Active ingredient: ganciclovir in the form of the sodium salt.
Vials containing dry substance equivalent to 500 mg ganciclovir and approximately 43 mg (2 mEq) sodium.
The vial content is a white to off-white solid and the constituted solution in water is colourless to light yellow.
Therapeutic/Pharmacologic Class of Drug: Antiviral. ATC code: J05AB06.
Pharmacology: Pharmacodynamics: Mechanism of Action: Ganciclovir is a synthetic analogue of 2'-deoxyguanosine which inhibits replication of herpes viruses in vitro and in vivo. Sensitive human viruses include human cytomegalovirus (HCMV), herpes-simplex virus-1 and -2 (HSV-1 and HSV-2), human herpes virus -6, -7 and -8 (HHV-6, HHV-7, HHV-8), Epstein-Barr virus (EBV), varicella-zoster virus (VZV) and hepatitis B virus. However, clinical studies have been limited to assessment of efficacy in patients with CMV infection.
In CMV infected cells ganciclovir is initially phosphorylated to ganciclovir monophosphate by the viral protein kinase, UL97. Further phosphorylation occurs by several cellular kinases to produce ganciclovir triphosphate, which is then slowly metabolised intracellularly. This has been shown to occur in HSV- and HCMV-infected cells with half-lives of 18 and between 6 and 24 hours respectively after removal of extracellular ganciclovir. As the phosphorylation is largely dependent on the viral kinase, phosphorylation of ganciclovir occurs preferentially in virus-infected cells.
The virustatic activity of ganciclovir is due to the inhibition of viral DNA synthesis by: (1) competitive inhibition of incorporation of deoxyguanosine triphosphate into DNA by DNA polymerase, and (2) incorporation of ganciclovir triphosphate into viral DNA causing termination of, or very limited, viral DNA elongation. Typical anti-viral IC50 against CMV in vitro is in the range 0.08 μM (0.02 μg/mL) to 14 μgM (3.5 μg/mL).
Clinical/Efficacy Studies: No text on clinical studies.
Viral resistance: Viruses resistant to ganciclovir can arise after chronic dosing with ganciclovir or valganciclovir by selection of mutations in either the viral kinase gene (UL97) responsible for ganciclovir monophosphorylation or the viral polymerase gene (UL54).
UL97 mutations arise earlier and more frequently than mutations in UL54. Virus containing mutations in the UL97 gene is resistant to ganciclovir alone, with M460V/I, H520Q, C592G, A594V, L595S, C603W being the most frequently reported ganciclovir resistance-associated substitutions. Mutations in the UL54 gene may show cross-resistance to other antivirals targeting the viral polymerase, and vice versa [106, 107, 108]. Amino acid substitutions in UL54 conferring cross-resistance to ganciclovir and cidofovir are generally located within the exonuclease domains and region V, however amino acid substitutions conferring cross-resistance to foscarnet are diverse, but concentrate at and between regions II (codon 696-742) and III (codon 805-845).
The possibility of viral resistance should be considered in patients who repeatedly show poor clinical response or experience continuous viral excretion during treatment.
Pharmacokinetics: The pharmacokinetics of IV ganciclovir is linear over the range of 1.6 - 5.0 mg/kg.
The systemic exposure (AUC0-24) reported following dosing with a single 1-hour IV infusion of 5 mg/kg ganciclovir in HIV+/CMV+ patients or in adult AIDS patients ranged from 18.8 to 26.0 μg·h/mL. In this patient population peak plasma concentration (Cmax) ranged from 7.59 to 9.03 μg/mL.
Absorption: Not applicable.
Distribution: For IV ganciclovir, the volume of distribution is correlated with body weight with values for the steady state volume of distribution ranging from 0.54 to 0.87 L/kg. Ganciclovir penetrates the cerebrospinal fluid, and diffuses across the placenta. Binding to plasma proteins was 1-2% over ganciclovir concentrations of 0.5 and 51 μg/mL.
Metabolism: Ganciclovir is not metabolized to a significant extent.
