


 Sign Out
Sign Out

ELAPRASE is intended to provide exogenous enzyme for uptake into cellular lysosomes. Mannose-6- phosphate (M6P) residues on the oligosaccharide chains allow binding of the enzyme to the M6P receptors on the cell surface, leading to cellular internalization of the enzyme, targeting to intracellular lysosomes and subsequent catabolism of accumulated GAG.
Pharmacodynamics: Decreases in urinary GAG levels were observed following treatment with ELAPRASE. The responsiveness of urinary GAG to dosage alterations of ELAPRASE is unknown, and the relationship of urinary GAG to other measures of clinical response has not been established. Patients who tested positive for anti-idursulfase antibodies (Ab) experienced a less pronounced decrease in urinary GAG levels [see Adverse Reactions and Pharmacology: Pharmacodynamics: Clinical Studies as follows].
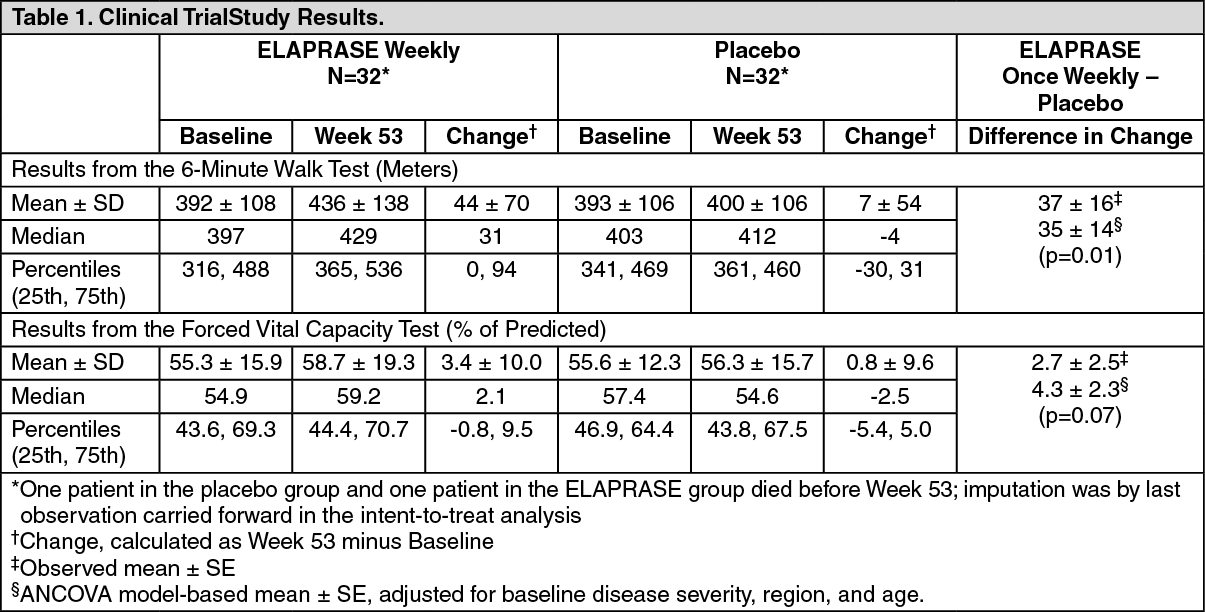
Clinical Studies: Clinical Trials in Patients 5 Years and Older: The safety and efficacy of ELAPRASE were evaluated in a 53-week, randomized, double-blind, placebo-controlled clinical trial of 96 patients with Hunter syndrome. The trial included patients with deficiency in iduronate-2-sulfatase enzyme activity and a percent predicted forced vital capacity (%-predicted FVC) less than 80%. The age of patients ranged from 5 to 31 years. Patients received ELAPRASE 0.5 mg/kg once per week (n = 32), ELAPRASE 0.5 mg/kg once every other week (n = 32), or placebo (n = 32).
The primary efficacy outcome assessment was a two-component composite score based on the sum of the ranks of the change from baseline to Week 53 in distance walked in six minutes (6-minute walk test) and the ranks of the change in %-predicted FVC. This two-component composite primary endpoint differed statistically significantly between the three groups, and the difference was greatest between the placebo group and the once weekly treatment group (once weekly ELAPRASE vs. placebo, p = 0.0049).
