


 Sign Out
Sign Out

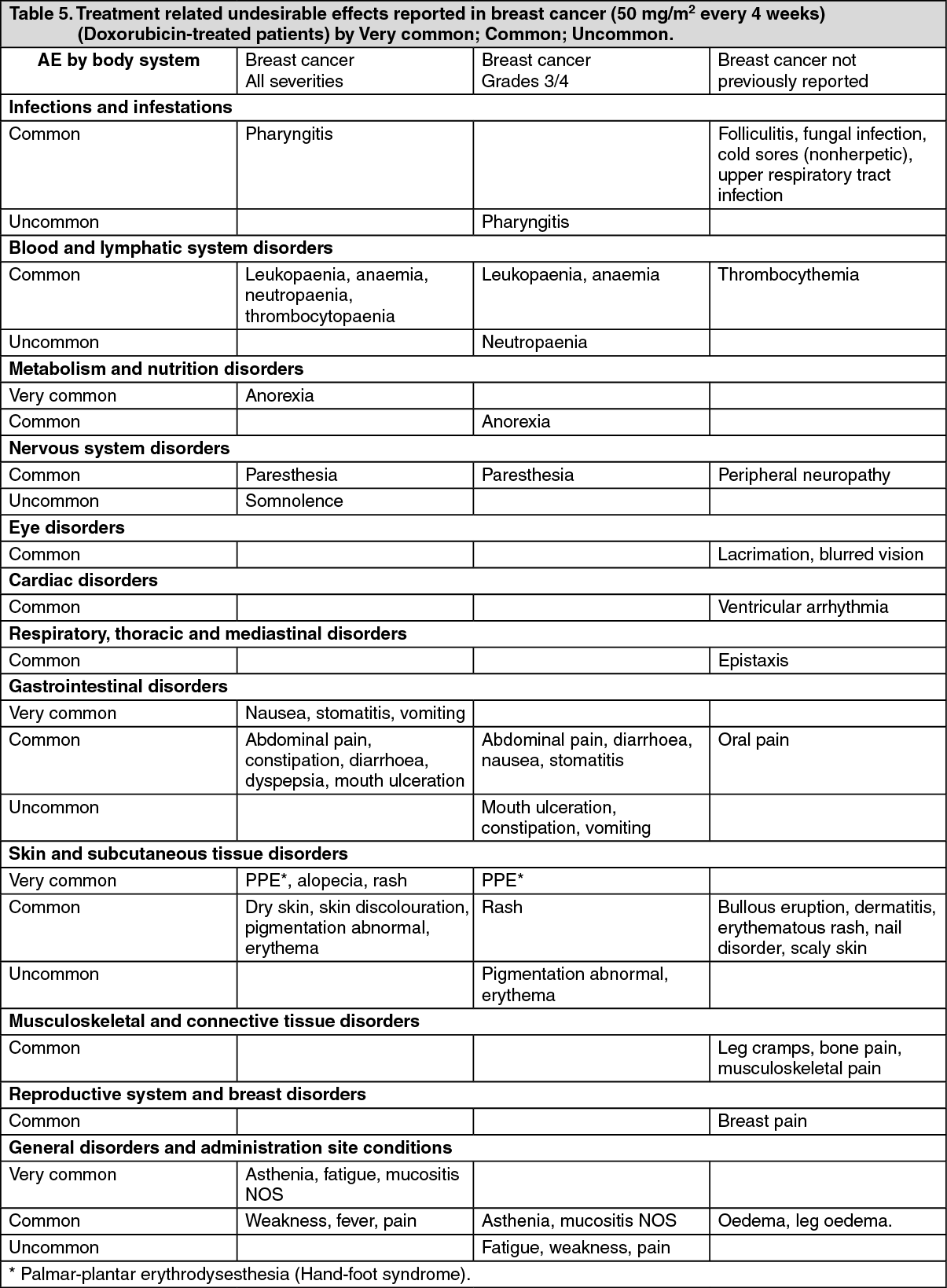
Breast cancer: The following common adverse events were reported more often with doxorubicin at a dose of 50 mg/m2 every 4 weeks than with Doxorubicin 60 mg/m2 every 3 weeks: nausea, vomiting, any alopecia, pronounced alopecia, and neutropaenia.
