Each film-coated tablet contains 10 mg dydrogesterone.
The score line is only to facilitate breaking for ease of swallowing and not to divide into equal doses.
Excipient(s) with known effect: Each tablet contains 111.1 mg Lactose monohydrate.
Excipients/Inactive Ingredients: Core: Lactose monohydrate, Hypromellose, Maize starch, Colloidal anhydrous silica, Magnesium stearate.
Film-Coating: Hypromellose, Macrogol 400, Titanium dioxide (E171).
Pharmacotherapeutic group: Genito-urinary system and sex hormones. ATC code: G03DB01.
Pharmacology: Pharmacodynamics: Mechanism of action: Dydrogesterone is an orally active progestogen which produces a complete secretory endometrium in an estrogen-primed uterus thereby providing protection against the increased risk for endometrium hyperplasia and/or carcinogenesis induced by estrogens. It is indicated in all cases of endogenous progesterone deficiency. Dydrogesterone has no estrogenic, no androgenic, no thermogenic, no anabolic and no corticoid activity.
Adolescent population: Limited clinical trial data indicate that dydrogesterone is efficacious in relieving symptoms of dysmenorrhoea, premenstrual syndrome, dysfunctional uterine bleeding and irregular cycles in the population of patients younger than 18 years of age in a similar manner as in the adult population.
Clinical efficacy and safety: Lotus I and Lotus II clinical study(s) confirmed the following: A Double-Blind, Double-Dummy, Randomized, Two-arm, Multicentre Study Comparing the Efficacy, Safety, and Tolerability of Oral Dydrogesterone 30 mg daily versus Intravaginal Micronized Progesterone Capsules 600 mg daily for Luteal Support in In-Vitro Fertilization (LOTUS I).
A randomized, Open-label, Two-arm, Multicenter Study Comparing the Efficacy, Safety and Tolerability of Oral Dydrogesterone 30 mg daily versus Crinone 8% intravaginal progesterone gel 90 mg daily for Luteal Support in In Vitro Fertilization (LOTUS II).
The primary objective of non-inferiority of oral dydrogesterone compared to intravaginal micronized progesterone in terms of the presence of fetal heartbeats at 12 weeks' gestation (week 10) was achieved.
In the studied patient population, pregnancy rates at 12 weeks' gestation (week 10) were 37.6% and 33.1% (LOTUS I) and 36.7% and 34.7% (LOTUS II). The difference in the pregnancy rate between the two groups was 4.7 (95% CI, -1.2; 10.6) (LOTUS I) and 2.0 (95% CI, -0.4; 0.8) (LOTUS II).
Within the safety sample of 1,029 subjects (LOTUS I) and 1030 subjects (LOTUS II) with at least one dose of study medication administered, the incidence of the most frequently reported TEAEs was similar between the two treatment groups.
Due to the nature of the indication and the studied patient population, a number of early abortions and miscarriages can be expected. Especially until 12 weeks' gestation (pregnancy week 10), the expected pregnancy rate is about 35%.
The safety profile observed both LOTUS studies is as expected taking into account the well-established safety profile of dydrogesterone and the treatment population and indication.
Pharmacokinetics: Absorption: Following oral administration, dydrogesterone film-coated tablets, is rapidly absorbed. Maximum plasma concentrations of about 3.2 ng/ml and 57 ng/ml are attained between 0.5 and 1.5 hours after dosing for the parent drug dydrogesterone and its active metabolite 20α-dihydrodydrogesterone (DHD) respectively. The total drug exposures across time (AUC) are about 9.1 and 220 ng.hr/ml for Dydrogesterone and DHD respectively.
After a single dose, food delays the peak plasma concentration of dydrogesterone with approximately 1 hour, resulting in approximately 20% lower dydrogesterone peak plasma concentrations without affecting the extent of exposure to dydrogesterone and DHD.
The observed effect of concomitant food intake on the peak plasma concentration of dydrogesterone is considered not clinically relevant. Therefore, Duphaston film-coated tablets can be taken without regards to food.