Examination of the individual components of the composite score showed that, in the adjusted analysis, the weekly ELAPRASE-treated group experienced a 35 meter greater mean increase in the distance walked in six minutes compared to placebo. The changes in %-predicted FVC were not statistically significant (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacodynamic assessments included urinary GAG levels and changes in liver and spleen size. Urinary GAG levels were elevated in all patients at baseline. Following 53 weeks of treatment, mean urinary GAG levels were markedly reduced in the ELAPRASE once weekly group, although GAG levels still remained above the upper limit of normal in half of the ELAPRASE-treated patients. Urinary GAG levels remained elevated and essentially unchanged in the placebo group. Sustained reductions in both liver and spleen volumes were observed in the ELAPRASE once weekly group through Week 53 compared to placebo. There were essentially no changes in liver and spleen volumes in the placebo group.
Extension Trial: Patients who participated in the placebo-controlled trial were eligible to continue treatment in an open-label extension trial. During the extension trial, all patients received ELAPRASE 0.5mg/kg once weekly for 24 months.
Patients who were treated with ELAPRASE once weekly and every other week in the placebo-controlled trial demonstrated improvement in distance walked in the 6-minute walk test for an additional 8 months of treatment in the extension trial. There was no change in mean %-predicted FVC in all Hunter syndrome patients after 6 months of treatment in the extension trial; however, a slight decrease in mean %-predicted FVC was demonstrated through to month 24 of the extension trial. The long-term effect of ELAPRASE on pulmonary function in Hunter syndrome patients is unclear.
There were no further reductions in mean urinary GAG levels in patients initially treated with ELAPRASE once weekly; however, the patients treated with ELAPRASE every other week during the placebo-controlled trial experienced further reductions in mean urinary GAG levels after changing to a more frequent dosing regimen during the extension trial. The persistence of reduced urinary GAG levels did not correlate with the long term effect demonstrated by the 6-minute walk test distance or %-predicted FVC.
Clinical Trial in Patients 7 Years and Younger: A 53-week, open-label, multicenter, single-arm trial was conducted to assess the safety, pharmacokinetics, and pharmacodynamics of ELAPRASE 0.5 mg/kg once weekly in male Hunter syndrome patients aged 7 years and younger. Safety results demonstrated that patients with complete gene deletion or large gene rearrangement mutations are more likely to develop antibodies, including neutralizing antibodies, and to experience hypersensitivity reactions with ELAPRASE administration [see Adverse Reactions]. In patients who remained antibody negative, the pharmacokinetic profile, reduction in urinary GAG excretion levels, and reduction in spleen volume were similar to those of adults and children 5 years and older. In patients who were persistently antibody positive, the presence of anti-idursulfase antibody was associated with reduced systemic exposure of idursulfase and a less pronounced decrease in urinary GAG levels [see Pharmacology as previously mentioned.].
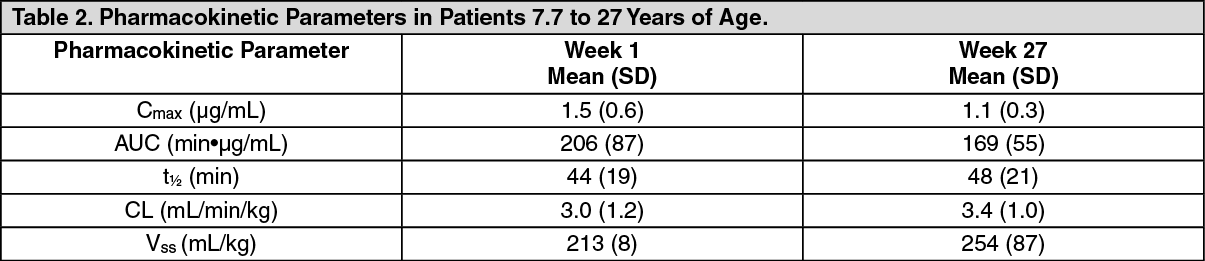
Pharmacokinetics: Clinical Trials in Patients 5 Years and Older: The pharmacokinetic characteristics of idursulfase were evaluated in 59 patients with Hunter syndrome. The serum concentration of idursulfase was quantified using an antigen-specific ELISA assay. The area under the concentration-time curve (AUC) increased in a greater than dose proportional manner as the dose increased from 0.15 mg/kg to 1.5 mg/kg following a single 1-hour infusion of ELAPRASE. The pharmacokinetic parameters at the recommended dose regimen (0.5 mg/kg ELAPRASE administered weekly as a 3-hour infusion) were determined at Week 1 and Week 27 in 10 patients ages 7.7 to 27 years (Table 3). There were no apparent differences in PK parameter values between Week 1 and Week 27 regardless of the antibody status in these patients. (See Table 2.)