Mucositis and stomatitis were reported more commonly with Doxorubicin than with doxorubicin. The average duration of the most common severe (grade 3/4) events for both groups was 30 days or less. See Table 5 for complete listing of undesirable effects reported in Doxorubicin-treated patients.
The incidence of life threatening (grade 4) haematologic effects and sepsis was reported. Growth factor support or transfusion support was necessary.
Clinically significant laboratory abnormalities (grades 3 and 4) in this group was low with elevated total bilirubin, AST and ALT reported. No clinically significant increases in serum creatinine were reported. (See Table 5.)
 Click on icon to see table/diagram/image
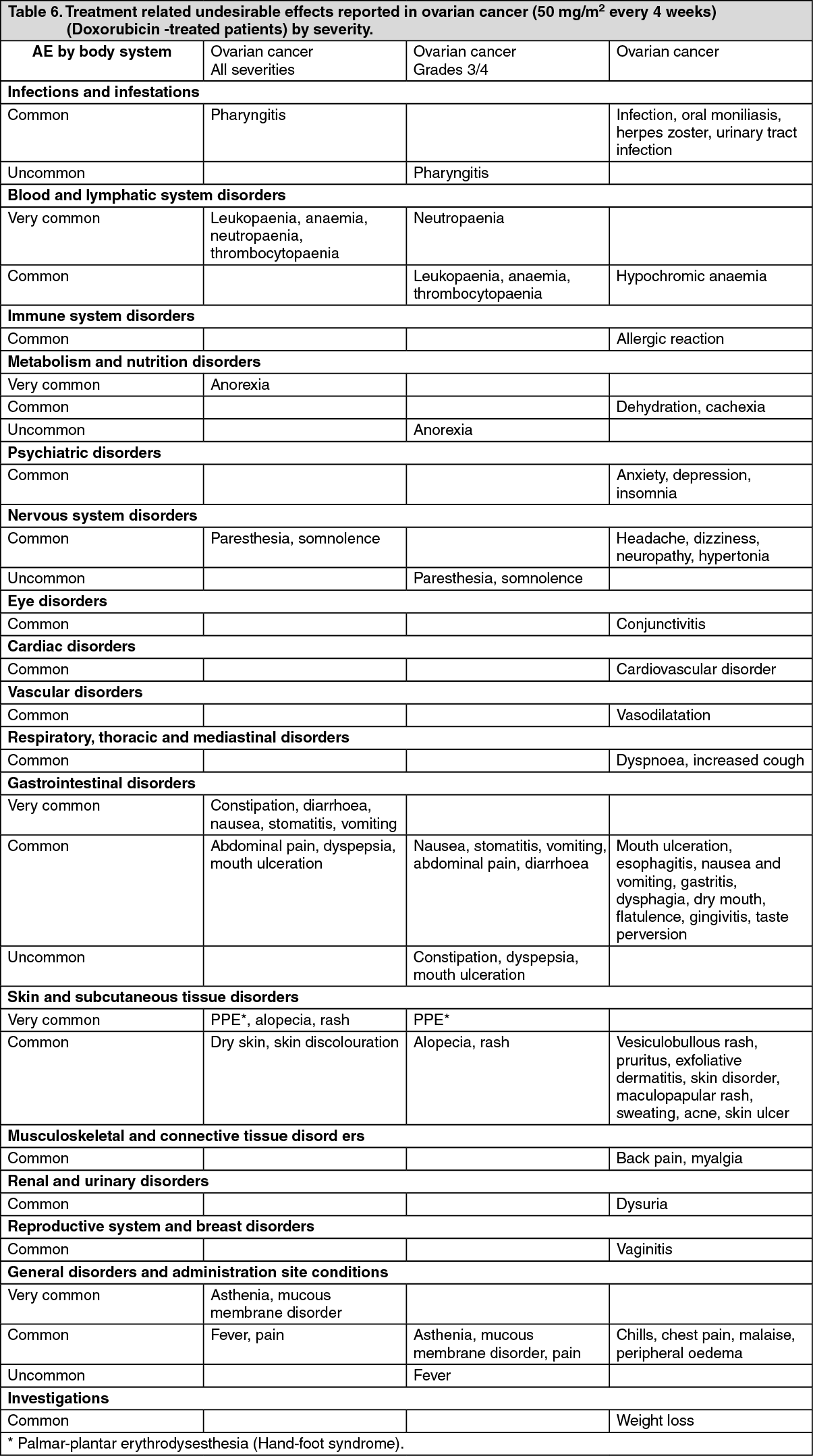
Click on icon to see table/diagram/imageOvarian cancer: Patients with ovarian cancer (a subset of 876 solid tumour patients) were treated with Doxorubicin at a dose of 50 mg/m2. See Table 6 for undesirable effects reported in Doxorubicin-treated patients. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMyelosuppression was mostly mild or moderate and manageable. Sepsis related to leukopaenia was observed infrequently. Growth factor support was required infrequently and transfusion support was required in approximately 15% of patients.