Elimination: Renal excretion of unchanged drug by glomerular filtration and active tubular secretion is the major route of elimination of ganciclovir. In patients with normal renal function, greater than 90% of IV administered ganciclovir was recovered unmetabolized in the urine within 24 hours. In patients with normal renal function, systemic clearance ranged from 2.64 ±0.38 mL/min/kg (N=15) to 4.52 ±2.79 mL/min/kg (N=6) and renal clearance ranged from 2.57 ±0.69 mL/min/kg (N=15) to 3.48 ±0.68 mL/min/kg (N=20), corresponding to 90-101% of administered ganciclovir. Half-lives in patients without renal impairment ranged from 2.73 ±1.29 (N=6) to 3.98 ±1.78 hours (N=8).
Pharmacokinetics in Special Populations: Pediatric Population: Ganciclovir pharmacokinetics were studied in 27 neonates aged 2 to 49 days at intravenous doses of 4 mg/kg (N=14) and 6 mg/kg (N=13). Mean Cmax was 5.5 ±6 μg/mL and 7.0 ±1.6 μg/mL the lower and higher dose levels respectively. Mean values for Vss (0.7 L/kg) and systemic clearance (3.15 ±0.47 mL/min/kg at 4 mg/kg and 3.55 ±0.35 mL/min/kg at 6 mg/kg) were comparable to those observed in adults with normal renal function.
Ganciclovir pharmacokinetics were also studied in 10 children with normal renal function, aged 9 months to 12 years. The pharmacokinetic characteristics of ganciclovir were the same after single and multiple (q12h) IV doses (5 mg/kg). Exposure as measured by mean AUC∞ on days 1 and 14 were 19.4 ±7.1 and 24.1 ±14.6 μg·h/mL respectively and the corresponding Cmax values were 7.59 ±3.21 (day 1) and 8.31 ±4.9 μg/mL (day 14). These range of exposures are comparable to those observed in adults. The steady state volume of distribution after a single dose on day 1 and at the end of the repeat dose period (day 14) was 0.68 ±0.20 L/kg. Systemic clearance for the same study days was 4.66 ±1.72 (day 1) and 4.86 ±2.96 mL/min/kg (day 14). The respective mean values for renal clearance (0 - 12 h) were 3.49 ±2.40 on day 1 and 3.49 ±1.19 mL/min/kg on day 14. The corresponding mean values for the half-life were 2.49 ±0.57 (day 1) and 2.22 ±0.76 h (day 14). The pharmacokinetics of ganciclovir from this study were consistent with those in neonates and adults.
Geriatric population: No ganciclovir pharmacokinetic studies have been conducted in adults older than 65 years of age. However, because ganciclovir is mainly renally excreted and since renal clearance decreases with age a decrease in ganciclovir total body clearance and prolongation of ganciclovir elimination half-life can be anticipated in the elderly (see Special dosage instructions: Geriatric patients under Dosage & Administration).
Renal impairment: The total body clearance of ganciclovir is linearly correlated with creatinine clearance. In patients with mild, moderate, and severe renal impairment, mean systemic clearances of 2.1, 1.0 and 0.3 mL/min/kg were observed. Patients with renal impairment show an increased elimination half-life. In patients with severe renal impairment elimination half-life was increased by 10-fold (see Special dosage instructions: Patients with renal impairment under Dosage & Administration).
Patients undergoing hemodialysis: Plasma concentrations of ganciclovir are reduced by about 50% during a 4 hour hemodialysis session (see Overdosage).
During intermittent hemodialysis, estimates for the clearance of ganciclovir ranged from 42 to 92 mL/min, resulting in intra-dialytic half-lives of 3.3 to 4.5 hours. Estimates of ganciclovir clearance for continuous dialysis were lower (4.0 to 29.6 mL/min) but resulted in greater removal of ganciclovir over a dose interval. For intermittent hemodialysis, the fraction of ganciclovir removed in a single dialysis session varied from 50-63%.
Hepatic impairment: No pharmacokinetic study has been conducted and no population PK data were collected in patients with hepatic impairment undergoing ganciclovir therapy. Hepatic impairment is not anticipated to affect the pharmacokinetics of ganciclovir since ganciclovir is excreted renally (see Elimination as previously mentioned).
Toxicology: Preclinical Safety: Carcinogenicity: Ganciclovir was mutagenic in mouse lymphoma cells and clastogenic in mammalian cells. Such results are consistent with the positive mouse carcinogenicity study with ganciclovir. Ganciclovir is a potential carcinogen.
Genotoxicity: Ganciclovir was mutagenic in mouse lymphoma cells and clastogenic in mammalian cells.
Impairment of Fertility: Ganciclovir causes impaired fertility and teratogenicity in animals (see Precautions).
