Pharmacotherapeutic group: sex hormones and modulators of the genital system, gonadotropins.
ATC code: G03GA09.
Pharmacology: Pharmacodynamics: Corifollitropin alfa is designed as a sustained follicle stimulant with the same pharmacodynamic profile as (rec)FSH, but with a markedly prolonged duration of FSH activity. Due to its ability to initiate and sustain multiple follicular growth for an entire week, a single subcutaneous injection of the recommended dose of Elonva may replace the first seven injections of any daily (rec)FSH preparation in a COS treatment cycle. The long duration of FSH activity was achieved by adding the carboxy-terminal peptide of the β-subunit of human chorionic gonadotropin (hCG) to the β-chain of human FSH. Corifollitropin alfa does not display any intrinsic LH/hCG activity.
Clinical trial information: In three randomized, double-blind, clinical trials (ENSURE, ENGAGE, and PURSUE), treatment with a single subcutaneous injection of Elonva, 100 micrograms (ENSURE study) or 150 micrograms (ENGAGE and PURSUE study), for the first seven days of COS was compared to treatment with a daily dose of 150, 200, or 300 IU of recFSH, respectively. Pituitary suppression with a GnRH antagonist (ganirelix acetate injection at a daily dose of 0.25 mg) was used in each of the three clinical trials.
In the ENSURE study, 396 healthy normal ovulatory women, aged 18 to 36 years with a body weight less than or equal to 60 kg, were treated for one cycle with 100 micrograms of Elonva and pituitary suppression with a GnRH antagonist as part of an ART program. The primary efficacy endpoint was number of oocytes retrieved. The median total duration of stimulation was 9 days for both groups, indicating that two days of recFSH were required to complete ovarian stimulation from stimulation day 8 onwards (recFSH was given on the day of hCG for this study).
In the ENGAGE Study, 1,506 healthy normal ovulatory women, aged 18 to 36 years with a body weight greater than 60 kg and less than or equal to 90 kg, were treated for one cycle with 150 micrograms of Elonva and pituitary suppression with a GnRH antagonist as part of an ART program. The co-primary efficacy endpoints were ongoing pregnancy rate and number of oocytes retrieved. The median total duration of stimulation was 9 days for both groups, indicating that two days of recFSH were required to complete ovarian stimulation from stimulation day 8 onwards (recFSH was given on the day of hCG for this study).
In the PURSUE study, 1,390 healthy normal ovulatory women, aged 35 to 42 years with a body weight greater than or equal to 50 kg, were treated for one cycle with 150 micrograms of Elonva and pituitary suppression with a GnRH antagonist as part of an ART program. The primary efficacy endpoint was vital pregnancy rate. The number of oocytes retrieved was a key secondary efficacy endpoint. The median total duration of stimulation was 9 days for both groups, indicating that one day of recFSH was required to complete ovarian stimulation from stimulation day 8 onwards (no recFSH was given on the day of hCG for this study).
