Travoprost, timolol maleate.
One mL of solution contains 40 micrograms of travoprost and 5 mg of timolol (6.8 mg timolol maleate).
Excipients/Inactive Ingredients: Boric acid, mannitol, polyoxyethylene hydrogenated castor oil 40 (HCO-40), polyquaternium-1 (POLYQUAD), propylene glycol, sodium chloride, sodium hydroxide and/or hydrochloric acid (for pH adjustment), and purified water.
Pharmacotherapeutic group: Ophthalmologicals, antiglaucoma preparations and miotics. ATC code: S01ED51.
Pharmacology: Mechanism of action (MOA): DuoTrav contains two active ingredients: travoprost and timolol maleate. These two agents reduce IOP by complementary mechanisms of action with a combined effect greater than that of either compound administered alone (synergistic effect).
Travoprost, a prostaglandin F2alpha analogue, is a full agonist which is highly selective and has a high affinity for the prostaglandin FP receptor, and reduces IOP by increasing the outflow of aqueous humor via trabecular meshwork and uveoscleral pathways. Reduction of IOP in humans starts within approximately 2 hours of administration and maximum effect is achieved within 12 hours. Significant IOP reduction can be maintained for periods exceeding 24 hours following a single dose.
Timolol is a non-selective beta-adrenergic blocking agent that has no intrinsic sympathomimetic, direct myocardial depressant or membrane-stabilizing activity. Its predominant ocular mechanism of action is to reduce aqueous humor formation and a slight increase in outflow activity.
Pharmacodynamics: In addition to reducing IOP, travoprost has been shown to increase optic nerve head blood flow based on data in rabbits following 7 days of topical ocular administration (1.4 micrograms, once daily (QD)).
Clinical studies: In a 12-month, controlled clinical study in patients with open-angle glaucoma or ocular hypertension and a mean baseline IOP range of 25 to 27 mmHg, the mean IOP-lowering of DuoTrav dosed QD in the morning was 8 to 10 mmHg. The non-inferiority of DuoTrav as compared with latanoprost 0.005% plus timolol 0.5% in mean IOP reduction was demonstrated across all time points at all visits.
In a 3-month, controlled clinical study in patients with open-angle glaucoma or ocular hypertension and a mean baseline IOP range of 27 to 30 mmHg, the mean IOP-lowering effect of DuoTrav dosed QD in the morning was up to 2 mmHg greater than that of travoprost 0.004% dosed QD in the evening and 2 to 3 mmHg greater than that of timolol 0.5% dosed b.i.d. A statistically significant superior reduction in mean morning IOP (8 AM - 24 hours after the previous DuoTrav dose) was observed compared with travoprost 0.004% at all visits throughout the study.
In two 3-month, controlled clinical studies in patients with open-angle glaucoma or ocular hypertension and a mean baseline IOP range of 23 to 26 mmHg, the mean IOP-lowering effect of DuoTrav dosed QD in the morning was 7 to 9 mmHg. Mean IOP reductions were non-inferior, although numerically lower, compared with those achieved by concomitant therapy with travoprost 0.004% dosed QD in the evening and timolol 0.5% dosed QD in the morning.
In a 6-week, controlled clinical study in patients with open-angle glaucoma or ocular hypertension and a mean baseline IOP range of 24 to 26 mmHg, the mean IOP-lowering effect of DuoTrav (polyquaternium
1-preserved) dosed QD in the morning was 8 mmHg and equivalent to that of DuoTrav (benzalkonium chloride-preserved).
Inclusion criteria were similar across the previously mentioned clinical studies, with the exception of the IOP entry criteria and response to previous IOP-lowering therapy. The clinical development of DuoTrav included both treatment-naïve patients and patients on therapy. Insufficient responsiveness to monotherapy was not an inclusion criterion. DuoTrav was well tolerated with no serious adverse events observed.
Additional randomized, double- or observer-masked, active-controlled studies have been performed in which over 500 subjects with open-angle glaucoma or ocular hypertension were treated with Travoprost 0.004%/Timolol 0.5%.
Many of these studies measured the IOP-lowering effects Travoprost 0.004%/Timolol 0.5% after a wash-out period and these demonstrated an IOP-lowering effect from baseline that is consistent with that shown in the pivotal studies described previously.