Based upon animal studies where aspermia was induced at ganciclovir systemic exposures below therapeutic levels, it is considered likely that ganciclovir could cause temporary or permanent inhibition of human spermatogenesis (see Females and Males of Reproductive Potential: Fertility under Use in Pregnancy & Lactation).
Reproductive toxicity: Ganciclovir causes teratogenicity in animals.
Cytomegalovirus retinitis in immunocompromised individuals including patients with acquired immunodeficiency syndrome (AIDS). Prevention of CMV disease in transplant patients at risk for CMV disease. Prevention and treatment of life- or sight-threatening cytomegalovirus (CMV) disease in immunocompromised individuals.
General: Caution: Do not administer by rapid or bolus IV injection. The toxicity of Cymevene may be increased as a result of excessive plasma levels.
I.M. or S.C. injection may result in severe tissue irritation due to the high pH (~11) of ganciclovir solutions.
The recommended dosage, frequency, or infusion rates should not be exceeded. See Special Instructions for Use, Handling and Disposal under Cautions for Usage for details of preparation and handling of Cymevene solution.
Standard dosage for treatment of CMV retinitis: Induction treatment: 5 mg/kg given as an IV infusion over one hour, every 12 hours for 14-21 days in patients with normal renal function.
Maintenance treatment: 5 mg/kg given as an IV infusion over one hour, once daily on 7 days per week or 6 mg/kg once daily on 5 days per week.
Standard dosage for prevention in transplant recipients: Induction treatment: 5 mg/kg given as an IV infusion over one hour, every 12 hours for 7-14 days in patients with normal renal function.
Maintenance treatment: 5 mg/kg given as an IV infusion over one hour, once daily on 7 days per week or 6 mg/kg once daily on 5 days per week.
Special dosage instructions: Pediatric patients: Safety and efficacy of ganciclovir in pediatrics have not been established, including use for the treatment of congenital or neonatal CMV infections. The use of Cymevene in children warrants extreme caution due to the potential for long-term carcinogenicity and reproductive toxicity. The benefits of treatment should outweigh the risks (see Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations: Pediatric Population under Actions).
Geriatric patients: No studies have been conducted in adults older than 65 years of age. Since renal clearance decreases with age, Cymevene should be administered to geriatric patients with special consideration of their renal status (see Table 1 and Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations: Geriatric population under Actions).
Patients with renal impairment: For patients with renal impairment, the dose of Cymevene should be modified as shown in Table 1 as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Estimated creatinine clearance can be related to serum creatinine by the following formulae: (See formula.)
Click on icon to see table/diagram/image
As dosage modifications are recommended in patients with renal impairment, serum creatinine or estimated creatinine-clearance levels should be monitored carefully.
Hepatic impairment: The safety and efficacy of Cymevene have not been studied in patients with hepatic impairment (see Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations: Hepatic impairment under Actions).
Overdose experience with intravenous ganciclovir: Reports of overdoses with intravenous ganciclovir, some with fatal outcomes, have been received from clinical trials and during post-marketing experience. In some of these cases no adverse events were reported. The majority of patients experienced one or more of the following adverse events: Hematological toxicity: myelosuppression including pancytopenia, bone marrow failure, leukopenia, neutropenia, granulocytopenia.
Hepatotoxicity: hepatitis, liver function disorder.
Renal toxicity: worsening of hematuria in a patient with pre-existing renal impairment, acute kidney injury, elevated creatinine.
Gastrointestinal toxicity: abdominal pain, diarrhea, vomiting.
Neurotoxicity: generalised tremor, seizure.
Hemodialysis and hydration may be of benefit in reducing blood plasma levels in patients who receive an overdose of ganciclovir (see Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Cymevene is contraindicated in patients with hypersensitivity to ganciclovir, valganciclovir or to any of the excipients.
Breast-feeding (see Lactation under Use in Pregnancy & Lactation).
General: Cross hypersensitivity: Due to the similarity of the chemical structure of ganciclovir and that of aciclovir and penciclovir, a cross-hypersensitivity reaction between these drugs is possible. Caution should therefore be used when prescribing Cymevene to patients with known hypersensitivity to aciclovir or penciclovir, (or to their prodrugs, valaciclovir or famciclovir respectively).
