


 Sign Out
Sign Out


Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adults with Atopic Dermatitis: Three randomized, double-blind, placebo-controlled, multicenter trials (SOLO 1, SOLO 2, and CHRONOS) and one dose-ranging trial (AD-1021) evaluated the safety of DUPIXENT in subjects with moderate-to-severe atopic dermatitis. The safety population had a mean age of 38 years; 41% of subjects were female, 67% were white, 24% were Asian, and 6% were black; in terms of comorbid conditions, 48% of the subjects had asthma, 49% had allergic rhinitis, 37% had food allergy, and 27% had allergic conjunctivitis. In these 4 trials, 1472 subjects were treated with subcutaneous injections of DUPIXENT, with or without concomitant topical corticosteroids (TCS).
A total of 739 subjects were treated with DUPIXENT for at least 1 year in the development program for moderate-to-severe atopic dermatitis.
SOLO 1, SOLO 2, and AD-1021 compared the safety of DUPIXENT monotherapy to placebo through Week 16. CHRONOS compared the safety of DUPIXENT + TCS to placebo + TCS through Week 52.
Weeks 0 to 16 (SOLO 1, SOLO 2, CHRONOS, and AD-1021): In DUPIXENT monotherapy trials (SOLO 1, SOLO 2, and AD-1021) through Week 16, the proportion of subjects who discontinued treatment because of adverse events was 1.9% in both the DUPIXENT 300 mg Q2W and placebo groups.
Table 15 summarizes the adverse reactions that occurred at a rate of at least 1% in the DUPIXENT 300 mg Q2W monotherapy groups, and in the DUPIXENT + TCS group, all at a higher rate than in their respective comparator groups during the first 16 weeks of treatment. (See Table 14.)
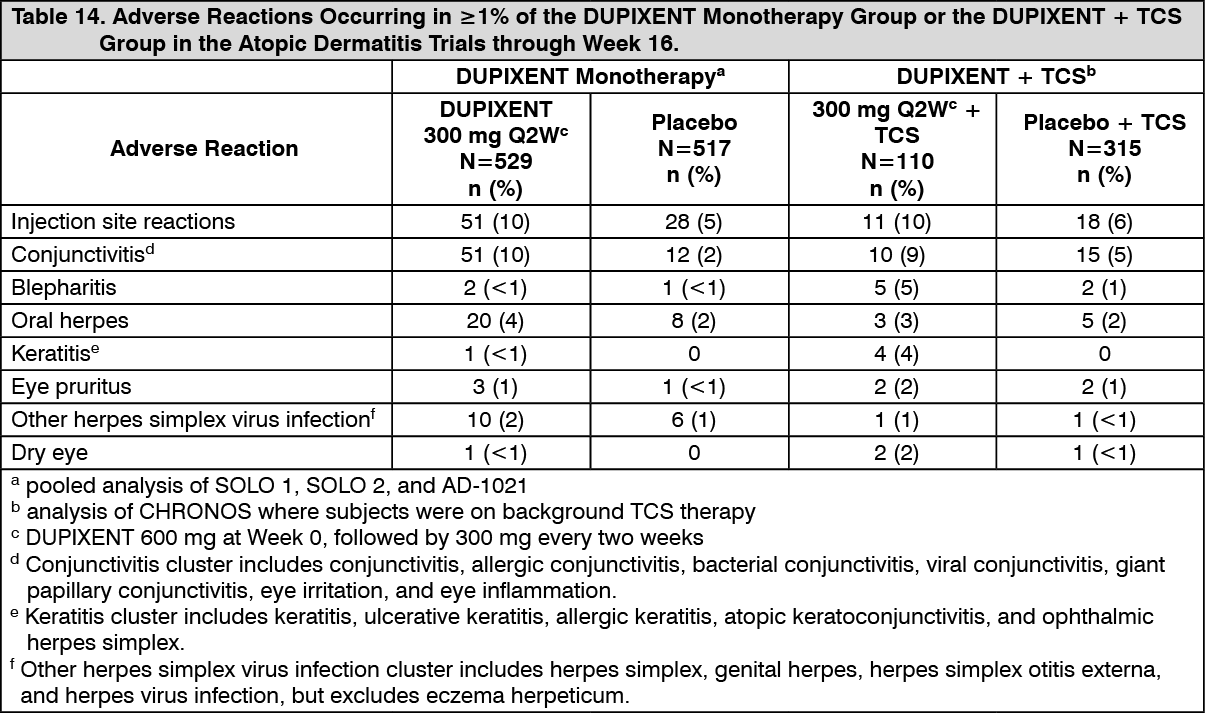 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSafety through Week 52 (CHRONOS): In the DUPIXENT with concomitant TCS trial (CHRONOS) through Week 52, the proportion of subjects who discontinued treatment because of adverse events was 1.8% in DUPIXENT 300 mg Q2W + TCS group and 7.6% in the placebo + TCS group. Two subjects discontinued DUPIXENT because of adverse reactions: atopic dermatitis (1 subject) and exfoliative dermatitis (1 subject).