Pharmacokinetics: Absorption: Travoprost and timolol are absorbed through the cornea. Travoprost is an isopropyl ester prodrug which undergoes rapid hydrolysis in the cornea to produce the active free acid. Following QD administration of DuoTrav (polyquaternium-1-preserved) to healthy subjects for 5 days, travoprost free acid plasma concentrations were below the 0.010 ng/mL assay quantitation limit in the majority of samples. Quantifiable free acid concentrations were observable in some cases within 1 hour post-dose, ranging from 0.010 to 0.030 ng/mL. The mean timolol steady-state Cmax was 1.34 ng/mL and Tmax was approximately 0.69 hours after QD administration of DuoTrav. Timolol has a plasma elimination half-life of about 4 hours.
Distribution: Travoprost free acid can be measured in aqueous humor for several hours in animals and in human plasma up to 1 hour post-dose. Timolol can be measured in human aqueous humor after topical ocular administration of timolol and in plasma for up to 12 hours following topical ocular administration of DuoTrav.
Biotransformation/metabolism: Metabolism is the primary clearance mechanism for both travoprost and its free acid. The systemic metabolic pathways for travoprost free acid parallel those of endogenous prostaglandin F2alpha, which are characterized by reduction of the 13 to 14 double bond, oxidation of the 15-hydroxyl to form a ketone, and beta-oxidative cleavages of the carboxylic acid side chain.
Timolol is primarily metabolized by CYP2D6 via two pathways. One route yields an ethanolamine side chain on the thiadiazole ring and the other generates an ethanolic side chain on the morpholine nitrogen and a second similar side chain with a carbonyl function adjacent to the nitrogen. No timolol metabolism occurs within the eye.
Elimination: Both travoprost free acid and timolol, along with their respective metabolites, are primarily excreted in urine. Less than 2% of an ocular dose of travoprost was recovered in urine as travoprost free acid. Approximately 20% of a timolol dose was found in urine as parent drug with the remainder excreted as metabolites.
Due to the very low concentrations and rapid disappearance of travoprost free acid from plasma, elimination half-life could not be determined. Timolol has a plasma elimination half-life of about 4 hours.
Linearity/non-linearity: Both travoprost and timolol exhibit linear pharmacokinetics following topical administration, either alone or in combination.
Pediatric patients (below 18 years): The pharmacokinetics of DuoTrav in pediatric patients has not been studied.
Pharmacogenomics: Higher plasma concentrations were detected in CYP2D6 poor metabolizers (PMs) compared with extensive metabolizers (EMs). Similar results have been obtained after the administration of ophthalmic timolol.
Toxicology: Non-clinical safety data: Non-clinical data for travoprost and timolol reveal no special hazard for humans based on conventional studies of single dose toxicity, repeated-dose toxicity, genotoxicity, carcinogenicity and topical ocular irritation studies. Ocular irritation studies were also conducted with travoprost plus timolol, and no adverse effects were observed with the exception of widened palpebral fissure and increased iris pigmentation in monkeys, which is consistent with the topical ocular administration of prostaglandins in humans. For details on reproductive studies, see Use in Pregnancy & Lactation.
Fertility studies in rats dosed with travoprost subcutaneously resulted in significant reductions in the number of corpora lutea, viable fetuses, and an increased early post-implantation loss as well as resorption rate at 10 micrograms/kg/day (34 times the MROHD based on BSA). The no effect level was set at 3 micrograms/kg/day (10 times the MROHD based on BSA). In contrast, fertility studies with timolol in rats showed no effects at oral doses up to 150 mg/kg/day (4,050 times the MROHD based on BSA).
Decrease of intraocular pressure (IOP) in adult patients with open-angle glaucoma or ocular hypertension who are insufficiently responsive to topical beta-blockers or prostaglandin analogues.
Dosage regimen: General target population: Adults: The recommended dosage of DuoTrav is one drop in the conjunctival sac of the affected eye(s) once daily in the morning or evening. It should be administered at the same time each day. The dosage of DuoTrav should not exceed one drop in the affected eye(s) once daily since it has been shown that more frequent administration of prostaglandin analogues may decrease the IOP-lowering effect.
