


 Sign Out
Sign Out

Doxorubicin exhibits unique pharmacokinetic properties and must not be used interchangeably with other formulations of doxorubicin hydrochloride.
Posology: Breast cancer/Ovarian cancer: Doxorubicin is administered intravenously at a dose of 50 mg/m2 once every 4 weeks for as long as the disease does not progress and the patient continues to tolerate treatment.
Multiple myeloma: Doxorubicin is administered at 30 mg/m2 on day 4 of the bortezomib 3 week regimen as a 1 hour infusion administered immediately after the bortezomib infusion. The bortezomib regimen consists of 1.3 mg/m2 on days 1, 4, 8, and 11 every 3 weeks. The dose should be repeated as long as patients respond satisfactorily and tolerate treatment.
AIDS-KS patients: Doxorubicin should be administered intravenously at 20 mg/m2 every two-to-three weeks. Intervals shorter than 10 days should be avoided as drug accumulation and increased toxicity cannot be ruled out. Patients should be treated for two-to-three months to achieve a therapeutic response. Treatment should be continued as needed to maintain a therapeutic response.
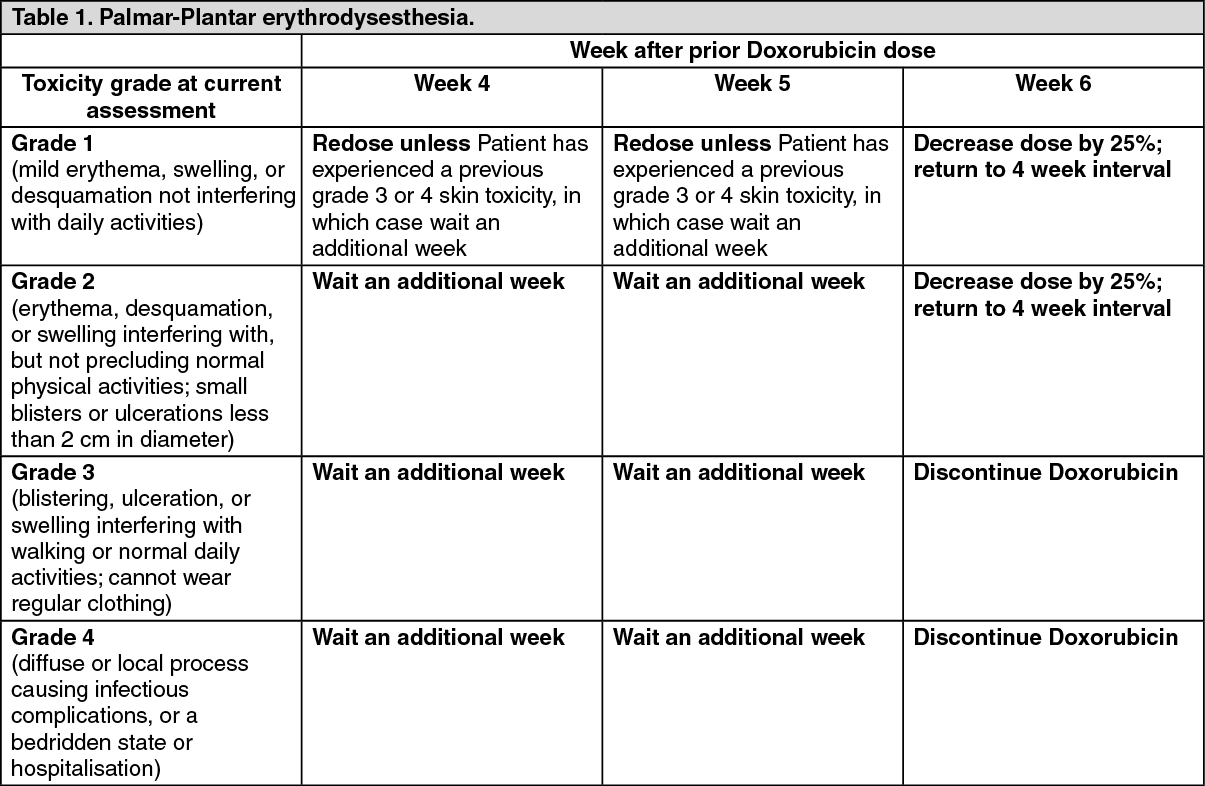
Guidelines for Doxorubicin dose modification: To manage adverse events such as palmar-plantar erythrodysesthesia (PPE), stomatitis or haematological toxicity, the dose may be reduced or delayed. Guidelines for Doxorubicin dose modification secondary to these adverse effects are provided in the tables as follows. The toxicity grading in these tables is based on the National Cancer Institute Common Toxicity Criteria (NCI-CTC).