In patients with ovarian cancer, increases in total bilirubin (usually in patients with liver metastases) and serum creatinine levels. Increases in AST were less frequently reported.
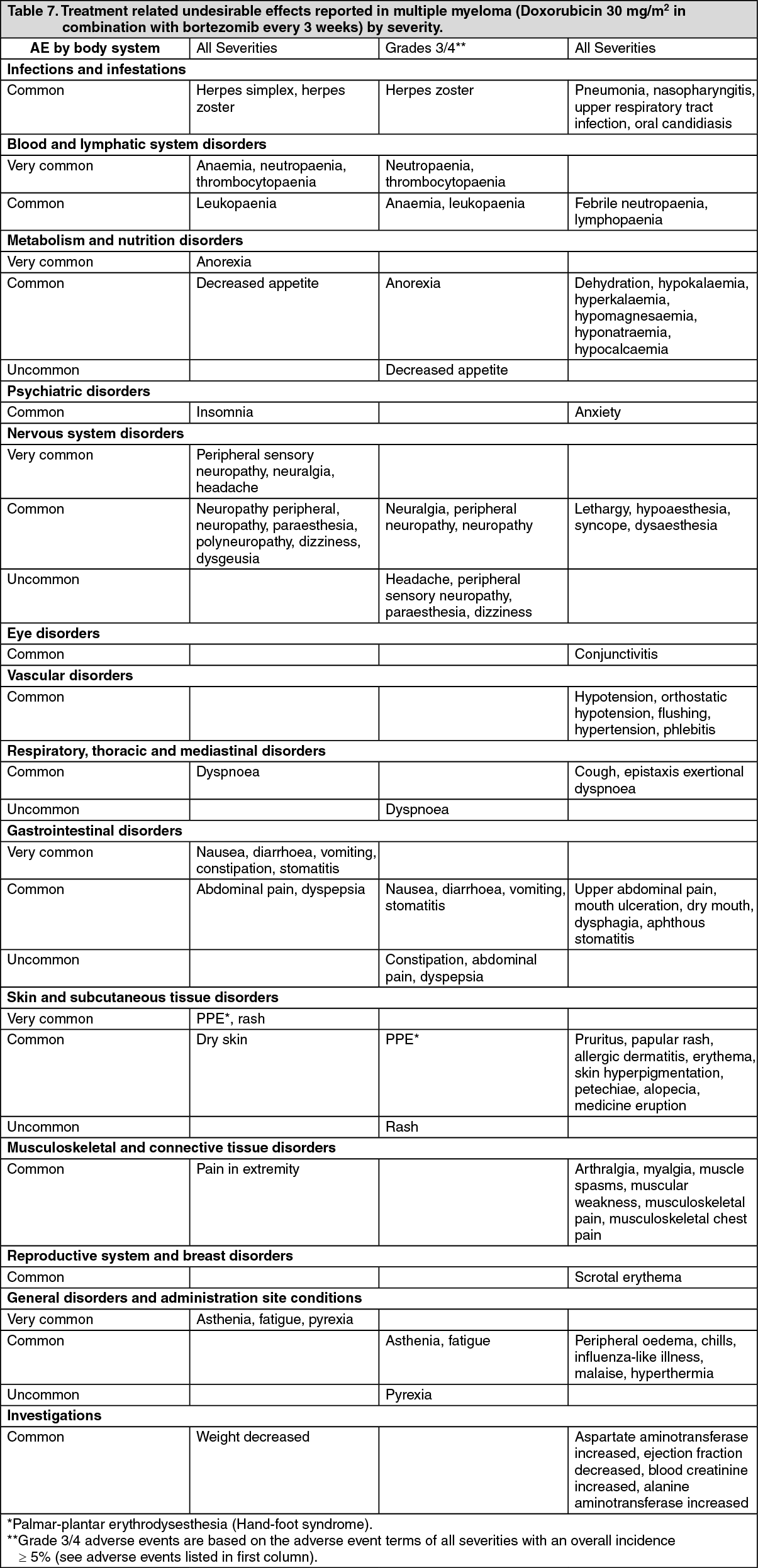
Multiple myeloma: Patients with multiple myeloma who have received at least 1 prior therapy, treated with combination therapy of Doxorubicin 30 mg/m2 as a one hour intravenous infusion administered on day 4 following bortezomib which is administered at 1.3 mg/m2 on days 1, 4, 8, and 11, every three weeks or with bortezomib monotherapy. See Table 7 for adverse effects reported in patients treated with combination therapy of Doxorubicin plus bortezomib.
Neutropaenia, thrombocytopaenia, and anaemia were the most frequently reported hematologic events reported with both combination therapy of Doxorubicin plus bortezomib and bortezomib monotherapy. The incidence of grade 3 and 4 neutropaenia was higher in the combination therapy group than in the monotherapy group. The incidence of grade 3 and 4 thrombocytopaenia washigher in the combination therapy group than in the monotherapy group. The incidence of anaemia was similar in both treatment groups.
Stomatitis was reported more frequently in the combination therapy group than in the monotherapy group, and most cases were grade 2 or less in severity. Grade 3 stomatitis was reported in patients in the combination therapy group. No grade 4 stomatitis was reported.
Nausea and vomiting were reported more frequently in the combination therapy group than in the monotherapy group and were mostly grade 1 and 2 in severity.
Treatment discontinuation of one or both agents due to adverse events was seen in 38% of patients. Common adverse events which led to treatment discontinuation of bortezomib and Doxorubicin included PPE, neuralgia, peripheral neuropathy, peripheral sensory neuropathy, thrombocytopaenia, decreased ejection fraction, and fatigue. (See Table 7.)