Distribution: After oral administration of dydrogesterone the apparent volume of distribution is large, being approximately 22000 L. Dydrogesterone and DHD are more than 90% bound to plasma proteins.
Metabolism: Following oral administration, dydrogesterone is rapidly metabolized to DHD. The levels of the main active metabolite DHD peak at similar times as Dydrogesterone. The plasma levels of DHD are substantially higher as compared to the parent drug. The AUC and Cmax ratios of DHD to dydrogesterone are approximately 25 and 20, respectively. The mean terminal elimination half-lives of both dydrogesterone and DHD is about 15 hours. A common feature of all metabolites characterised is the retention of the 4,6 diene-3-one configuration of the parent compound and the absence of 17α-hydroxylation. This explains the lack of estrogenic and androgenic effects of dydrogesterone.
Elimination: After oral administration of labelled dydrogesterone, on average 63% of the dose is excreted into the urine. The apparent total body clearance of dydrogesterone from plasma is high at approximately 20 L/min. Within 72 hours excretion is complete. DHD is present in the urine predominantly as the glucuronic acid conjugate.
Dose and time dependencies: The single and multiple dose pharmacokinetics are linear in the oral dose range 2.5 to 10 mg. Comparison of the single and multiple dose kinetics shows that the pharmacokinetics of dydrogesterone and DHD are not changed as a result of repeated dosing. Steady state conditions are generally reached after 3 days of treatment.
Toxicology: Preclinical safety data: Non-clinical data obtained from conventional studies on single and repeated dose toxicity, genotoxicity and carcinogenic potential reveal no special hazard for humans.
Reproduction toxicity studies in rats have shown an increased incidence of prominent nipples (between day 11 and day 19 of age) and of hypospadias in the male offspring at high dosages not comparable to human exposure. The actual risk of hypospadias in humans cannot be determined in animal studies due to major species differences in metabolism between rats and humans (see Use in Pregnancy & Lactation).
Limited animal safety data suggest that dydrogesterone has prolongating effects on parturition, which is consistent with its progestogenic activity.
Progesterone deficiencies: Treatment of dysmenorrhoea.
Treatment of endometriosis.
Treatment of secondary amenorrhoea.
Treatment of irregular cycles.
Treatment of dysfunctional uterine bleeding.
Treatment of pre-menstrual syndrome.
Treatment of threatened abortion, associated with proven progesterone deficiency.
Treatment of habitual abortion, associated with proven progesterone deficiency.
Treatment of infertility due to luteal insufficiency.
Luteal support as part of an Assisted Reproductive Technology (ART) treatment.
Hormone replacement therapy: To counteract the effects of unopposed estrogen on the endometrium in hormone replacement therapy for women with disorders due to the natural or surgical induced menopause with an intact uterus.
Always take Duphaston exactly as the doctor has prescribed. If there are any questions, contact the doctor or pharmacist.
If the patient forgets to take the tablet(s), do not take a double dose to compensate for it. If the patient requires further information, ask the doctor or pharmacist for advice.
For hormone replacement therapy: In combination with continuous oestrogen therapy, take one tablet daily for 14 consecutive days of a 28 day cycle.
In combination with cyclical oestrogen therapy, take one tablet daily during the last 12 to 14 days of oestrogen therapy.
For doctors: If endometrial biopsies or ultrasound reveal inadequate progestational response, 20 mg dydrogesterone should be prescribed.
If the patient is not sure what type of oestrogen therapy, talk to the doctor before taking Duphaston.
Posology for specific indications: Dysmenorrhoea (painful menstruation): Take one tablet twice daily from day 5 to day 25 of the cycle.
Endometriosis (abnormal growth of uterine tissues outside the uterus): Take one tablet two or three times daily from day 5 to day 25 of the cycle or continuously (as prescribed by the doctor).
Dysfunctional bleeding (to stop bleeding): Take one tablet twice daily for five to seven days.
Dysfunctional bleeding (to prevent bleeding): Take one tablet twice daily from day 11 to day 25 of the cycle.
