frequencies are reported as: Very common: (≥1/10); Common: (≥1/100 to <1/10); Uncommon: (≥1/1,000 to <1/100); Rare: (≥1/10,000 to <1/1,000); Very rare: (<1/10,000). (See Table 5.)
Click on icon to see table/diagram/image
In a comparative trial in subjects from 11 years up to and including 15 years of age, the incidence of local and general solicited symptoms reported after a two-dose regimen of Engerix-B 20 μg was similar overall to that reported after the standard three-dose regimen of Engerix-B 10 μg.
The simultaneous administration of Engerix-B and a standard dose of HBIg does not result in lower anti-HBs antibody titres provided that they are administered at separate injection sites.
Engerix-B can be given concomitantly with DTP, DT and/or polio vaccines, if this fits conveniently in an immunisation scheme recommended by the country Health Authority.
Engerix-B can also be administered together with measles-mumps-rubella vaccines, Haemophilus influenzae b vaccine, hepatitis A vaccine and BCG.
Engerix-B can be given concomitantly with Human Papillomavirus (HPV) vaccine (Cervarix).
Administration of Engerix-B at the same time as Cervarix has shown no clinically relevant interference in the antibody response to the HPV antigens. Anti-HBs geometric mean antibody concentrations were lower on co-administration, but the clinical significance of this observation is not known since the seroprotection rates remain unaffected. The proportion of subjects reaching anti-HBs ≥ 10 mIU/ml was 97.9% for concomitant vaccination and 100% for Engerix-B alone.
Different injectable vaccines should always be administered at different injection sites.