The safety profile of DUPIXENT + TCS through Week 52 was generally consistent with the safety profile observed at Week 16.
Pediatric Subjects 12 to 17 Years of Age with Atopic Dermatitis: The safety of DUPIXENT was assessed in a trial of 250 pediatric subjects 12 to 17 years of age with moderate-to-severe atopic dermatitis (AD-1526). The safety profile of DUPIXENT in these subjects through Week 16 was similar to the safety profile from studies in adults with atopic dermatitis.
The long-term safety of DUPIXENT was assessed in an open-label extension study in subjects 12 to 17 years of age with moderate-to-severe atopic dermatitis (AD-1434). The safety profile of DUPIXENT in subjects followed through Week 52 was similar to the safety profile observed at Week 16 in AD-1526. The long-term safety profile of DUPIXENT observed in pediatric subjects 12 to 17 years of age was consistent with that seen in adults with atopic dermatitis.
Pediatric Subjects 6 to 11 Years of Age with Atopic Dermatitis: The safety of DUPIXENT with concomitant TCS was assessed in a trial of 367 subjects 6 to 11 years of age with severe atopic dermatitis (AD-1652). The safety profile of DUPIXENT + TCS in these subjects through Week 16 was similar to the safety profile from trials in adults and pediatric subjects 12 to 17 years of age with atopic dermatitis.
The long-term safety of DUPIXENT ± TCS was assessed in an open-label extension study of 368 pediatric subjects 6 to 11 years of age with atopic dermatitis (AD-1434). Among subjects who entered this study, 110 (30%) had moderate and 72 (20%) had severe atopic dermatitis at the time of enrollment in AD-1434. The safety profile of DUPIXENT ± TCS in subjects followed through Week 52 was similar to the safety profile observed through Week 16 in AD-1562. The long-term safety profile of DUPIXENT ± TCS observed in pediatric subjects 6 to 11 years of age was consistent with that seen in adults and pediatric subjects 12 to 17 years of age with atopic dermatitis [see Use in Children under Precautions].
Pediatric Subjects 6 Months to 5 Years of Age with Atopic Dermatitis: The safety of DUPIXENT with concomitant TCS was assessed in a trial of 161 pediatric subjects 6 months to 5 years of age with moderate-to-severe atopic dermatitis (AD-1539). The safety profile of DUPIXENT + TCS in these subjects through Week 16 was similar to the safety profile from trials in adults and pediatric subjects 6 to 17 years of age with atopic dermatitis.
The long-term safety of DUPIXENT ± TCS was assessed in an open-label extension study of 180 pediatric subjects 6 months to 5 years of age with atopic dermatitis (AD-1434). The majority of subjects were treated with DUPIXENT 300 mg every 4 weeks. The safety profile of DUPIXENT ± TCS in subjects followed through Week 52 was similar to the safety profile observed through Week 16 in AD-1539. The long-term safety profile of DUPIXENT ± TCS observed in pediatric subjects 6 months to 5 years of age was consistent with that seen in adults and pediatric subjects 6 to 17 years old with atopic dermatitis. In addition, hand-foot-and-mouth disease was reported in 9 (5%) pediatric subjects and skin papilloma was reported in 4 (2%) pediatric subjects treated with DUPIXENT ± TCS. These cases did not lead to study drug discontinuation [see Use in Children under Precautions].
