One gram of cream contains lidocaine 25 mg and prilocaine 25 mg.
EMLA cream is an oil/water emulsion in which the oil phase consists of a eutectic mixture of lidocaine and prilocaine in the ratio 1:1.
Excipients/Inactive Ingredients: Carbomer, macrogol glycerol hydroxystearate, sodium hydroxide to pH 8.7-9.7, water.
Pharmacotherapeutic Group: Local anaesthetics of the amide-type. ATC Code: N01B B20.
Pharmacology: Pharmacodynamics: EMLA Cream 5% provides dermal anaesthesia through the release of lidocaine and prilocaine from the cream into the epidermal and dermal layers of the skin and the accumulation of lidocaine and prilocaine in the vicinity of dermal pain receptors and nerve endings. Lidocaine and prilocaine are amide-type local anaesthetic agents. They both stabilize neuronal membranes by inhibiting the ionic fluxes required for the initiation and conduction of impulses, thereby producing local anaesthesia.
The quality of anaesthesia depends upon the application time and the dose.
EMLA Cream is applied to intact skin under an occlusive dressing. The time needed to achieve reliable anaesthesia of intact skin is 1-2 hours, depending on the type of procedure.
In clinical studies of EMLA on intact skin, no differences in safety or efficacy (including anaesthetic onset time) were observed between geriatric patients (aged 65-96 years) and younger patients.
The duration of anaesthesia following the application of EMLA Cream for 1-2 hours is at least 2 hours after removal of the dressing.
The depth of cutaneous anaesthesia increases with application time. In 90% of patients the anaesthesia is sufficient for the insertion of a biopsy punch (4 mm diameter) to a depth of 2 mm after 60 min and 3 mm after 120 min EMLA treatment. EMLA is equally effective and has the same anaesthetic onset time across the range of light to dark pigmented skin (skin types I to VI).
The use of EMLA prior to measles-mumps-rubella or intramuscular diphtheria-pertussis-tetanus-inactivated poliovirus-Haemophilus influenzae b or Hepatitis B vaccines does not affect mean antibody titres, rate of seroconversion, or the proportion of patients achieving protective or positive antibody titres post immunization, as compared to placebo-treated patients.
Absorption from the genital mucosa is more rapid and onset time is shorter than after application to the skin.
After a 5-10 min application of EMLA to female genital mucosa the average duration of effective analgesia to an argon laser stimulus which produced a sharp, pricking pain was 15-20 min (individual variations in the range 5-45 min).
Reliable anaesthesia for the cleansing of leg ulcers is achieved after an application time of 30 minutes in most patients. An application time of 60 minutes may improve the anaesthesia further. The cleansing procedure should start within 10 minutes of removal of the cream. Clinical data from a longer waiting period are not available. EMLA reduces the postoperative pain for up to 4 hours after debridement. EMLA reduces the number of cleansing sessions required to achieve a clean ulcer compared to debridement with placebo cream. No negative effects on ulcer healing or bacterial flora have been observed.
EMLA produces a biphasic vascular response involving initial vasoconstriction followed by vasodilatation at the application site (see Adverse Reactions). Irrespective of the vascular response, EMLA facilitates the needle procedure compared to placebo cream.
In patients with atopic dermatitis, a similar but shorter vascular reaction is seen, with erythema occurring after 30-60 minutes, indicating more rapid absorption through the skin (see Precautions).
Pharmacokinetics: The systemic absorption of lidocaine and prilocaine from EMLA is dependent upon the dose, area of application and application time. Additional factors include thickness of the skin (which varies in different areas of the body), other conditions such as skin diseases, and shaving. Following application to leg ulcers, the characteristics of the ulcers may also affect the absorption.
Intact skin: Following application to the thigh in adults (60 g cream/400 cm2 for 3 hours), the extent of absorption was approx 5% of lidocaine and prilocaine. Maximum plasma concentrations (mean 0.12 and 0.07 μg/ml) were reached approx 2-6 hours after application.