Mutagenicity, teratogenicity, carcinogenicity, fertility and contraception: In animal studies ganciclovir was found to be mutagenic, teratogenic carcinogenic and to impair fertility. Cymevene should therefore be considered a potential teratogen and carcinogen in humans with the potential to cause birth defects and cancers. Prior to initiation of ganciclovir treatment, patients should be advised of the potential risks to the fetus and to use contraceptive measures. Based on clinical and nonclinical studies, Cymevene may cause temporary or permanent inhibition of spermatogenesis in males (see Use in Pregnancy & Lactation, Adverse Reactions, Pharmacology: Toxicology: Preclinical Safety under Actions, and Special Instructions for Use, Handling and Disposal under Cautions for Usage).
Myelosuppression: Cymevene should be used with caution in patients with pre-existing hematological cytopenia or a history of drug-related hematological cytopenia and in patients receiving radiotherapy.
Severe leukopenia, neutropenia, anemia, thrombocytopenia, pancytopenia, bone marrow failure and aplastic anemia have been observed in patients treated with Cymevene. Therapy should not be initiated if the absolute neutrophil count is less than 500 cells/μL or the platelet count is less than 25,000 cells/μL or the hemoglobin is less than 8 g/dL (see Adverse Reactions).
It is recommended that complete blood counts and platelet counts be monitored in all patients during therapy, particularly in patients with renal impairment (see Special dosage instructions under Dosage & Administration).
In patients with severe leukopenia, neutropenia, anemia and/or thrombocytopenia, that treatment with hematopoietic growth factors and/or the interruption of therapy is recommended (see Adverse Reactions).
Use with other medicines: Seizures have been reported in patients taking imipenem-cilastatin and ganciclovir. Cymevene should not be used concomitantly with imipenem-cilastatin unless the potential benefits outweigh the potential risks (see Interactions).
Zidovudine and Cymevene each have the potential to cause neutropenia and anemia. Some patients may not tolerate concomitant therapy at full dosage (see Interactions).
Didanosine plasma concentrations may increase during concomitant use with Cymevene; therefore, patients should be closely monitored for didanosine toxicity (see Interactions).
Concomitant use of other drugs that are known to be myelosuppressive or associated with renal impairment with Cymevene may result in added toxicity (see Interactions).
Drug Abuse and Dependence: No information is available for drug abuse and dependence with Cymevene.
Ability to Drive and Use Machines: No studies on the effect on the ability to drive and use machines have been performed. Based on the adverse reaction profile, ganciclovir may have a minor influence on the ability to drive and use machines. Adverse reactions, for example seizures, dizziness and confusion may occur in patients receiving Cymevene (see Adverse Reactions). If they occur, such effects may affect tasks requiring alertness including the patient's ability to drive and operate machinery.
Renal Impairment: In patients with renal impairment, dosage adjustments based on creatinine clearance are required (see Special dosage instructions: Patients with renal impairment under Dosage & Administration and Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Hepatic Impairment: The safety and efficacy of Cymevene have not been studied in patients with hepatic impairment (see Special dosage instructions under Dosage & Administration and Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions).
Use in Children: See Special dosage instructions under Dosage & Administration and Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions.
Use in the Elderly: See Special dosage instructions under Dosage & Administration and Pharmacology: Pharmacokinetics: Pharmacokinetics in Special Populations under Actions.
Females and Males of Reproductive Potential: Fertility: In animal studies ganciclovir was found to impair fertility (see Pharmacology: Toxicology: Preclinical Safety: Impairment of Fertility under Actions). In a clinical study renal transplant patients receiving Valcyte (which is a pro-drug of Cymevene) for CMV prophylaxis for up to 200 days were compared to an untreated control group. Spermatogenesis was inhibited during treatment with Valcyte. At follow-up, approximately six months after treatment discontinuation, the mean sperm density in treated patients was comparable to that observed in the untreated control group. In Valcyte treated patients, all patients with normal sperm density (n=7) and 8/13 patients with low sperm density at baseline, recovered to normal counts after treatment cessation. In the control group, all patients with normal sperm density (n=6) and 2/4 patients with low sperm density at baseline, had normal density at the end of follow-up.
Contraception: Women of reproductive potential should be advised to use effective contraception during and for at least 30 days after treatment. Sexually active men are recommended to use condoms during and for at least 90 days after cessation of treatment with Cymevene, unless it is certain that the female partner is not at risk of becoming pregnant (see General: Mutagenicity, teratogenicity, carcinogenicity, fertility and contraception under Precautions and Pharmacology: Toxicology: Preclinical Safety: Reproductive toxicity under Actions).