If a dose is missed, treatment should continue with the next dose as planned. If more than one topical ophthalmic drug is being used, the drugs should be administered at least 5 minutes apart.
When substituting another ophthalmic antiglaucoma medicinal product with DuoTrav Eye Drops, Solution, the other medicinal product should be discontinued and DuoTrav Eye Drops, Solution should be started the following day.
Special populations: Hepatic and renal impairment: No studies have been conducted with DuoTrav or with timolol 5 mg/mL eye drops in patients with renal or hepatic impairment.
Travoprost alone has been studied in patients with mild to severe hepatic impairment and in patients with mild to severe renal impairment (creatinine clearance as low as 14 mL/min). No dose adjustment was necessary in these patients. Patients with hepatic or renal impairment are unlikely to a require dose adjustment with DuoTrav.
Pediatric patients (below 18 years): The use of DuoTrav in pediatric patients is currently not recommended. The safety and efficacy of the use of DuoTrav in children and adolescents below the age of 18 years have not been established. No data are available.
Geriatric patients (65 years of age and above): No overall differences in safety or effectiveness have been observed between elderly and other adult patients.
Method of administration: For ocular use only.
To avoid contamination, the dropper tip should not touch any surface. The dropper tip should also not come into contact with the eye as this may cause injury to the eye. When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase in local activity.
No specific reactions are to be expected with an ocular overdose of the product.
In case of accidental ingestion, symptoms of overdose from systemic beta-blockade may include bradycardia, hypotension, cardiac failure and bronchospasm.
Treatment of an accidental ingestion should be symptomatic and supportive.
Hypersensitivity to the active substances, or to any of the excipients.
Reactive airway disease including bronchial asthma or a history of bronchial asthma, severe chronic obstructive pulmonary disease.
Sinus bradycardia, sick sinus syndrome (including sino-atrial block), second or third degree atrioventricular block, overt cardiac failure, or cardiogenic shock.
General: Like other topically applied ophthalmic agents, travoprost and timolol are absorbed systemically. Due to the beta-adrenergic blocking component in ophthalmic timolol, the same types of cardiovascular, pulmonary and other adverse reactions seen with systemic beta-adrenergic blocking agents may occur.
Cardiac disorders: In patients with cardiovascular diseases (e.g. coronary heart disease, Prinzmetal's angina and cardiac failure) and hypotension, therapy with beta-blockers should be critically assessed and the therapy with other active substances should be considered. Patients with cardiovascular diseases should be watched for signs of deterioration of these diseases and for adverse reactions.
Vascular disorders: Patients with severe peripheral circulatory disturbance/disorders (i.e. severe forms of Raynaud's disease or Raynaud's syndrome) should be treated with caution.
Respiratory disorders: Respiratory reactions, including death due to bronchospasm in patients with asthma have been reported following administration of some ophthalmic beta-blockers.
Hypoglycemia/diabetes: Beta-blockers should be administered with caution in patients subject to spontaneous hypoglycemia or to patients with labile diabetes, as beta-blockers may mask the signs and symptoms of acute hypoglycemia.
Hyperthyroidism: Beta-blockers may mask the signs of hyperthyroidism.
Muscle weakness: Beta-adrenergic blocking agents have been reported to potentiate muscle weakness consistent with certain myasthenic symptoms (e.g. diplopia, ptosis and generalized weakness).
Anaphylactic reactions: While taking beta-blockers, patients with history of atopy or a history of severe anaphylactic reaction to a variety of allergens may be more reactive to repeated challenge with such allergens and unresponsive to the usual dose of adrenaline (epinephrine) used to treat anaphylactic reactions.
Ocular effects: Travoprost may gradually change the eye color by increasing the number of melanosomes (pigment granules) in melanocytes. Before treatment is instituted, patients must be informed of the possibility of a permanent change in eye color. The change in iris color occurs slowly and may not be noticeable for months to years.
Periorbital and/or eyelid skin darkening has been reported in association with the use of travoprost. Periorbital and lid changes, including deepening of the eyelid sulcus, have been observed with prostaglandin analogues.