The extent of systemic absorption was approx 10% following application to the face (10 g/100 cm2 for 2 hours). Maximum plasma levels (mean 0.16 and 0.06 μg/ml) were reached after approx 1.5-3 hours.
Plasma levels of lidocaine and prilocaine in both geriatric and non-geriatric patients following application of EMLA to intact skin are very low and well below potentially toxic levels.
Children: Following the application of 1.0 g EMLA Cream in neonates below 3 months of age, to approx 10 cm2 for one hour, the maximum plasma concentrations of lidocaine and prilocaine were 0.135 μg/ml and 0.107 μg/ml respectively. Following the application of 2.0 g EMLA Cream in infants between 3 and 12 months of age, to approx 16 cm2 for four hours, the maximum plasma concentrations of lidocaine and prilocaine were 0.155 μg/ml and 0.131 μg/ml respectively. Following the application of 10.0 g of EMLA Cream in children between 2 and 3 years of age, to approx 100 cm2 for two hours, the maximum plasma concentrations of lidocaine and prilocaine were 0.315 μg/ml and 0.215 μg/ml respectively. Following the application of 10.0-16.0 g EMLA Cream in children between 6 and 8 years of age, to approx 100-160 cm2 for two hours, the maximum plasma concentrations of lidocaine and prilocaine were 0.299 μg/ml and 0.110 μg/ml respectively.
Genital mucosa: After the application of 10 g EMLA Cream for 10 minutes to vaginal mucosa, maximum plasma concentrations of lidocaine and prilocaine (mean 0.18 μg/ml and 0.15 μg/ml respectively) were reached after 20-45 minutes.
Leg ulcer: Following a single application of 5 to 10 g of EMLA Cream to leg ulcers with an area of up to 64 cm2 for 30 minutes, the maximum plasma levels of lidocaine (range 0.05-0.25 μg/ml, one individual value of 0.84 μg/ml) and of prilocaine (0.02-0.08 μg/ml) were reached within 1-2.5 hours.
After an application time of 24 hours to leg ulcers with an area of up to 50-100 cm2, the maximum plasma levels of lidocaine (0.19-0.71 μg/ml) and of prilocaine (0.06-0.28 μg/ml) were usually reached within 2-4 hours.
Following repeated application of 2-10 g EMLA Cream to leg ulcers with an area of up to 62 cm2 for 30-60 minutes 3-7 times a week for up to 15 doses during a period of one month, there was no apparent accumulation in plasma of lidocaine and its metabolites monoglycinexylidide and 2,6-xylidine or of prilocaine and its metabolite ortho-toluidine. The maximum observed plasma levels for lidocaine, monoglycinexylidide and 2,6-xylidine were 0.41, 0.03 and 0.01 μg/ml respectively. The maximum observed plasma levels for prilocaine and ortho-toluidine were 0.08 μg/ml and 0.01 μg/ml respectively.
Toxicology: Preclinical safety data: In animal studies the toxicity noted after high doses of either lidocaine or prilocaine, alone or in combination, consisted of effects on the central nervous and cardiovascular systems. When lidocaine and prilocaine were combined, only additive effects were seen, with no indication of synergism or unexpected toxicity. Both compounds were shown to have a low oral acute toxicity, providing a good safety margin in the event that EMLA is inadvertently swallowed. No drug-related adverse effects were seen in the reproduction toxicity studies, using either compound separately or together.
Neither local anaesthetic showed a mutagenic potential in either in vitro or in vivo mutagenicity tests. Cancer studies have not been performed with either lidocaine or prilocaine alone or in combination, due to the indication and duration of therapeutic use of these drugs.
A metabolite of lidocaine, 2,6-dimethylaniline, and a metabolite of prilocaine, o-toluidine, showed evidence of mutagenic activity. These metabolites have been shown to have carcinogenicity potential in preclinical toxicological studies evaluating chronic exposure. Risk assessments comparing the calculated maximum human exposure from intermittent use of lidocaine and prilocaine, with the exposure used in preclinical studies, indicate a wide margin of safety for clinical use.