Amenorrhoea (cessation of menstruation): The doctor should prescribe an oestrogen along with Duphaston. Then take the oestrogen once daily from day 1 to day 25 of the cycle, together with one tablet of dydrogesterone twice daily from day 11 to day 25 of the cycle.
Premenstrual syndrome: Take one tablet twice daily from day 11 to day 25 of the cycle.
Irregular cycles: Take one tablet twice daily from day 11 to day 25 of the cycle.
Threatened abortion: Take four tablets at once, then one tablet every eight hours until symptoms abate.
Habitual abortion: Take one tablet twice daily until the twentieth week of pregnancy.
Infertility due to luteal (yellow body) insufficiency: Take one tablet daily from day 14 to 25 of the cycle. Continue the treatment for at least six consecutive cycles. In addition, it is advisable to continue treatment for the first few months of pregnancy as described under "Habitual abortion". If the patient is uncertain about how long to continue the treatment, talk to the doctor.
Luteal support as part of an Assisted Reproductive Technology (ART) treatment: Take one tablet three times daily (30 mg daily) starting at the day of oocyte retrieval and continuing for 10 weeks if pregnancy is confirmed.
Duphaston is not recommended for use in children below age 18 due to insufficient data on safety and efficacy.
Limited data are available with regard to overdose in humans. Dydrogesterone was well tolerated after oral dosing (maximum daily dose taken to date in humans 360 mg). There are no specific antidotes and treatment should be symptomatic. This information is also applicable for overdose in children.
Known hypersensitivity to the active substance or to any of the excipients.
Known or suspected progestogen dependent neoplasms (e.g. meningioma).
Undiagnosed vaginal bleeding.
Contraindications which are related to the use of estrogen when Duphaston is used in combination with estrogen (see also the contraindication in the product information of the estrogen preparation).
Treatment for luteal support as part of an Assisted Reproductive Technology (ART) treatment should be discontinued upon diagnosis of abortion or miscarriage.
Before initiating dydrogesterone treatment for abnormal bleeding the etiology for the bleeding should be clarified. Breakthrough bleeding and spotting may occur during the first months of treatment. If breakthrough bleeding or spotting appears after some time on therapy, or continues after treatment has been discontinued, the reason should be investigated, which may include endometrial biopsy to exclude endometrial malignancy.
Conditions which need supervision: If any of the following conditions are present, have occurred previously, and/or have been aggravated during pregnancy or previous hormone treatment, the patient should be closely supervised. It should be taken into account that these conditions may recur or be aggravated during treatment with dydrogesterone and ceasing the treatment should be considered: Porphyria; Depression; Abnormal liver function values by acute and chronic liver disease.
Other conditions: Patients with rare hereditary problems of galactose intolerance, Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.
The following warnings and precautions apply when using dydrogesterone in combination with estrogens for hormone replacement therapy (HRT): See also precautions in the product information of the estrogen preparation.
For the treatment of postmenopausal symptoms, HRT should only be initiated for symptoms that adversely affect quality of life. In all cases, a careful appraisal of the risks and benefits should be undertaken at least annually and HRT should only be continued as long as the benefit outweighs the risk.
Evidence regarding the risks associated with HRT in the treatment of premature menopause is limited. Due to the low level of absolute risk in younger women, however, the balance of benefits and risks for these women may be more favorable than in older women.
Medical examination/follow-up: Before initiating or reinstituting HRT, a complete personal and family medical history should be taken. Physical (including pelvic and breast) examination should be guided by this and by the contraindications and warnings for use. During treatment, periodic check-ups are recommended of a frequency and nature adapted to the individual woman. Women should be advised what changes in their breasts should be reported to their doctor or nurse (see 'Breast cancer' as follows).
Investigations, including appropriate imaging tools, e.g., mammography, should be carried out in accordance with currently accepted screening practices, modified to the clinical needs of the individual.
Endometrial hyperplasia and carcinoma: In women with an intact uterus the risk of endometrial hyperplasia and carcinoma is increased when estrogens are administered alone for prolonged periods.