Asthma: A total of 2888 adult and pediatric subjects 12 to 17 years of age with moderate-to-severe asthma (AS) were evaluated in 3 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks duration (DRI12544, QUEST, and VENTURE). Of these, 2678 had a history of 1 or more severe exacerbations in the year prior to enrollment despite regular use of medium to high-dose inhaled corticosteroids plus an additional controller(s) (DRI12544 and QUEST). A total of 210 subjects with oral corticosteroid-dependent asthma receiving high-dose inhaled corticosteroids plus up to two additional controllers were enrolled (VENTURE).
The safety population (DRI12544 and QUEST) was 12-87 years of age, of which 63% were female, and 82% were white. DUPIXENT 200 mg or 300 mg was administered subcutaneously Q2W, following an initial dose of 400 mg or 600 mg, respectively.
In DRI12544 and QUEST, the proportion of subjects who discontinued treatment due to adverse events was 4% of the placebo group, 3% of the DUPIXENT 200 mg Q2W group, and 6% of the DUPIXENT 300 mg Q2W group.
Table 16 summarizes the adverse reactions that occurred at a rate of at least 1% in subjects treated with DUPIXENT and at a higher rate than in their respective comparator groups in DRI12544 and QUEST. (See Table 15.)
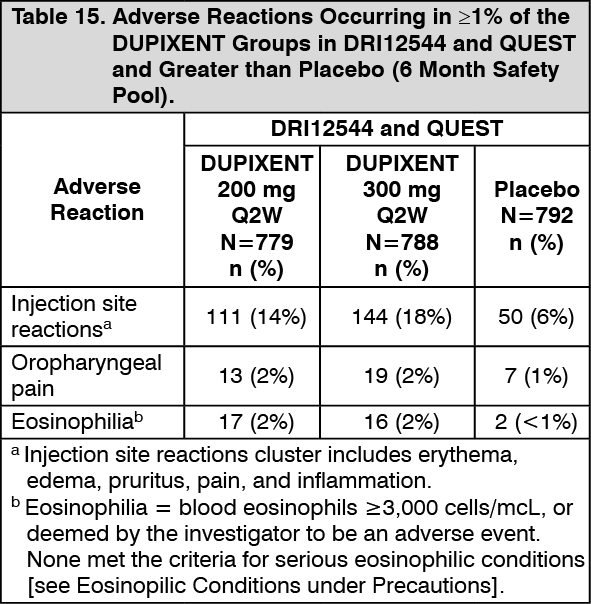 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe safety profile of DUPIXENT through Week 52 was generally consistent with the safety profile observed at Week 24.
Specific Adverse Reactions: Conjunctivitis and Keratitis: During the 52-week treatment period of concomitant therapy atopic dermatitis trial (CHRONOS), conjunctivitis was reported in 16% of the DUPIXENT 300 mg Q2W + TCS group (20 per 100 subject-years) and in 9% of the placebo + TCS group (10 per 100 subject-years). In DUPIXENT atopic dermatitis monotherapy trials (SOLO 1, SOLO 2, and AD-1021) through Week 16, keratitis was reported in <1% of the DUPIXENT group (1 per 100 subject-years) and in 0% of the placebo group (0 per 100 subject-years). In the 52-week atopic dermatitis DUPIXENT + topical corticosteroids (TCS) atopic dermatitis trial (CHRONOS), keratitis was reported in 4% of the DUPIXENT + TCS group (12 per 100 subject-years) and in 0% of the placebo + TCS group (0 per 100 subject-years). Most subjects with conjunctivitis or keratitis recovered or were recovering during the treatment period.
Among asthma subjects, the frequency of conjunctivitis was similar between DUPIXENT and placebo [see Conjunctivitis and Keratitis under Precautions].
Eczema Herpeticum and Herpes Zoster: The rate of eczema herpeticum was similar in the placebo and DUPIXENT groups in the atopic dermatitis trial.