Local tolerance studies using a 1:1 (w/w) mixture of lidocaine and prilocaine as an emulsion, cream or gel indicated that these formulations are well tolerated by intact and damaged skin and mucosal membranes.
A marked irritative reaction was seen after single ocular administration of a 50 mg/g lidocaine + prilocaine 1:1 (w/w) emulsion, in an animal study. This is the same concentration of local anaesthetics and a similar formulation as for EMLA cream and patch. This ocular reaction may have been influenced by the high pH of the formulation of the emulsion (approximately 9), but is probably also partly a result of the irritative potential of the local anaesthetics themselves.
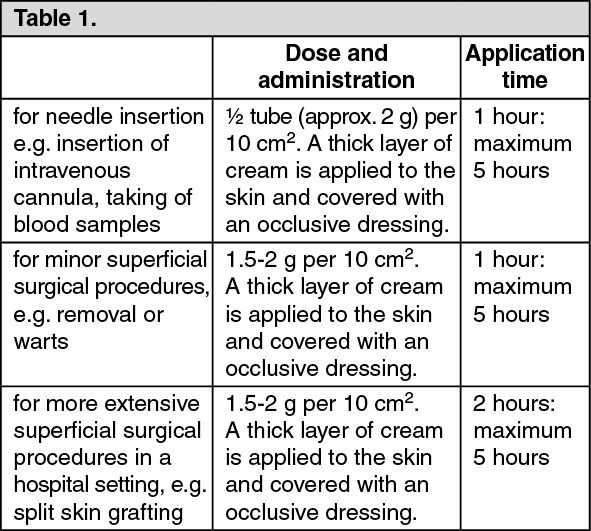
Surface anaesthesia of the skin in connection with needle insertion and for superficial surgical procedures.
Surface anaesthesia of leg ulcers prior to cleaning and superficial surgical procedures e.g., removal of fibrin, pus and necroses.
Surface anaesthesia of the genital mucosa.
Adults: Intact Skin:
(See Table 1.)
 Click on icon to see table/diagram/image
Leg ulcers:
Click on icon to see table/diagram/image
Leg ulcers: For cleaning of leg ulcers: approx. 1-2 g per 10 cm
2. The cream is applied in a thick layer to the surface of the ulcer, but not more than 10 g per treatment occasion. Cover the ulcer surface with an occlusive dressing.
An opened tube is intended for single use, and left-over cream should therefore be discarded after each treatment occasion.
Application time: at least 30 minutes.
For leg ulcers with tissue that is especially difficult to penetrate, the application time may be extended to 60 minutes. Cleaning of the ulcer should be begun within 10 minutes after removal of the cream.
EMLA has been used on up to 15 treatment occasions during a 1-2 month period without a reduction in effect or increase in the number of local reactions.
Genital use: Skin: Use before injection of local anaesthetics: Men: 1 g per 10 cm
2. A thick layer of cream is applied to the skin.
Application time: 15 minutes.
Women: 1-2 g per 10 cm
2. A thick layer of cream is applied to the skin.
Application time: 60 minutes.
Mucosa: For removal of condylomata or before injection of local anaesthetics: Approximately 5-10 g, depending on the area treated. The whole surface including mucous membrane folds must be covered. Occlusion is not necessary.
Application time: 5-10 minutes.
The surgery may be begun immediately after removal of the cream.
Children:
For needle insertion, removal of mollusca and other minor superficial surgical procedures: 1 g per 10 cm
2. A thick layer of cream is applied to the skin and covered with an occlusive dressing.
The dose should not exceed 1 gram per 10 cm
2 and should be adjusted according to the application area. (See Table 2.)
Click on icon to see table/diagram/image
Children with atopic dermatitis: Reduced application time to 30 minutes.
Rare cases of clinically significant methaemoglobinaemia have been reported. Prilocaine in high doses may cause an increase in the methaemoglobin level particularly in conjunction with methaemoglobin-inducing agents (e.g., sulphonamides). Clinically significant methaemoglobinaemia should be treated with a slow intravenous injection of methylene blue. Should other symptoms of systemic toxicity occur, the signs are anticipated to be similar in nature to those following the administration of local anaesthetics by other routes. Local anaesthetic toxicity is manifested by symptoms of nervous system excitation and, in severe cases, central nervous and cardiovascular depression.