Pregnancy: In animal studies ganciclovir was associated with reproductive toxicity and teratogenicity (see Pharmacology: Toxicology: Preclinical Safety: Impairment of Fertility and Reproductive toxicity under Actions).
The safety of Cymevene in pregnant women has not been established. However, ganciclovir readily diffuses across the human placenta. The use of Cymevene should be avoided in pregnant women unless the benefit to the mother outweighs the potential risk to the fetus. The safe use of Cymevene during labor and delivery has not been established.
Lactation: Peri- and postnatal development has not been studied with ganciclovir but the possibility of ganciclovir being excreted in breast milk and causing serious adverse reactions in the nursing infant cannot be discounted. Human data are not available but animal data indicates that ganciclovir is excreted in the milk of lactating rats. Therefore, a decision should be made to discontinue the drug or discontinue nursing taking into consideration the potential benefit of Cymevene to the nursing mother.
Clinical Trials: Valganciclovir is a pro-drug of ganciclovir, and adverse reactions associated with valganciclovir can be expected to occur with ganciclovir. Therefore, adverse drug reactions reported with IV or oral ganciclovir (no longer available) or with valganciclovir are included in the table of adverse reactions (see Table 2).
In patients treated with ganciclovir/valganciclovir the most serious and frequent adverse drug reactions are hematological reactions and include neutropenia, anemia and thrombocytopenia.
The frequencies presented in the table of adverse reactions are derived from a pooled population of HIV-infected patients (n=1704) receiving maintenance therapy with ganciclovir (GAN1697, GAN1653, GAN2304, GAN1774, GAN2226, AVI034, GAN041) or valganciclovir (WV15376, WV15705). Exception is made for agranulocytosis, granulocytopenia and anaphylactic reaction; the frequencies of which are derived from post-marketing experience.
Frequencies are presented as percentages and as CIOMS frequency categories defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000) and very rare (< 1/10,000).
The overall safety profile of ganciclovir/valganciclovir is consistent in HIV and transplant populations except that retinal detachment has only been reported in HIV patients with CMV retinitis. However, there are some differences in the frequency of certain reactions.
Intravenous ganciclovir is associated with a lower risk of diarrhea compared to oral valganciclovir. Pyrexia, candida infections, depression, severe neutropenia (ANC <500 μL) and skin reactions are reported more frequently in patients with HIV. Renal and hepatic dysfunction is reported more frequently in organ transplant recipients. (See Table 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: Neutropenia: The risk of neutropenia is not predictable on the basis of the number of neutrophils before treatment. Neutropenia usually occurs during the first or second week of induction therapy. The cell count usually normalizes within 2 to 5 days after discontinuation of the drug or dose reduction (see Precautions).
Thrombocytopenia: Patients with low baseline platelet counts (< 100,000/μL) have an increased risk of developing thrombocytopenia. Patients with iatrogenic immunosuppression due to treatment with immunosuppressive drugs are at greater risk of thrombocytopenia than patients with HIV (see Precautions). Severe thrombocytopenia may be associated with potentially life-threatening bleeding.
Laboratory Abnormalities: Laboratory abnormalities in HIV infected patients: Laboratory abnormalities reported from three clinical trials in HIV infected patients receiving intravenous ganciclovir as maintenance treatment for CMV retinitis are listed as follows in Table 3. One hundred seventy-nine patients were eligible for the laboratory abnormality analysis. (See Table 3.)
Click on icon to see table/diagram/image
Post-marketing Experience: Safety reports from the postmarketing setting are consistent with safety data from clinical trials with ganciclovir and valganciclovir (see Table 2 previously).
Imipenem-cilastatin: Convulsions have been reported in patients who received ganciclovir and imipenem-cilastatin and a pharmacodynamic interaction between these two drugs cannot be discounted. These drugs should not be used concomitantly unless the potential benefits outweigh the risks (see General: Use with other medicines under Precautions).