The tables for PPE (Table 1) and stomatitis (Table 2) provide the schedule followed for dose modification in clinical trials in the treatment of breast or ovarian cancer (modification of the recommended 4 week treatment cycle): if these toxicities occur in patients with AIDS-related KS, the recommended 2 to 3 week treatment cycle can be modified in a similar manner.
The table for haematological toxicity (Table 3) provides the schedule followed for dose modification in clinical trial in the treatment of patients with breast or ovarian cancer only. Dose modification in patients with AIDS-KS is addressed in Adverse Reactions. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image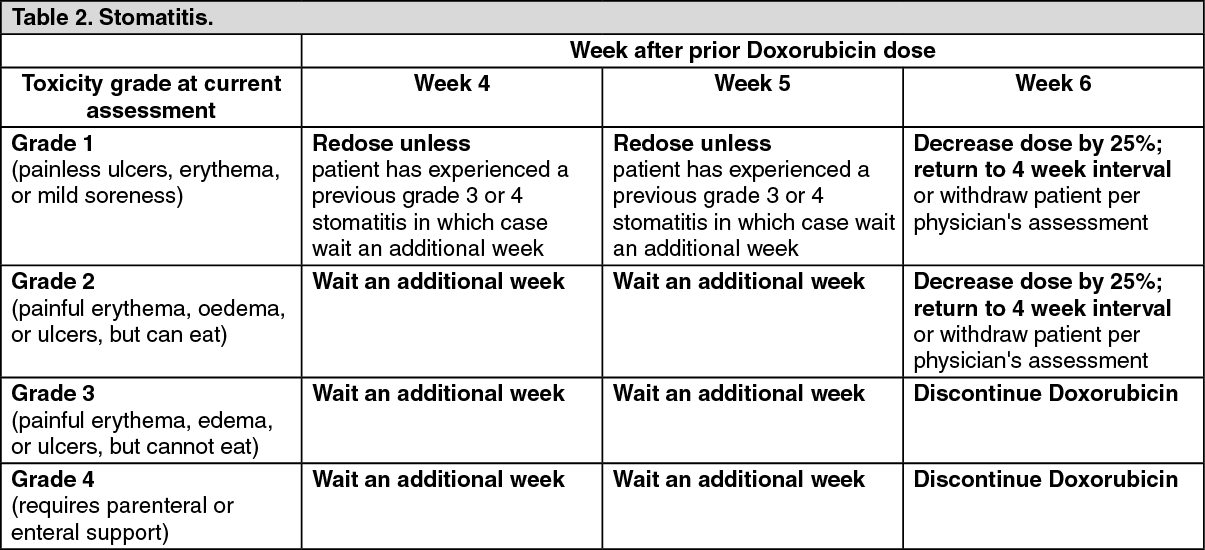 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
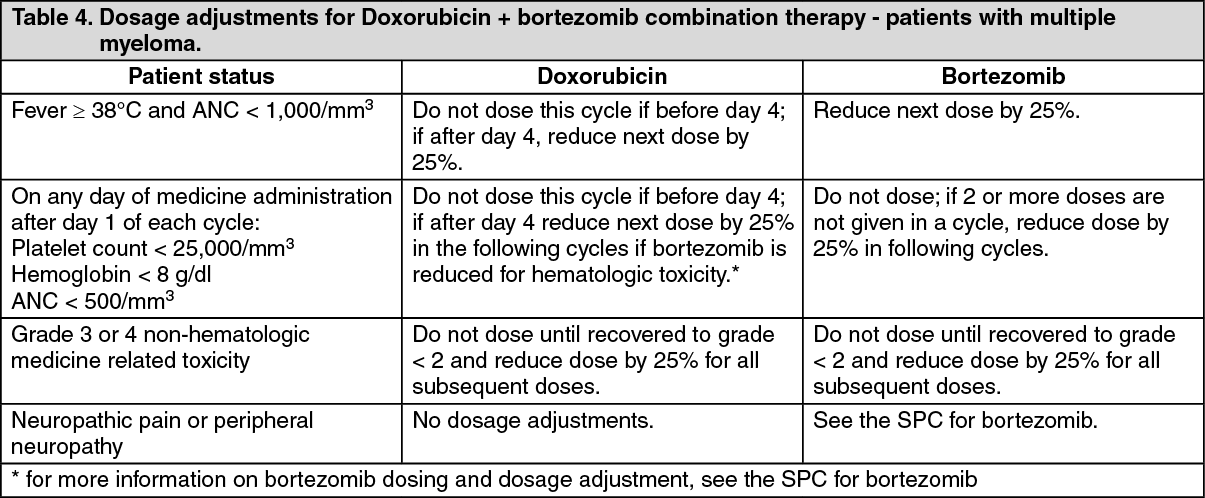
Click on icon to see table/diagram/imageFor multiple myeloma patients treated with Doxorubicin in combination with bortezomib who experience PPE or stomatitis, the Doxorubicin dose should be modified as described previously in Table 1 and 2 respectively. For more detailed information on bortezomib dosing and dosage adjustments, see the prescribing information for bortezomib. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial Populations: Pediatrics (17 years of age and younger): Limited Phase I safety data indicate that doses up to 60 mg/m2 every 4 weeks are well tolerated in pediatric patients; however, effectiveness in patients under 18 years of age has not been established.