Severe neurological symptoms (convulsions, CNS depression) must be treated symptomatically by respiratory support and the administration of anticonvulsive drugs.
Known hypersensitivity to local anaesthetics of the amide type or to any other excipients.
Patients with glucose-6-phosphate dehydrogenase deficiency or congenital or idiopathic methaemoglobinaemia are more susceptible to drug-induced methaemoglobinaemia.
Due to insufficient data on absorption, EMLA should not be applied to open wounds other than leg ulcers.
Studies have been unable to demonstrate the efficacy of EMLA for heel lancing in neonates.
Care should be taken when applying EMLA to patients with atopic dermatitis. A shorter application time, 15-30 minutes, may be sufficient (see Pharmacology: Pharmacodynamics under Actions).
Prior to curettage of mollusca in children with atopic dermatitis, an application time of 30 minutes is recommended.
EMLA should not be applied to the genital mucosa of children owing to insufficient data on absorption. However, when used in neonates for circumcision, a dose of 1.0 g EMLA on the prepuce has proven to be safe.
Care should be taken not to allow EMLA to come in contact with the eyes as it may cause eye irritation (see Pharmacology: Toxicology: Preclinical Safety Data under Actions). Also the loss of protective reflexes may allow corneal irritation and potential abrasion. If eye contact occurs, immediately rinse the eye in water or sodium chloride solution and protect it until sensation returns.
EMLA should not be applied to an impaired tympanic membrane. Tests on laboratory animals have shown that EMLA Cream has an ototoxic effect when instilled into the middle ear. Animals with an intact tympanic membrane, however, show no abnormality when exposed to EMLA Cream in the external auditory canal.
In children/neonates younger than 3 months a transient, clinically insignificant increase in methaemoglobin level is commonly observed up to 12 hours after an application of EMLA.
Patients treated with anti-arrhythmic drugs class III (eg, amiodarone) should be under close surveillance and ECG monitoring considered, since cardiac effects may be additive.
Lidocaine and prilocaine have bacteriocidal and antiviral properties in concentrations above 0.5-2%. For this reason, although one clinical study suggests that the immunization response is not affected when EMLA is used prior to BCG vaccination, the results of intracutaneous injections of live vaccines should be monitored.
Until further clinical data are available, EMLA should not be used in the following cases: (a) in infants between 0 and 12 months of age receiving treatment with methaemoglobin-inducing agents; (b) in preterm infants with a gestational age less than 37 weeks.
Effects on the ability to drive and use machines: Not applicable at the recommended dosage.
Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development.
Use in Pregnancy: In both animal and humans, lidocaine and prilocaine cross the placental barrier and may be absorbed by the foetal tissues. It is reasonable to assume that lidocaine and prilocaine have been used in a large number of pregnant women and women of childbearing potential. No specific disturbances to the reproductive process have so far been reported e.g., an increased incidence of malformations or other directly or indirectly harmful effects on the foetus. However, caution should be exercised when used in pregnant women.
Use in Lactation: Lidocaine and, in all probability, prilocaine are excreted in breast milk, but in such small quantities that there is generally no risk of the child being affected at therapeutic dose levels.
FREQUENCY OF ADVERSE EVENTS: (See Table 3.)
Click on icon to see table/diagram/image
Prilocaine in high doses may cause an increase in the methaemoglobin level particularly in conjunction with methaemoglobin-inducing agents (e.g., sulphonamides).
With large doses of EMLA, consideration should be given to the risk of additional systemic toxicity in patients receiving other local anaesthetics or agents structurally related to local anaesthetics, since the toxic effects are additive.
Specific interaction studies with lidocaine/prilocaine and anti-arrhythmic drugs class III (e.g., amiodarone) have not been performed, but caution is advised (see Precautions).