The addition of a progestogen such as dydrogesterone cyclically for at least 12 days per month/28 day cycle or continuous combined estrogen-progestogen therapy in nonhysterectomized women can prevent the excess risk associated with estrogen-only HRT.
Breast cancer: The overall evidence suggests an increased risk of breast cancer in women taking combined estrogen-progestogen and possibly also estrogen-only HRT, that is dependent on the duration of taking HRT.
Combined estrogen-progestogen therapy: The randomized placebo-controlled trial, Women's Health Initiative study (WHI), and a meta-analysis of prospective epidemiological studies are consistent in finding an increased risk of breast cancer in women taking combined estrogen-progestogen for HRT that becomes apparent after about 3 (1-4) years. Results from a large meta-analysis showed that after stopping treatment, the excess risk will decrease with time and the time needed to return to baseline depends on the duration of prior HRT use. When HRT was taken for more than 5 years, the risk may persist for 10 years or more. HRT, especially estrogen-progestogen combined treatment, increases the density of mammographic images which may adversely affect the radiological detection of breast cancer.
Ovarian cancer: Ovarian cancer is much rarer than breast cancer. Epidemiological evidence from a large meta-analysis suggests a slightly increased risk in women taking oestrogen-only or combined oestrogen-progestogen HRT, which becomes apparent within 5 years of use and diminishes over time after stopping. Some other studies including the WHI trial suggest that use of combined HRTs may be associated a similar, or slightly smaller, risk.
Venous thromboembolism: HRT is associated with a 1.3-3 fold risk of developing venous thromboembolism (VTE), i.e. deep vein thrombosis or pulmonary embolism. The occurrence of such an event is more likely in the first year of HRT than later.
Patients with known thrombophilic states have an increased risk of VTE and HRT may add to this risk. HRT is therefore contraindicated in these patients.
Generally recognized risk factors for VTE include, use of estrogens, older age, major surgery, prolonged immobilization, obesity (BMI > 30 kg/m2), pregnancy/postpartum period, systemic lupus erythematosus (SLE), and cancer. There is no consensus about the possible role of varicose veins in VTE.
As in all postoperative patients, prophylactic measures need be considered to prevent VTE following surgery. If prolonged immobilization is to follow elective surgery temporarily stopping HRT 4 to 6 weeks earlier is recommended. Treatment should not be restarted until the woman is completely mobilized.
In women with no personal history of VTE but with a first degree relative with a history of thrombosis at young age, screening may be offered after careful counseling regarding its limitations (only a proportion of thrombophilic defects are identified by screening).
If a thrombophilic defect is identified which segregates with thrombosis in family members or if the defect is 'severe' (e.g., antithrombin, protein S, or protein C deficiencies or a combination of defects) HRT is contraindicated.
Women already on chronic anticoagulant treatment require careful consideration of the benefit risk of use of HRT.
If VTE develops after initiating therapy, the drug should be discontinued. Patients should be told to contact their doctors immediately when they are aware of a potential thromboembolic symptom (e.g., painful swelling of a leg, sudden pain in the chest, dyspnea).
Coronary artery disease (CAD): There is no evidence from randomized controlled trials of protection against myocardial infarction in women with or without existing CAD who received combined estrogen-progestogen or estrogen-only HRT.
Combined estrogen-progestogen therapy: The relative risk of CAD during use of combined estrogen-progestogen HRT is slightly increased. As the baseline absolute risk of CAD is strongly dependent on age, the number of extra cases of CAD due to estrogen-progestogen use is very low in healthy women close to menopause, but will rise with more advanced age.
Ischemic stroke: Combined estrogen-progestogen and estrogen-only therapy are associated with an up to 1.5-fold increase in risk of ischemic stroke. The relative risk does not change with age or time since menopause. However, as the baseline risk of stroke is strongly age-dependent, the overall risk of stroke in women who use HRT will increase with age.
Effects on ability to drive and use machines: Dydrogesterone has minor influence on the ability to drive and use machines.
Infrequently, dydrogesterone may cause mild somnolence and/or dizziness, especially within the first few hours after intake. Therefore, care should be taken when driving or using machines.