Travoprost may gradually change eyelashes in the treated eye(s); these changes include increased length, thickness, pigmentation, and/or number of lashes.
Macular edema has been reported during treatment with prostaglandin F2a analogues. Travoprost should be used with caution in aphakic patients, pseudophakic patients with torn posterior lens capsule or anterior chamber lenses, or in patients with known risk factors for macular edema.
DuoTrav should be used with caution in patients with active intraocular inflammation, as well as patients with predisposing risk factors for uveitis.
Choroidal detachment: Choroidal detachment has been reported with administration of aqueous suppressant therapy (e.g. timolol, acetazolamide) after filtration procedures.
Surgical anesthesia: Beta-blocking ophthalmological preparations may block systemic beta-agonist effects e.g. of adrenaline. The anesthesiologist should be informed when the patient is receiving timolol.
Other beta-blocking agents: The effect on intra-ocular pressure or the known effects of systemic beta-blockade may be exaggerated when timolol is given to the patients already receiving a systemic beta-blocking agent. The response of these patients should be closely observed. The use of two topical beta-adrenergic blocking agents is not recommended (see Interactions).
Effects on ability to drive and use machines: As with any eye drop, temporary blurred vision or other visual disturbances may affect the ability to drive or use machines. If blurred vision occurs at instillation, the patient must wait until the vision clears before driving or using machines.
Pregnancy: Risk summary: There is limited amount of data from the use of DuoTrav or the individual components in pregnant women.
Studies in rats and mice with subcutaneous (s.c.) administration of travoprost during organogenesis have shown reproductive toxicity at the dose of 34 times and 1.7 times, respectively, the maximum recommended ocular human dose (MROHD) based on body surface area (BSA). Reproduction studies in mice, rats and rabbits with orally administered timolol showed no malformations at doses up to 675 times the MROHD based on BSA (see Animal data as follows).
Epidemiological studies have not revealed malformative effects but show a risk for intrauterine growth retardation when beta-blockers are administered by the oral route. In addition, signs and symptoms of beta-blockade (e.g. bradycardia, hypotension, respiratory distress and hypoglycemia) have been observed in the neonate when systemic beta-blockers have been administered to the mother until delivery.
DuoTrav should not be used during pregnancy unless clearly necessary. However, if DuoTrav is administered during pregnancy up to the time of delivery, the neonate should be carefully monitored during the first days of life.
Animal data: Travoprost: An embryo-fetal study was conducted in pregnant mice administered travoprost once daily by subcutaneous injection during the period of organogenesis. At 1 microgram/kg/day (1.7 times the MROHD, based on BSA), travoprost caused post-implantation loss and decreased fetal weight. The no-observed-effect-level (NOEL) for embryofetal toxicity was 0.3 micrograms/kg/day (0.5 times the MROHD, based on BSA). The maternal NOEL was 1 microgram/kg/day.
An embryo-fetal study was conducted in pregnant rats administered travoprost once daily by s.c. injection during the period of organogenesis. At 10 micrograms/kg/day (34 times the MROHD, based on BSA), travoprost was teratogenic in rats, as evidenced by an increase in the incidence of skeletal malformations as well as external and visceral malformations, including fused sternebrae, domed head and hydrocephaly. Travoprost caused post-implantation loss at 10 micrograms/kg/day. The NOEL for post-implantation loss was 3 micrograms/kg/day (10 times the MROHD based on BSA).
Pre- and postnatal development studies were conducted in rats administered with travoprost once daily by s.c. injection during organogenesis and lactation. At doses of ≥0.12 micrograms/kg/day (0.4 times the MROHD, based on BSA), adverse pregnancy outcomes (embryofetal lethality, abortion, early delivery), low birth weight and developmental delays were observed for F1 offspring. The NOEL for adverse pregnancy outcomes, low birth weight and developmental delay was 0.1 micrograms/kg/day (0.3 times the MROHD, based on BSA). The NOEL for F2 offspring development was 0.36 micrograms/kg/day (1.2 times the MROHD, based on BSA).