Potential drug interactions: Toxicity may be enhanced when ganciclovir is co-administered with other drugs known to be myelosuppressive or associated with renal impairment. This includes nucleoside analogues (e.g. zidovudine, didanosine, stavudine), immunosuppressants (e.g. ciclosporin, tacrolimus, mycophenolate mofetil), antineoplastic agents (e.g. doxorubicin, vincristine, vinblastine, hydroxyurea), and anti-infectives (e.g. trimethoprim/sulphonamides, dapsone, amphotericin B, flucytosine, pentamidine). Therefore, these drugs should only be considered for concomitant use with ganciclovir if the potential benefits outweigh the potential risks (see General: Use with other medicines under Precautions).
Zidovudine: Both zidovudine and Cymevene have the potential to cause neutropenia and anemia, a pharmacodynamic interaction may occur during concomitant administration of these drugs some patients may not tolerate concomitant therapy at full dosage (see General: Use with other medicines under Precautions).
Didanosine: Didanosine plasma concentrations were found to be consistently raised when given with IV ganciclovir. At intravenous doses of 5 and 10 mg/kg/day, an increase in the AUC of didanosine ranging from 38 to 67% has been observed confirming a pharmacokinetic interaction during the concomitant administration of these drugs. There was no significant effect on ganciclovir concentrations. Patients should be closely monitored for didanosine toxicity (e.g. pancreatitis) (see General: Use with other medicines under Precautions).
Probenecid: Probenecid given with oral ganciclovir resulted in statistically decreased renal clearance of ganciclovir (20%) leading to statistically significant increased exposure (40%). These changes were consistent with a mechanism of interaction involving competition for renal tubular excretion. Therefore patients taking probenecid and Cymevene should be closely monitored for ganciclovir toxicity.
Special Instructions for Use, Handling and Disposal: Caution should be exercised in the handling of Cymevene.
Since Cymevene is considered a potential teratogen and carcinogen in humans, caution should be observed in its handling (see Precautions). Avoid inhalation or direct contact of the powder contained in the vials or direct contact of the reconstituted solution with the skin or mucous membranes. Cymevene solutions are alkaline (pH ~11). If such contact occurs, wash thoroughly with soap and water, rinse eyes thoroughly with plain water.
Wearing disposable gloves is recommended during reconstitution and when wiping the outer surface of the vials and the table after reconstitution.
Incompatibilities: Cymevene should not be mixed with other IV products.
Preparation of Cymevene reconstituted solution: 1. Lyophilized Cymevene should be reconstituted by injecting 10 mL of sterile water for injection into the vial. Do not use bacteriostatic water for injection containing parabens (para-hydroxybenzoates), since these are incompatible with Cymevene sterile powder and may cause precipitation.
2. The vial should be gently swirled in order to ensure complete wetting of the product. Continue swirling until a clear reconstituted solution is obtained. Reconstituted solution should be inspected for particulate matter prior to proceeding with admixture preparation.
3. From a microbiological point of view, the reconstituted solution should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user..
Preparation of Cymevene infusion solution: Based on patient weight the appropriate calculated dose volume should be removed from the Cymevene vial (concentration 50 mg/mL) and added to an acceptable infusion fluid. Normal saline, dextrose 5% in water, Ringer's or lactated Ringer's solution are determined chemically or physically compatible with Cymevene. Infusion concentrations greater than 10 mg/mL are not recommended.
From a microbiological perspective, because Cymevene is reconstituted with non-bacteriostatic sterile water, the infusion solution should be used as soon as possible. If not used immediately in-use storage times and conditions prior to use are the responsibility of the user and should not be longer than 24 hours at 2°C to 8°C.
Disposal of unused/expired medicines: The release of pharmaceuticals in the environment should be minimized.
Medicines should not be disposed of via wastewater and disposal through household waste should be avoided.
The following points should be strictly adhered to regarding the use and disposal of syringes and other medicinal sharps: Needles and syringes should never be reused.
Place all used needles and syringes into a sharps container (puncture-proof disposable container).
Dispose of the full container and of the administration system according to local requirements.
Do not store above 30°C.
Shelf-life: 3 years.
Shelf-life and storage of the reconstituted solution: For immediate use after reconstitution.
Shelf-life and storage of the infusion solution: Chemical and physical in-use stability of the infusion solution has been demonstrated for 24 hours at 2-8°C. Do not freeze (see Special Instructions for Use, Handling and Disposal under Cautions for Usage).
J05AB06 - ganciclovir ; Belongs to the class of nucleosides and nucleotides excluding reverse transcriptase inhibitors. Used in the systemic treatment of viral infections.