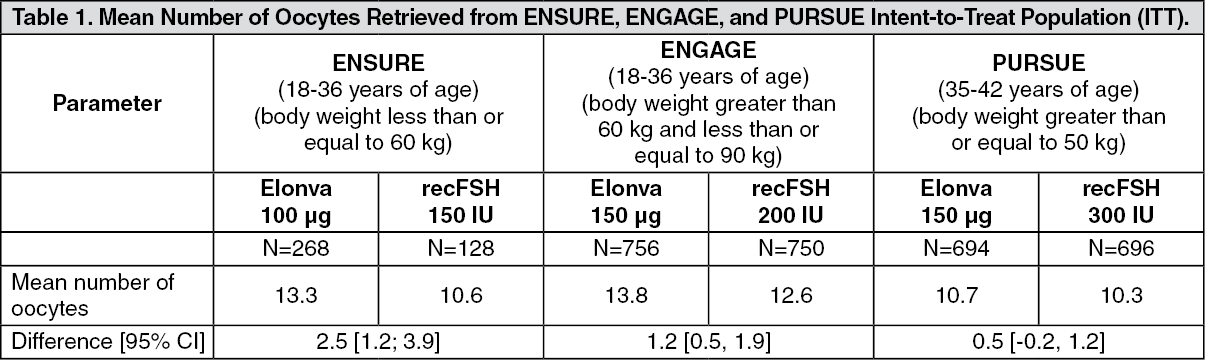
Number of oocytes retrieved: In all three studies, treatment with a single injection of Elonva, 100 or 150 micrograms, for the first seven days of COS, resulted in a higher number of oocytes retrieved compared with a daily dose of recFSH. However, the differences were within the predefined equivalence (ENGAGE and ENSURE) or non-inferiority (PURSUE) margins. See Table 1 as follows.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pregnancy from the fresh cycles of ENGAGE and PURSUE: In the ENGAGE study, non-inferiority was demonstrated in ongoing pregnancy rates between Elonva and recFSH, with ongoing pregnancy rate defined as presence of at least one foetus with heart activity assessed at least 10 weeks after embryo transfer.
In the PURSUE study, non-inferiority was demonstrated in vital pregnancy rate between Elonva and recFSH, with vital pregnancy rate defined as the percentage of subjects with at least one foetus with heart activity assessed 5 to 6 weeks after embryo transfer.
The pregnancy results from the fresh cycles of ENGAGE and PURSUE are summarized in Table 2 as follows.
Click on icon to see table/diagram/image
In these clinical trials, the safety profile of a single injection with Elonva was comparable to daily injections with recFSH.
Pregnancy from the Frozen-Thawed Embryo Transfer (FTET) cycles of ENGAGE and PURSUE: The follow-up FTET trial for ENGAGE included women who had at least one embryo thawed for use up to at least one year after cryopreservation. The mean number of embryos transferred in the FTET cycles of ENGAGE was 1.7 in both treatment groups.
The follow-up FTET trial for PURSUE included women who had at least one embryo thawed for use within two years of the date of the last cryopreservation for this trial. The mean number of embryos transferred in the FTET cycles of PURSUE was 2.4 in both treatment groups. This trial also provided safety data on the infants born from cryopreserved embryos.
The pregnancy results from the FTET cycles of ENGAGE and PURSUE are summarized in Table 3 as follows.
Click on icon to see table/diagram/image
Pregnancy from the addition of FTET cycles to the fresh cycles of ENGAGE and PURSUE (Cumulative Vital Pregnancy Rates): The cumulative vital pregnancy rate (per subject and per cycle) was calculated based on the results of the fresh and subsequent FTET cycles of a single cohort of women who received Elonva or recFSH in ENGAGE or PURSUE.
The cumulative vital pregnancy rate from ENGAGE in subjects treated with a single injection of 150 μg Elonva was similar to that in subjects treated with daily 200 IU recFSH.
The cumulative vital pregnancy rate from PURSUE in subjects treated with a single injection of 150 μg Elonva was similar to that in subjects treated with daily 300 IU recFSH.
The pregnancy results are summarized in Table 4 as follows.
Click on icon to see table/diagram/image
Congenital malformations reported in infants born after a frozen-thawed embryo transfer (FTET) cycle: Following use of Elonva, 61 infants were born after an FTET cycle in the PURSUE study follow-up, and 607 infants were born after fresh ART cycles in the ENSURE, ENGAGE and PURSUE studies combined. The rates for congenital malformations (major and minor combined) reported for infants born after an FTET cycle in the PURSUE study follow-up (16.4%) were similar to those reported for infants born after fresh ART cycles in the ENSURE, ENGAGE and PURSUE studies combined (16.8%).