 Click on icon to see table/diagram/image
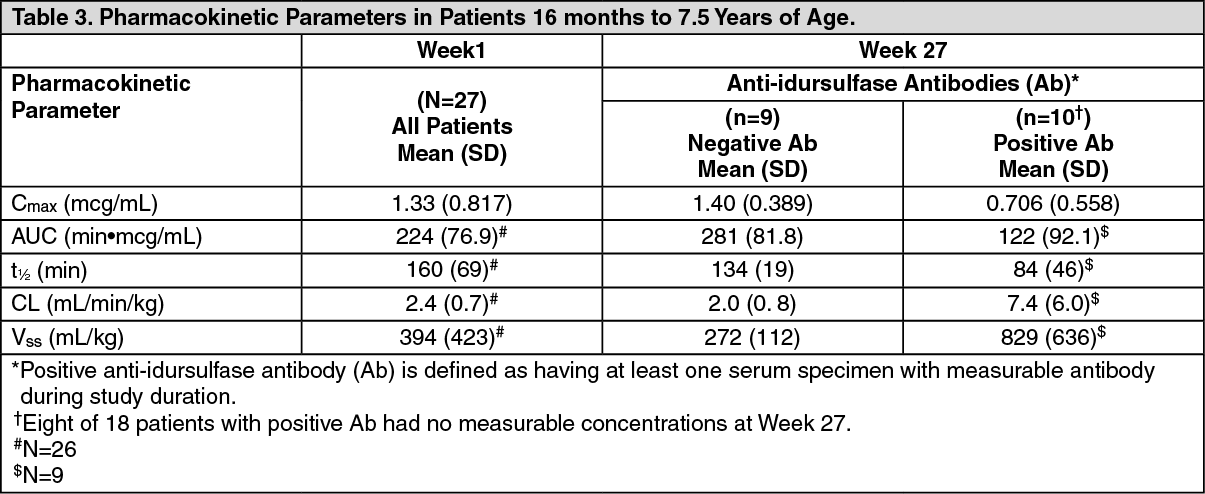
Click on icon to see table/diagram/imageClinical Trial in Patients 7 Years and Younger: Idursulfase pharmacokinetics was evaluated in 27 patients with Hunter syndrome 16 months to 7.5 years of age who received ELAPRASE 0.5 mg/kg once weekly as a 3-hour infusion. The presence of antiidursulfase antibody (Ab) was associated with a reduced systemic exposure of idursulfase. Eight of the 18 Ab-positive patients had no measurable idursulfase concentrations. An additional 9 Ab-positive patients had decreased Cmax, AUC, and t1/2 at Week 27 compared to Week 1 (Table 3). Idursulfase pharmacokinetics was similar between Week 1 and Week 27 in Ab-negative patients (Table 3). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAll patients with the complete gene deletion or large gene rearrangement genotype (n = 8) developed Ab at Week 27. Five of these eight patients had no measurable idursulfase concentrations at Week 27, and three had a lower systemic exposure at Week 27 compared to Week 1.
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Long-term studies in animals to evaluate carcinogenic potential or studies to evaluate mutagenic potential have not been performed with ELAPRASE.
ELAPRASE at intravenous doses up to 5 mg/kg, administered twice weekly (about 1.6 times the recommended human weekly dose based on body surface area) had no effect on fertility and reproductive performance in male rats.