Timolol: Teratogenicity studies with timolol in mice, rats, and rabbits at oral doses up to 50 mg/kg/day (675 times the MROHD based on BSA) demonstrated no evidence of fetal malformations. Although delayed fetal ossification was observed at this dose in rats, there were no adverse effects on postnatal development of offspring. Doses of 1,000 mg/kg/day (13,500 times the MROHD based on BSA) were maternal toxic in mice and resulted in an increased number of fetal resorptions. Increased fetal resorptions were also seen in rabbits at 100 mg/kg/day or 5,400 times the MROHD based on BSA, and without apparent maternal toxicity.
Lactation: Risk summary: There is a limited amount of data from the use of DuoTrav Eye Drops, Solution in breast-feeding women.
Timolol is transferred into human breast milk following ocular topical administration. Oral beta-blockers have the potential to cause serious adverse reactions in the breast-fed infant. However, in the case of ocular administration at therapeutic doses, the amounts of timolol present in breast milk are not likely to produce clinical symptoms of beta-blockade in the infant.
It is unknown whether travoprost is transferred into human breast milk after ocular administration. An animal study has shown transfer of travoprost and/or metabolites into milk following subcutaneous administration (see Animal data as follows).
The developmental and health benefits of breast-feeding should be considered along with the mother's clinical need for DuoTrav and any potential adverse effects on the breast-fed child from DuoTrav.
Animal data: A study in lactating rats demonstrated that radiolabeled travoprost and/or its metabolites were excreted in milk following subcutaneous administration with highest concentrations of travoprost and/or metabolites observed 6 hours post-dose with a milk to plasma ratio of 11.
Females and males of reproductive potential: Infertility: There are no data on the effects of DuoTrav on human fertility. Fertility studies in rats showed no effect of travoprost or timolol at doses up to 34 times and 4,050 times the MROHD, respectively, based on BSA (see Pharmacology: Toxicology: Non-clinical safety data under Actions).
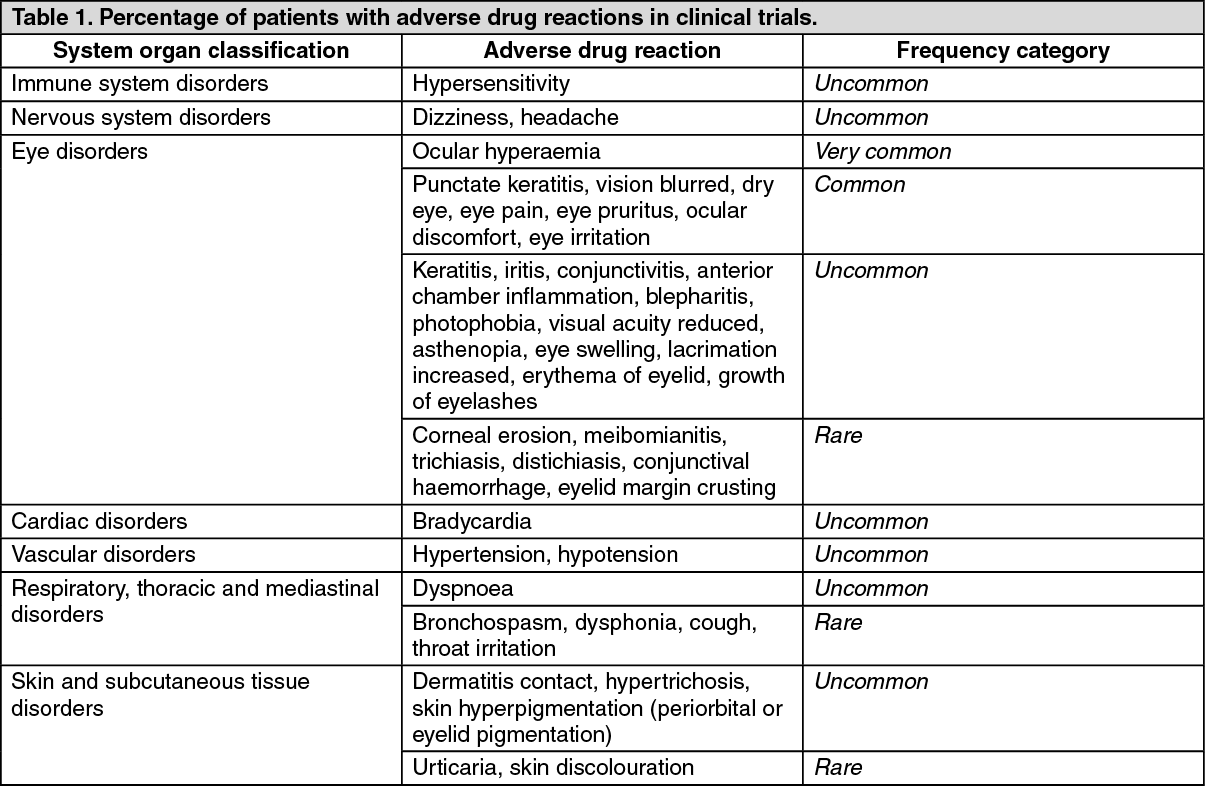
Tabulated summary of adverse drug reactions from clinical trials: Adverse drug reactions from clinical trials (Table 1) are listed by MedDRA system organ class. Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. In addition, the corresponding frequency category for each adverse drug reaction is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). (See Table 1.)