Cymevene infusion conc 500 mg
1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image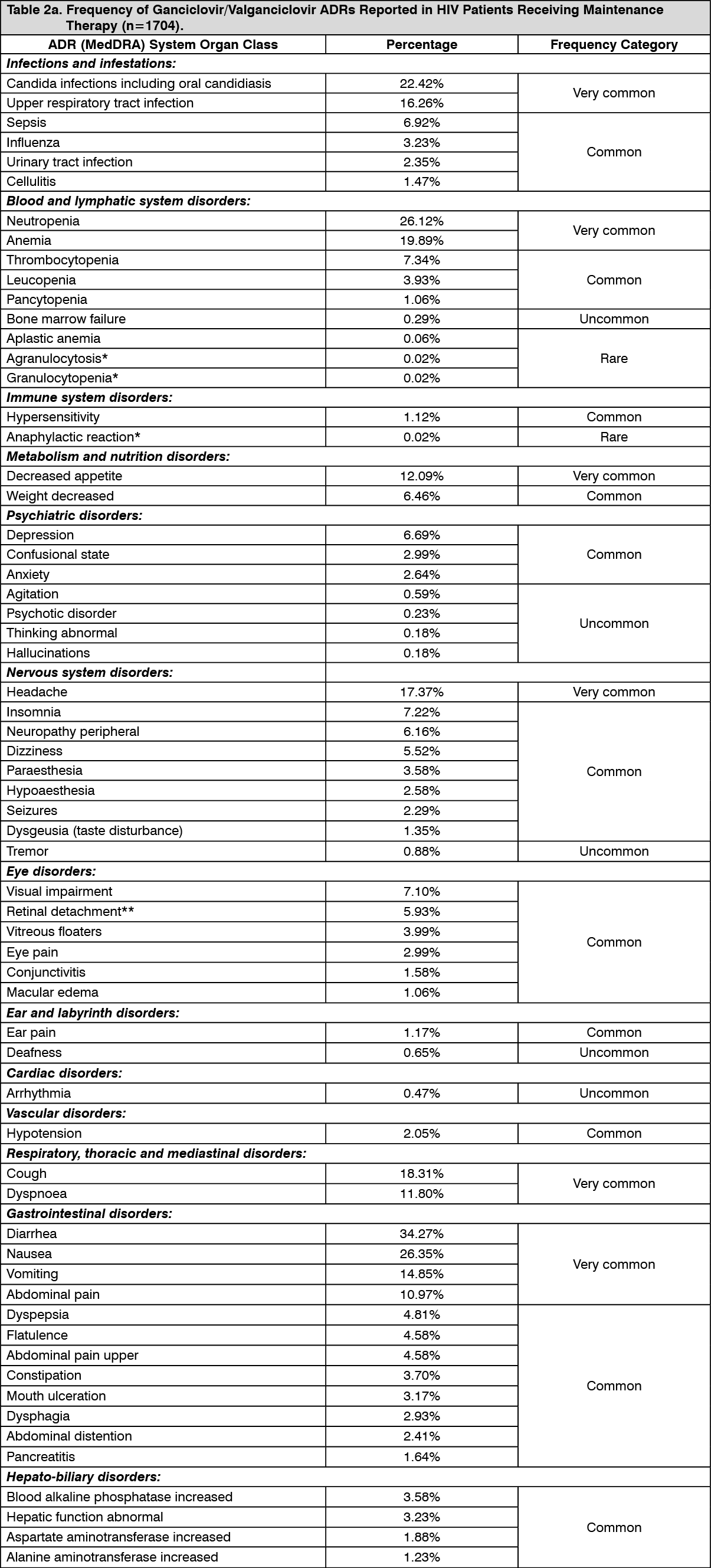 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image