Elderly (65 years of age and older): Population based analysis demonstrates that age across the range tested (21-75 years) does not significantly alter the pharmacokinetics of doxorubicin.
Patients with impaired renal function: As doxorubicin is metabolised by the liver and excreted in the bile, dose modification should not be required with Doxorubicin. Population-based analysis confirms that changes in renal function over the range tested (estimated creatinine clearance 30-156 mL/min) do not alter the pharmacokinetics of doxorubicin. No pharmacokinetic data are available in patients with creatinine clearance of less than 30 ml/min.
Hepatic impairment: Doxorubicin pharmacokinetics determined in a small number of patients with elevated total bilirubin levels do not differ from patients with normal total bilirubin; however, until further experience is gained, the doxorubicin dosage in patients with impaired hepatic function should be reduced based on the experience from the breast and ovarian clinical trial program as follows: At initiation of therapy, if the bilirubin is between 1.2 - 3.0 mg/dl, the first dose is reduced by 25 %. If the bilirubin is > 3.0 mg/dL, the first dose is reduced by 50 %. If the patient tolerates the first dose without an increase in serum bilirubin or liver enzymes, the dose for cycle 2 can be increased to the next dose level, i.e., if reduced by 25 % for the first dose, increase to full dose for cycle 2; if reduced by 50 % for the first dose, increase to 75 % of full dose for cycle 2.The dosage can be increased to full dose for subsequent cycles if tolerated. Doxorubicin can be administered to patients with liver metastases with concurrent elevation of bilirubin and liver enzymes up to 4x the upper limit of the normal range. Prior to doxorubicin administration, evaluate hepatic function using conventional clinical laboratory tests such as ALT/AST, alkaline phosphatase, and bilirubin.
Other population: AIDS-KS patients with splenectomy: As there is no experience with doxorubicin in patients with splenectomy, treatment with doxorubicin is not recommended.
Method of administration: For doses < 90 mg: dilute Doxorubicin in 250 ml Dextrose 5% in water.
For doses ≥ 90 mg: dilute Doxorubicin in 500 ml Dextrose 5% in water.
If the patient experiences early symptoms or signs of infusion reaction, immediately discontinue the infusion, give appropriate premedications (antihistamine and/or short acting corticosteroid) and restart at a slower rate.
DO NOT administer as a bolus injection or undiluted solution. It is recommended that the doxorubicin infusion line be connected through the side port of an intravenous infusion of Dextrose 5% in Water to achieve further dilution and minimize the risk of thrombosis and extravasation. The infusion may be given through a peripheral vein. Doxorubicin must not be given by the intramuscular or subcutaneous route. Do not use with in-line filters.
Breast cancer/Ovarian cancer: To minimise the risk of infusion reactions, the initial dose is administered at a rate no greater than 1 mg/minute. If no infusion reaction is observed, subsequent Doxorubicin infusions may be administered over a 60-minute period.
In the breast cancer trial program, modification of the infusion was permitted for those patients experiencing an infusion reaction as follows: 5% of the total dose should be infused slowly over the first 15 minutes. If tolerated without reaction, the infusion rate was doubled for the next 15 minutes. If tolerated, the infusion was completed over the next hour for a total infusion time of 90 minutes. Subsequent doxorubicin infusions may be administered over a 60 minute period.
Multiple myeloma: The intravenous catheter and tubing should be flushed with 5% glucose solution for infusion between administration of doxorubicin and bortezomib. Day 4 dosing of both medicinal products may be delayed up to 48 hours as medically necessary. Doses of bortezomib should be at least 72 hours apart. The first infusion of doxorubicin should be administered over 90 minutes, as follows: 10 mL over first 10 minutes; 20 mL over next 10 minutes; 40 mL over next 10 minutes; Then, complete the infusion over a total of 90 minutes.
Subsequent doses of doxorubicin will be administered over 1 hour, as tolerated. If an infusion reaction to doxorubicin occurs, stop the infusion and after the symptoms resolve, attempt to administer the remaining doxorubicin over 90 minutes, as follows: 10 mL over first 10 minutes; 20 mL over next 10 minutes; 40 mL over next 10 minutes; then, complete the remaining infusion over a total of 90 minutes. Infusion may be given through a peripheral vein or a central line.
AIDS-related KS: Doxorubicin, diluted in 250 ml Dextrose 5% in water, is administered by intravenous infusion over 30 minutes.