Pregnancy: It is estimated that more than 10 million pregnancies have been exposed to dydrogesterone. So far there were no indications of a harmful effect of dydrogesterone use during pregnancy.
Some progestogens have been reported in the literature to be associated with an increased risk of hypospadias. However due to confounding factors during pregnancy, no definitive conclusion can be drawn regarding the contribution of progestogens to hypospadias. Clinical studies, where a limited number of women were treated with dydrogesterone early in pregnancy, have not shown any increase in risk. No other epidemiological data are hitherto available.
Effects in non-clinical embryo-fetal and post-natal development studies were in line with the pharmacological profile. Untoward effects occurred only at exposures which exceeded the maximum human exposure considerably, indicating little relevance to clinical use (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Dydrogesterone can be used during pregnancy if clearly indicated.
Breastfeeding: No data exist on excretion of dydrogesterone in mother's milk. Experience with other progestogens indicates that progestogens and the metabolites pass to mother's milk in small quantities. Whether there is a risk to the child is not known. Therefore, dydrogesterone should not be used during the lactation period.
Fertility: There is no evidence that dydrogesterone decreases fertility at therapeutic dose.
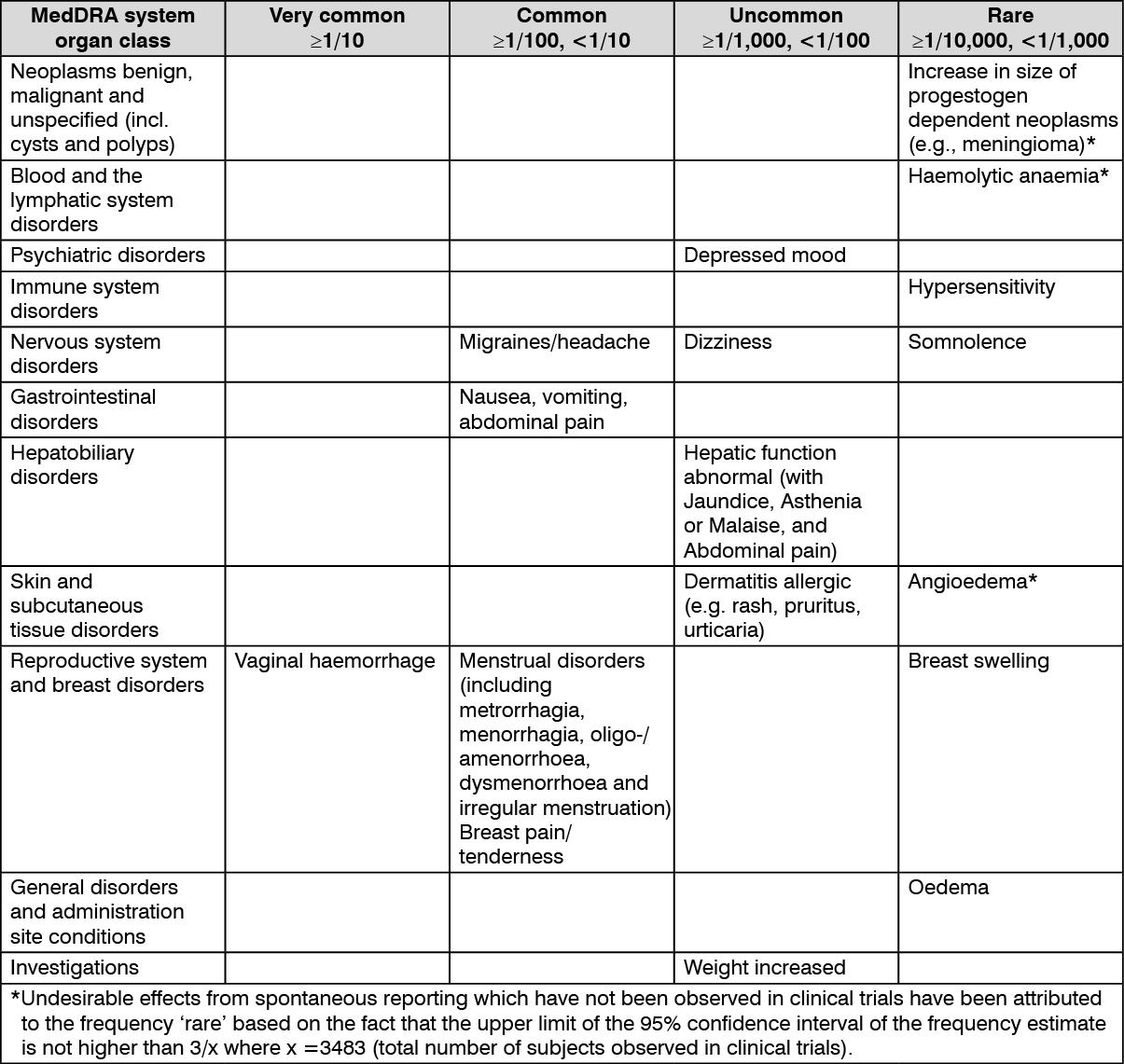
The most commonly reported adverse drug reactions of patients treated with dydrogesterone in clinical trials of indications without estrogen treatment are vaginal haemorrhage, migraines/headache, nausea, vomiting, abdominal pain, menstrual disorders and breast pain/tenderness.
The following undesirable effects have been observed with the frequencies indicated as follows during clinical trials using dydrogesterone (n=3483) in indications without estrogen treatment, in two company sponsored interventional clinical trials in luteal support as part of an ART treatment using dydrogesterone (n=1036) and from spontaneous reporting. Frequencies are based on the most conservative approach. (See table.)
 Click on icon to see table/diagram/image
Undesirable effects in adolescent population:
Click on icon to see table/diagram/image