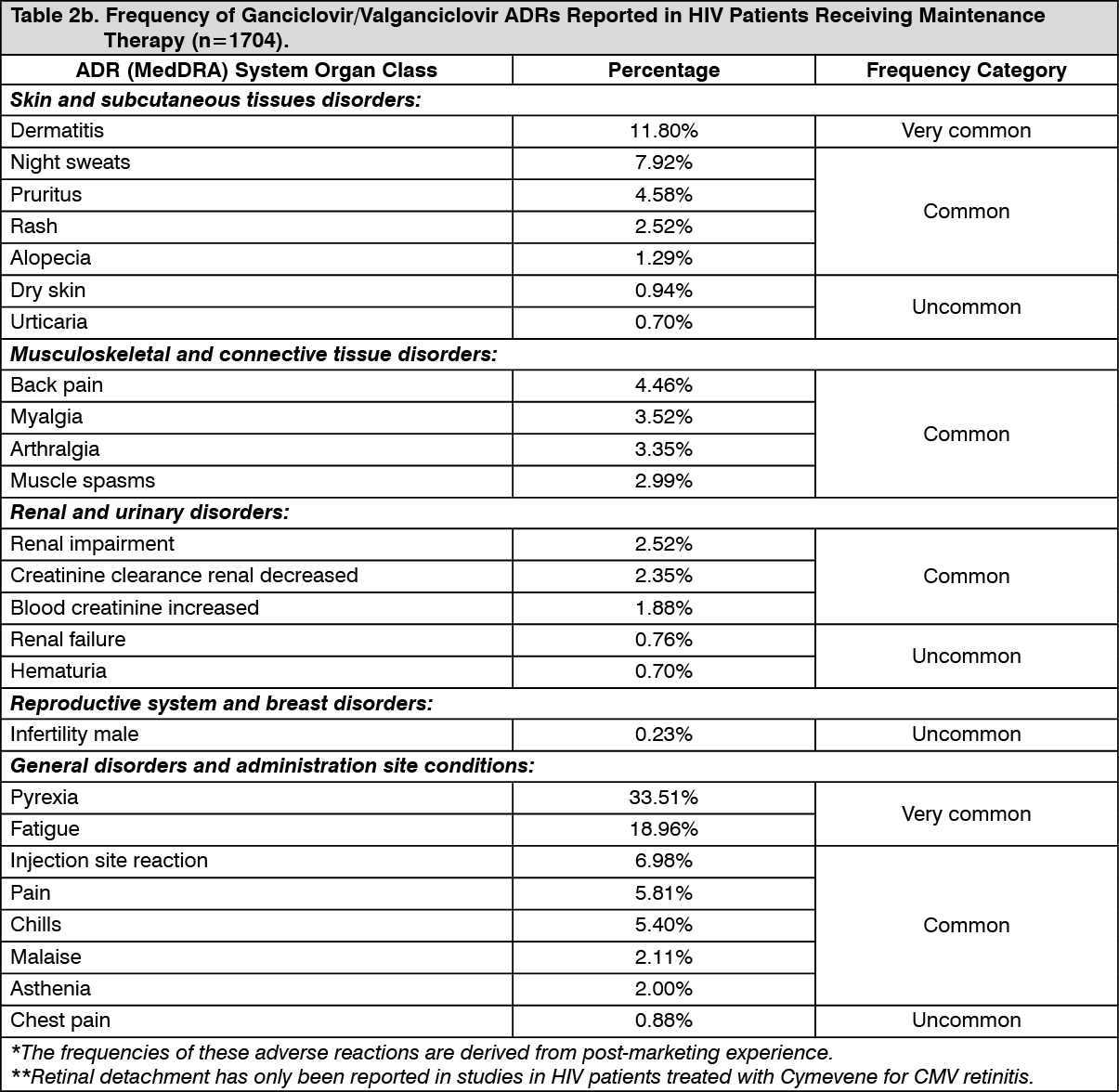 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image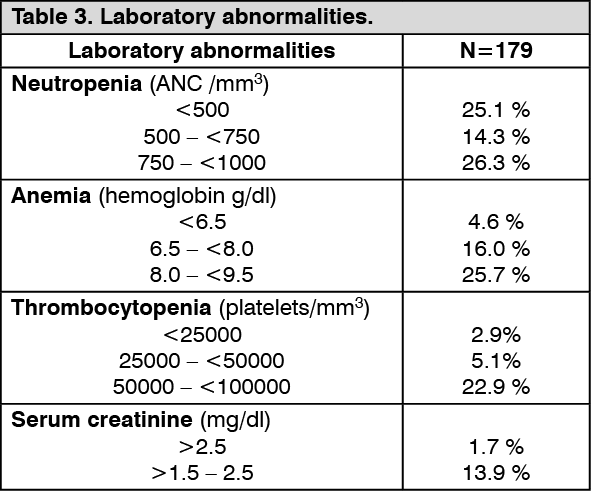 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