 Click on icon to see table/diagram/image
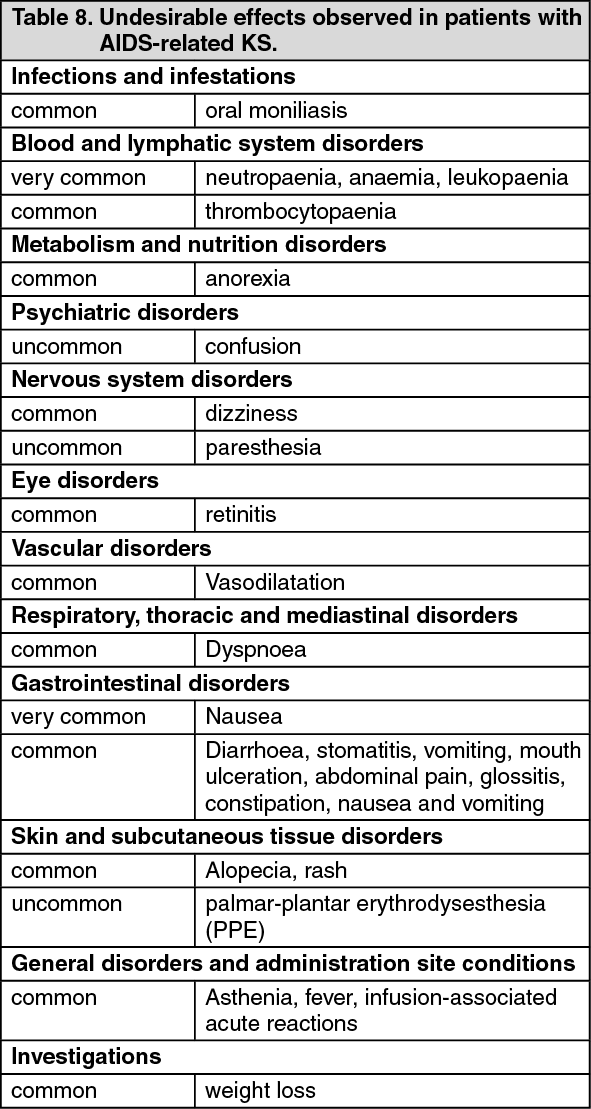
Click on icon to see table/diagram/imageAIDS-related KS: AIDS-KS patients treated at 20 mg/m2 with Doxorubicin show that myelosuppression was the most frequent undesirable effect considered related to Doxorubicin occurring very commonly.
Leukopaenia is the most frequent undesirable effect experienced with Doxorubicin in this population; neutropaenia, anaemia and thrombocytopaenia have been observed. These effects may occur early on in treatment. Haematological toxicity may require dose reduction or suspension or delay of therapy. Temporarily suspend Doxorubicin treatment in patients when the ANC count is < 1,000/mm3 and/or the platelet count is < 50,000/mm3. G-CSF (or GM-CSF) may be given as concomitant therapy to support the blood count when the ANC count is < 1,000/mm3 in subsequent cycles. The haematological toxicity for ovarian cancer patients is less severe than in the AIDS-KS.
Respiratory undesirable effects commonly occurred with Doxorubicin and may be related to opportunistic infections in the AIDS population. Opportunistic infections (OI's) are observed in KS patients after administration with Doxorubicin, and are frequently observed in patients with HIV-induced immunodeficiency. The most frequently observed OI's were candidiasis, cytomegalovirus, herpes simplex, Pneumocystis carinii pneumonia, and mycobacterium avium complex. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOther less frequently observed undesirable effects included hypersensitivity reactions including anaphylactic reactions. Following marketing, bullous eruption has been reported rarely in this population. Clinically significant laboratory abnormalities