Herpes zoster was reported in <0.1% of the DUPIXENT groups (<1 per 100 subject-years) and in <1% of the placebo group (1 per 100 subject-years) in the 16-week atopic dermatitis monotherapy trials. In the 52-week DUPIXENT + TCS atopic dermatitis trial, herpes zoster was reported in 1% of the DUPIXENT + TCS group (1 per 100 subject-years) and 2% of the placebo + TCS group (2 per 100 subject-years). Among asthma subjects the frequency of herpes zoster was similar between DUPIXENT and placebo.
Hypersensitivity Reactions: Hypersensitivity reactions were reported in <1% of DUPIXENT-treated subjects. These included serum sickness reaction, serum sickness-like reaction, and generalized urticaria, rash, erythema nodosum, and anaphylaxis [see Contraindications, Hypersensitivity under Precautions, and Immunogenicity as follows].
Eosinophils: DUPIXENT-treated subjects had a greater mean initial increase from baseline in blood eosinophil count compared to subjects treated with placebo. In adult subjects with atopic dermatitis, the mean and median increases in blood eosinophils from baseline to Week 4 were 100 and 0 cells/mcL respectively. In pediatric subjects <6 years old with atopic dermatitis, the mean and median increases from baseline to Week 4 were 478 and 90 cells/mcL, respectively. In adult and pediatric subjects 12 years of age and older with asthma, the mean and median increases in blood eosinophils from baseline to Week 4 were 130 and 10 cells/mcL, respectively.
Across all indications, the incidence of treatment-emergent eosinophilia (≥500 cells/mcL) was similar in DUPIXENT and placebo groups. Treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in <3% of DUPIXENT-treated patients and <0.5% in placebo-treated patients. Blood eosinophil counts declined to near baseline levels during study treatment. In study AD-1539, treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in 8% of DUPIXENT-treated subjects and 0% in placebo-treated subjects [see Eosinophilic Conditions under Precautions].
Cardiovascular: In the 1-year placebo-controlled trial in subjects with asthma (QUEST), cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.2%) of the DUPIXENT 200 mg Q2W group, 4 (0.6%) of the DUPIXENT 300 mg Q2W group, and 2 (0.3%) of the placebo group.
In the 1-year placebo-controlled trial in subjects with atopic dermatitis (CHRONOS), cardiovascular thromboembolic events (cardiovascular deaths, non-fatal myocardial infarctions, and non-fatal strokes) were reported in 1 (0.9%) of the DUPIXENT + TCS 300 mg Q2W group, 0 (0.0%) of the DUPIXENT + TCS 300 mg QW group, and 1 (0.3%) of the placebo + TCS group.
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to dupilumab in the studies described as follows with the incidence of antibodies in other studies or to other products may be misleading.
Approximately 5% of subjects with atopic dermatitis or asthma who received DUPIXENT 300 mg Q2W for 52 weeks developed antibodies to dupilumab; approximately 2% exhibited persistent ADA responses, and approximately 2% had neutralizing antibodies. Similar results were observed in pediatric subjects 6 months to 11 years of age with atopic dermatitis who received either DUPIXENT 200 mg Q2W, 200 mg Q4W, or 300 mg Q4W.
Approximately 16% of pediatric subjects 12 to 17 years of age with atopic dermatitis who received DUPIXENT 300 mg or 200 mg Q2W for 16 weeks developed antibodies to dupilumab; approximately 3% exhibited persistent ADA responses, and approximately 5% had neutralizing antibodies.
Approximately 9% of subjects with asthma who received DUPIXENT 200 mg Q2W for 52 weeks developed antibodies to dupilumab; approximately 4% exhibited persistent ADA responses, and approximately 4% had neutralizing antibodies.
Regardless of age or population, up to 4% of subjects in placebo groups were positive for antibodies to DUPIXENT; approximately 2% exhibited persistent ADA responses, and approximately 1% had neutralizing antibodies.
The antibody titers detected in both DUPIXENT and placebo subjects were mostly low. In subjects who received DUPIXENT, development of high titer antibodies to dupilumab was associated with lower serum dupilumab concentrations [see Pharmacology: Pharmacokinetics under Actions].
Two adult subjects who experienced high titer antibody responses developed serum sickness or serum sickness-like reactions during DUPIXENT therapy [see Hypersensitivity under Precautions].
View ADR Monitoring Form