Immunogenicity: Of the 2,511 women treated with Elonva who were evaluated for the formation of post-treatment antibodies, four (0.16%) had evidence of antibody formation, including three who had been exposed once to Elonva and one who had been exposed twice to Elonva. In each case, these antibodies were non-neutralizing and did not interfere with the response to stimulation or the normal physiologic responses of the Hypothalamic-Pituitary-Ovarian (HPO) axis. Two of these four women became pregnant during the same treatment cycle in which antibodies were detected, suggesting that the presence of non-neutralizing antibodies after stimulation with Elonva is not clinically relevant.
Cardiac Electrophysiology: In a randomized, double-blind, placebo- and active-controlled, 4-period crossover study, 70 healthy postmenopausal women received a single therapeutic dose of 150 mcg of corifollitropin alfa subcutaneously, a single supratherapeutic dose of 240 mcg of corifollitropin alfa subcutaneously, 400 mg moxifloxacin orally, and placebo. Both doses of corifollitropin alfa did not appear to prolong the QTc interval for up to 216 hours postdose. After baseline and placebo adjustment, the maximum mean QTc interval change after administration of a therapeutic dose of 150 mcg of corifollitropin alfa was 1.4 msec (1-sided 95% upper CI: 3.4 msec). After administration of the supratherapeutic dose of 240 mcg of corifollitropin alfa, the maximum mean QTc interval change was 1.2 msec (1-sided 95% upper CI: 3.6 msec).
Pharmacokinetics: Pharmacokinetic parameters of corifollitropin alfa were evaluated after subcutaneous administration in women undergoing a COS treatment cycle.
Due to the long elimination half-life, after administration of the recommended dose, serum concentrations of corifollitropin alfa are sufficient to sustain multiple follicular growth for an entire week. Therefore, a single subcutaneous injection of Elonva may be used as an alternative to the first seven days of daily rec(FSH) in COS for the development of multiple follicles and pregnancy in an ART program (see Dosage & Administration).
Body weight is a determinant of exposure to corifollitropin alfa. The mean corifollitropin alfa exposure (AUC) after a single subcutaneous injection is 665 hours*ng/mL (426-1,037 hours*ng/mL
1) and is similar after administration of 100 micrograms corifollitropin alfa to women with a body weight less than or equal to 60 kilograms and of 150 micrograms corifollitropin alfa to women with a body weight greater than 60 kilograms.
Absorption: After a single subcutaneous injection of Elonva, the mean maximum serum concentration (C
max) of corifollitropin alfa is 4.24 ng/mL (2.49-7.21 ng/mL
1) and is reached at the mean T
max of 44 hours (35-57 hours
1) postdose. The absolute bioavailability is 58% (48-70%
1).
Distribution: Distribution, metabolism and elimination of corifollitropin alfa are very similar to other gonadotropins, such as FSH, hCG and LH. After absorption into the blood, corifollitropin alfa is distributed mainly to the ovaries and the kidneys. Elimination of corifollitropin alfa predominantly occurs via the kidneys. The steady state volume of distribution is 9.2 L (6.5-13.1 L
1). Exposure to corifollitropin alfa increases proportionally with dose within the range of 60 micrograms to 240 micrograms.
Elimination: Corifollitropin alfa has a mean elimination half-life (t
1/2) of 70 hours (59-82 hours
1) and a clearance of 0.13 L/h (0.10-0.18 L/h
1). Elimination of corifollitropin alfa predominantly occurs via the kidneys, and the rate of elimination may be reduced in patients with renal insufficiency (see Dosage & Administration and Precautions). Hepatic metabolism contributes to a minor extent to the elimination of corifollitropin alfa.
Other special populations: Hepatic impairment: Although data in hepatically impaired patients are not available, hepatic impairment is unlikely to affect the pharmacokinetic profile of corifollitropin alfa.
1Predicted range for 90% of subjects
Toxicology: Preclinical safety data: Preclinical data revealed no special hazard for humans based on conventional studies of single and repeated dose toxicity and safety pharmacology.