frequently occurred including increases in alkaline phosphatase; AST and bilirubin which were believed to be related to the underlying disease and not Doxorubicin. Reduction in haemoglobin and platelets were less frequently reported. Sepsis-related to leukopaenia was rarely observed. Some of these abnormalities may have been related to the underlying HIV infection and not Doxorubicin.
All patients: Patients with solid tumours were described as having an infusion-associated reaction during treatment with Doxorubicin as defined by the following Costart terms: allergic reaction, anaphylactoid reaction, asthma, face oedema, hypotension, vasodilatation, urticaria, back pain, chest pain, chills, fever, hypertension, tachycardia, dyspepsia, nausea, dizziness, dyspnoea, pharyngitis, rash, pruritus, sweating, injection site reaction and medicinal product interaction. Permanent treatment discontinuation was infrequently reported. A similar incidence of infusion reactions and treatment discontinuation was observed in the breast cancer program. In patients with multiple myeloma receiving Doxorubicin plus bortezomib, infusion-associated reactions have been reported. In patients with AIDS-KS, infusion-associated reactions, were characterised by flushing, shortness of breath, facial oedema, headache, chills, back pain, tightness in the chest and throat and/or hypotension. Very rarely, convulsions have been observed in relation to infusion reactions. In all patients, infusion-associated reactions occurred primarily during the first infusion. Temporarily stopping the infusion usually resolves these symptoms without further therapy. In nearly all patients, Doxorubicin treatment can be resumed after all symptoms have resolved without recurrence. Infusion reactions rarely recur after the first treatment cycle with Doxorubicin.