 Click on icon to see table/diagram/image
Adverse drug reactions from spontaneous reports and literature cases (frequency not known):
Click on icon to see table/diagram/image
Adverse drug reactions from spontaneous reports and literature cases (frequency not known): The following adverse drug reactions have been derived from post-marketing experience with DuoTrav via spontaneous case reports and literature cases. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency which is therefore categorized as not known. Adverse drug reactions are listed according to system organ classes in MedDRA. Within each system organ class, ADRs are presented in order of decreasing seriousness. (See Table 2.)
Click on icon to see table/diagram/image
Additional adverse reactions previously reported with the individual components of DuoTrav: See Product Information for Timolol 2.5 mg/mL and 5 mg/mL Eye Drops, Solution and Travoprost 30 micrograms/mL and 40 micrograms/mL Eye Drops, Solution.
The following interactions are expected with DuoTrav due to potential drug interactions with the mono-components: Potentiated systemic beta-blockade (e.g., decreased heart rate, depression) has been reported during combined treatment with CYP2D6 inhibitors (e.g. quinidine, fluoxetine, paroxetine) and timolol.
There is a potential for additive effects resulting in hypotension and/or marked bradycardia when an ophthalmic beta-blocker solution is administered concomitantly with oral calcium channel blockers, beta-adrenergic blocking agents, antiarrhythmics (including amiodarone), digitalis glycosides, parasympathomimetics.
Beta-blockers can decrease the response to adrenaline used to treat anaphylactic reactions. Special caution should be exercised in patients with a history of atopy or anaphylaxis (see Precautions).
Mydriasis resulting from concomitant use of ophthalmic beta-blockers and adrenaline (epinephrine) has been reported occasionally.
Incompatibilities: Not applicable.
Special precautions for disposal: Any unused product or waste material should be disposed of in accordance with local requirements.
S01ED51 - timolol, combinations ; Belongs to the class of beta blocking agents. Used in the treatment of glaucoma.
DuoTrav eye drops
2.5 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image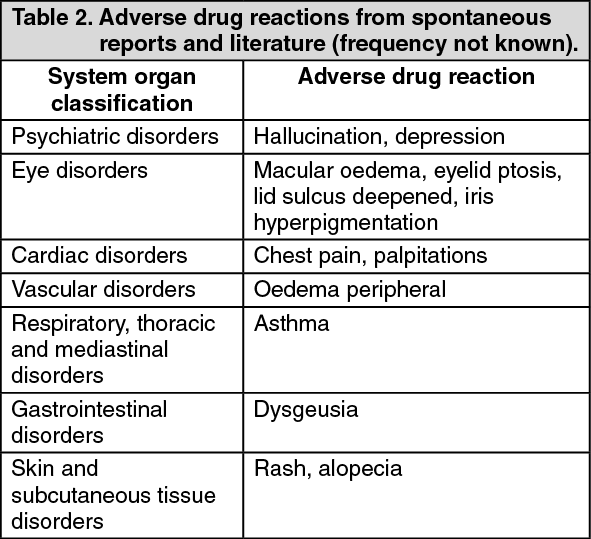 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