Reproduction toxicology studies in rats and rabbits indicated that corifollitropin alfa does not affect adversely fertility. Administration of corifollitropin alfa to rats and rabbits, prior to and directly after mating, and during early pregnancy, resulted in embryotoxicity. In rabbits, when administered prior to mating, teratogenicity has been observed. Both embryotoxicity and teratogenicity are considered a consequence of the superovulatory state of the animal not able to support a number of embryos above a physiological ceiling. The relevance of these findings for the clinical use of Elonva is limited.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image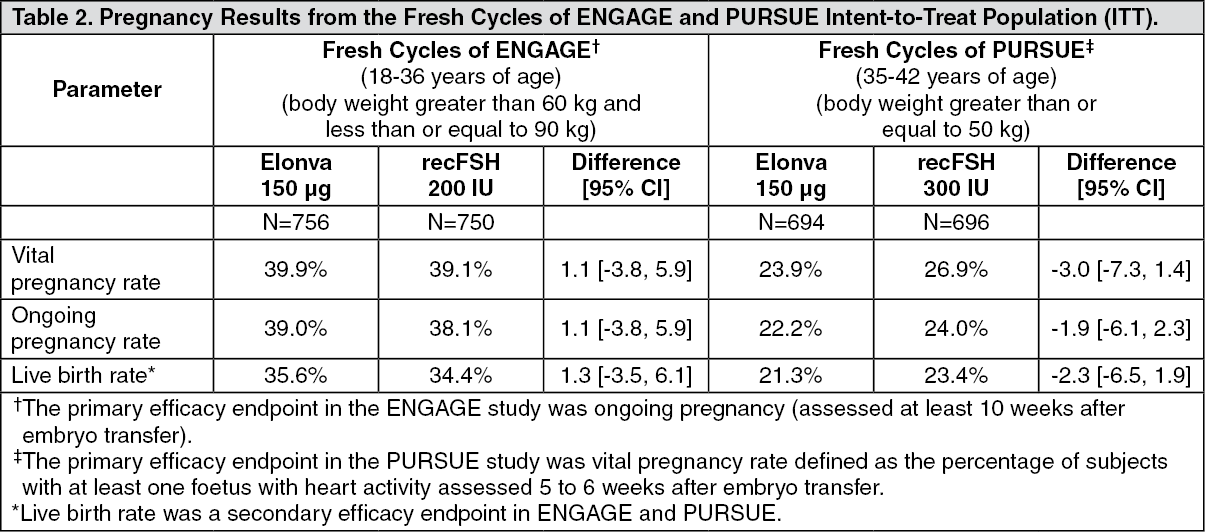 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image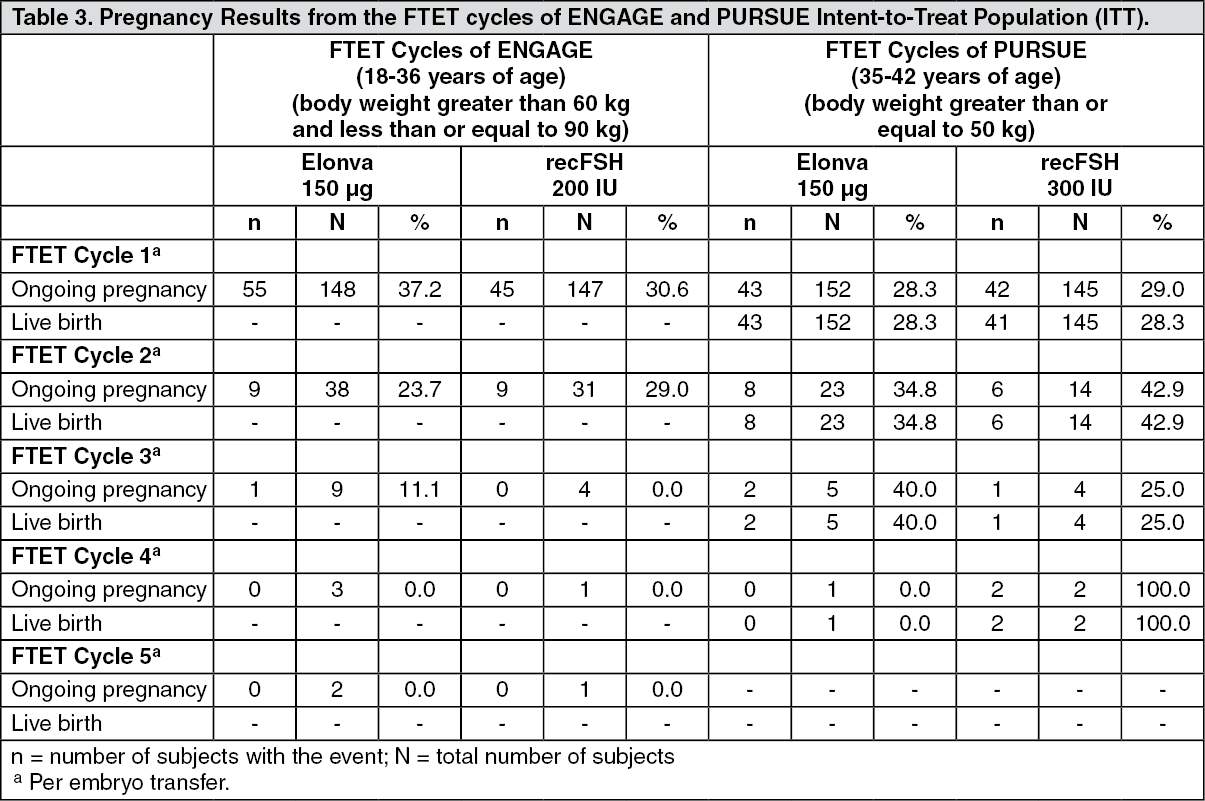 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image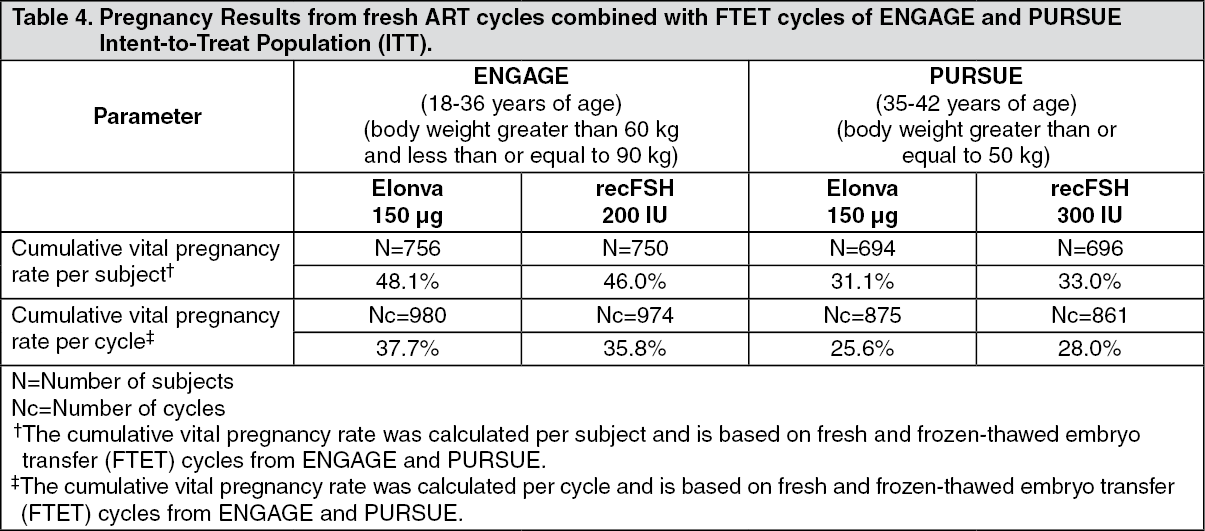 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 150 mcg_0.5 mL12a08368-17de-42ed-acc4-ad470112c219.GIF)

 Sign Out
Sign Out