Myelosuppression associated with anaemia, thrombocytopaenia, leukopaenia, and rarely febrile neutropaenia, has been reported in Doxorubicin-treated patients.
Stomatitis has been reported in patients receiving continuous infusions of conventional doxorubicin hydrochloride and was frequently reported in patients receiving Doxorubicin. It did not interfere with patients completing therapy and no dosage adjustments are generally required, unless stomatitis is affecting a patient's ability to eat. In this case, the dose interval may be extended by 1-2 weeks or the dose reduced.
An increased incidence of congestive heart failure is associated with doxorubicin therapy at cumulative lifetime doses > 450 mg/m2 or at lower doses for patients with cardiac risk factors. Endomyocardial biopsies on nine of ten AIDS-KS patients receiving cumulative doses of Doxorubicin greater than 460 mg/m2 indicate no evidence of anthracycline-induced cardiomyopathy. The recommended dose of Doxorubicin for AIDS-KS patients is 20 mg/m2 every two-to-three weeks. The cumulative dose at which cardiotoxicity would become a concern for these AIDS-KS patients (> 400 mg/m2) would require more than 20 courses of Doxorubicin therapy over 40 to 60 weeks.
In addition, endomyocardial biopsies were performed in 8 solid tumour patients with cumulative anthracycline doses of 509 mg/m2-1,680 mg/m2. The range of Billingham cardiotoxicity scores was grades 0-1.5. These grading scores are consistent with no or mild cardiac toxicity.
Cardiac toxicity was defined as a decrease of 20 points or greater from baseline if the resting LVEF remained in the normal range or a decrease of 10 points or greater if the LVEF became abnormal (less than the lower limit for normal). In patients with solid tumours, including a subset of patients with breast and ovarian cancers, treated at a dose of 50 mg/m2/cycle with lifetime cumulative anthracycline doses up to 1,532 mg/m2, the incidence of clinically significant cardiac dysfunction was low.
As with other DNA-damaging antineoplastic agents, secondary acute myeloid leukemias and myelodysplasias have been reported in patients having received combined treatment with doxorubicin. Therefore, any patient treated with doxorubicin should be kept under haematological supervision.
Although local necrosis following extravasation has been reported very rarely, Doxorubicin is considered to be an irritant. Animal studies indicate that administration of doxorubicin hydrochloride as a liposomal formulation reduces the potential for extravasation injury. If any signs or symptoms of extravasation occur (e.g., stinging, erythema) terminate the infusion immediately and restart in another vein. The application of ice over the site of extravasation for approximately 30 minutes may be helpful in alleviating the local reaction. Doxorubicin must not be given by the intramuscular or subcutaneous route.
Recall of skin reaction due to prior radiotherapy has rarely occurred with Doxorubicin administration.
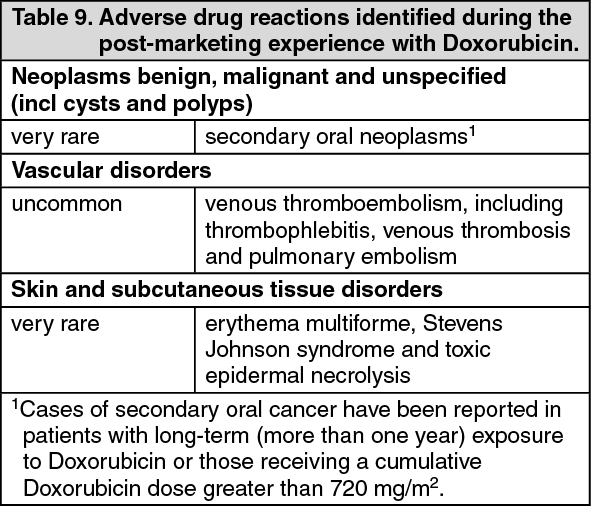
Post-marketing experience: Adverse drug reactions identified during the post-marketing experience with Doxorubicin are described in Table 9. The frequencies are provided according to the following convention: Very common; Common and Uncommon; Rare; Very rare including isolated reports. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form