Undesirable effects in adolescent population: Based on spontaneous reports and limited clinical trial data, the adverse reaction profile in adolescents is expected to be similar to that seen in adults.
Undesirable effects that are associated with an estrogen-progestogen treatment (see also Precautions and the product information of the estrogen preparation): Breast cancer, endometrial hyperplasia, endometrial carcinoma, ovarian cancer.
Venous thromboembolism.
Myocardial infarction, coronary artery disease, ischemic stroke.
In vitro data show that the major metabolic pathway generating the main pharmacologically active metabolite 20α-dihydrodydrogesterone (DHD) is catalyzed by aldo-keto reductase 1C (AKR 1C) in human cytosol. Next to the cytosolic metabolism there are metabolic transformations by cytochrome P450 iso-enzymes (CYPs), nearly exclusively via CYP3A4, resulting in several minor metabolites. The main active metabolite DHD is substrate for metabolic transformation by CYP3A4.
Therefore, the metabolism of dydrogesterone and DHD may be increased by concomitant use of substances known to induce CYP enzymes such as anticonvulsants (e.g., phenobarbital, phenytoin, carbamazepine), anti-infectives (e.g., rifampicin, rifabutin, nevirapine, efavirenz) and herbal preparations containing e.g. St John's Wort (Hypericum perforatum), sage, or gingko biloba.
Ritonavir and nelfinavir, although known as strong cytochrome enzyme inhibitors, by contrast exhibit enzyme-inducing properties when used concomitantly with steroid hormones.
Clinically, an increased metabolism of dydrogesterone may lead to a decreased effect.
In vitro studies have shown that dydrogesterone and DHD do not inhibit or induce CYP drug metabolizing enzymes at clinically relevant concentrations.
Incompatibilities: Not applicable.
Special precautions for disposal and other handling: Any unused product or waste material should be disposed of in accordance with local requirements.
Special precautions for storage: This medicinal product does not require any special storage condition.
Do not store above 30°C.
Keep the blister in the outer carton, in order to protect from moisture.
Shelf life: 5 years.
G03DB01 - dydrogesterone ; Belongs to the class of pregnadien derivative progestogens used in progestogenic hormone preparations.
Duphaston FC tab 10 mg
20's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