Interchangeability of hepatitis B vaccines: Engerix-B may be used to complete a primary immunisation course started either with plasma-derived or with other genetically-engineered hepatitis B vaccines, or as a booster dose in subjects who have previously received a primary immunisation course with plasma-derived or with other genetically-engineered hepatitis B vaccines.
Incompatibilities: Engerix-B should not be mixed with other vaccines.
Use and Handling: Upon storage, a fine white deposit with a clear colourless supernatant may be observed. The vaccine should be well shaken before use to obtain a slightly opaque, white suspension.
The vaccine should be inspected visually for any foreign particulate matter and/or abnormal physical appearance prior to administration. In the event of either being observed, do not administer the vaccine.
Any unused product or waste material should be disposed of in accordance with local requirements.
Store in a refrigerator (2°C - 8°C).
Do not freeze.
Store in the original package in order to protect from light.
Stability data indicate that Engerix-B is stable at temperatures up to 37°C for 3 days or up to 25°C for 7 days. These data are intended to guide healthcare professionals in case of temporary temperature excursion only. The storage conditions are detailed on the packaging.
J07BC01 - hepatitis B, purified antigen ; Belongs to the class of hepatitis viral vaccines.
Engerix-B vaccine 10 mcg/0.5 mL
1's
Engerix-B vaccine 20 mcg/mL
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image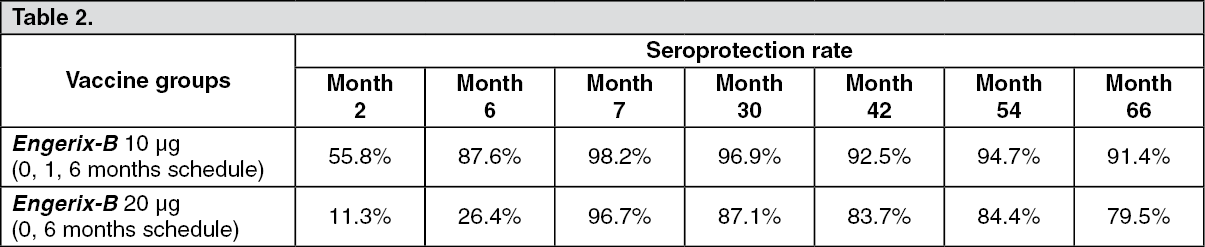 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image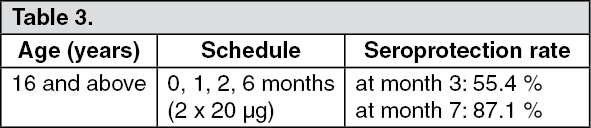 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image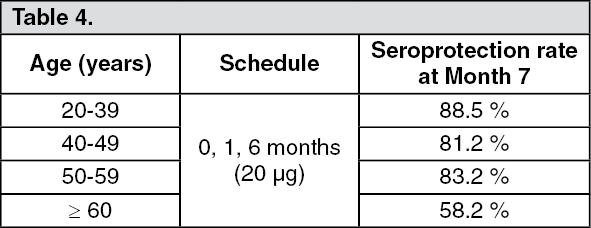 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image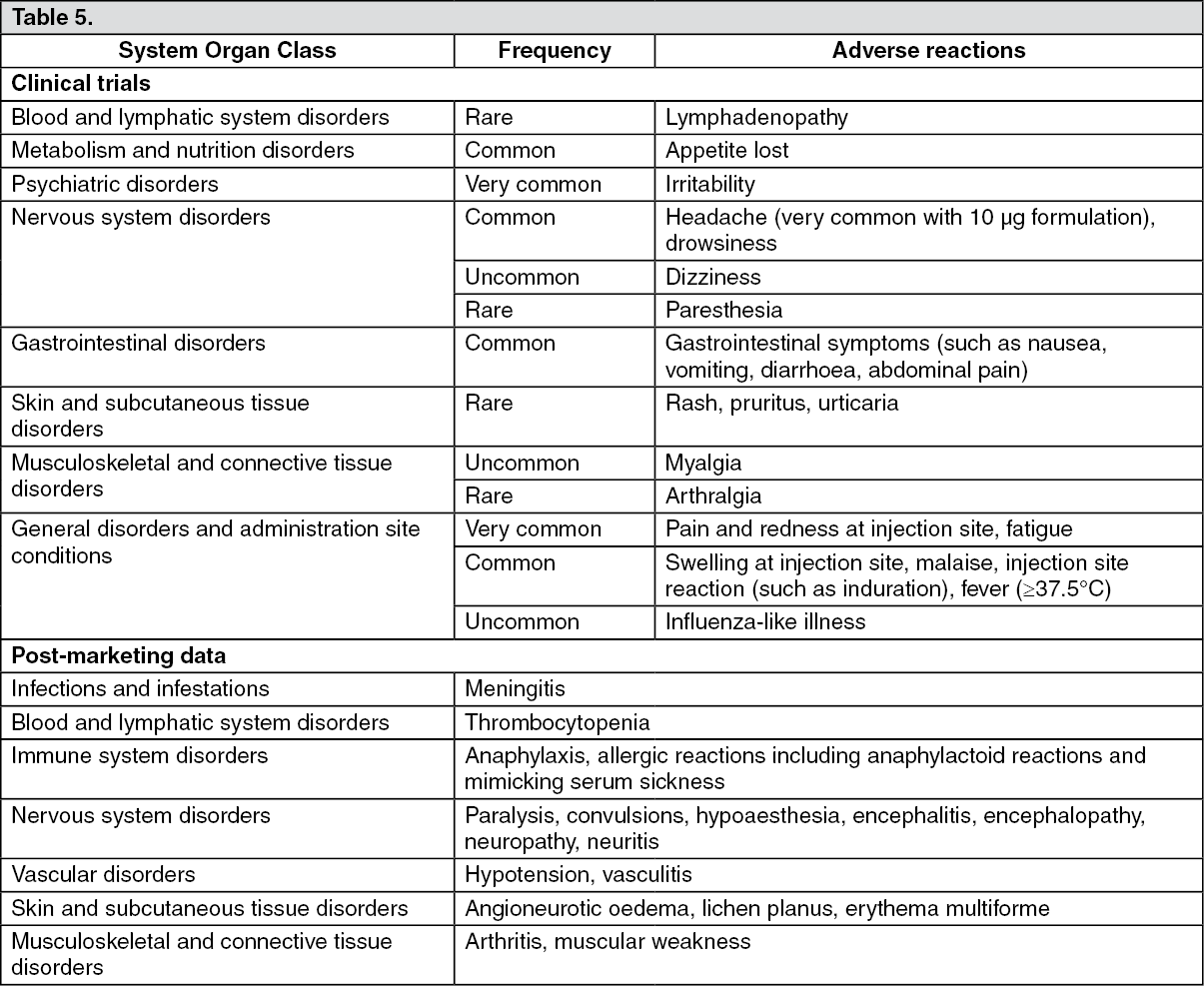 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