Drugs that reduce the clearance of lidocaine (e.g., cimetidine or betablockers) may cause potentially toxic plasma concentrations when lidocaine is given in repeated high doses over a long time period. Such interactions should therefore be of no clinical importance following short term treatment with lidocaine (e.g., EMLA cream) at recommended doses.
Instructions for use and handling and for disposal: Use the tube cap to puncture the membrance over the tip of the tube.
Incompatibilities: Not relevant.
Do not store above 30°C. Do not freeze.
Shelf-Life: 3 years.
N01BB52 - lidocaine, combinations ; Belongs to the class of amides. Used as local anesthetics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image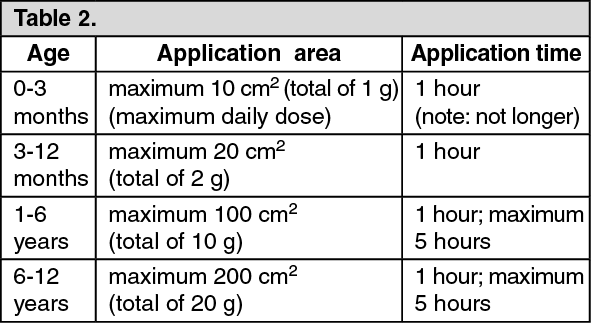 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image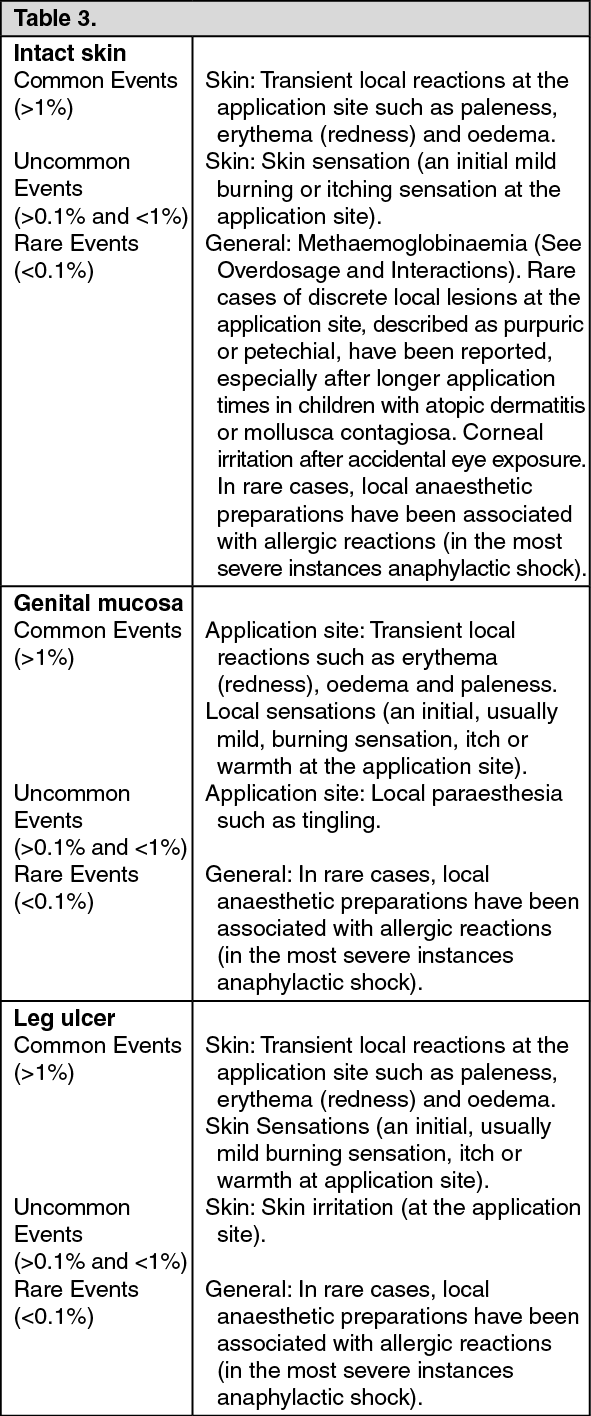 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
