


 Sign Out
Sign Out

Tabulated summary of adverse reactions: The table gives the adverse reactions observed from spontaneous reporting and in placebo-controlled clinical trials.
Table: Adverse reactions: Frequency estimate: Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to<1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000).
Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. (See Table A and Table B.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image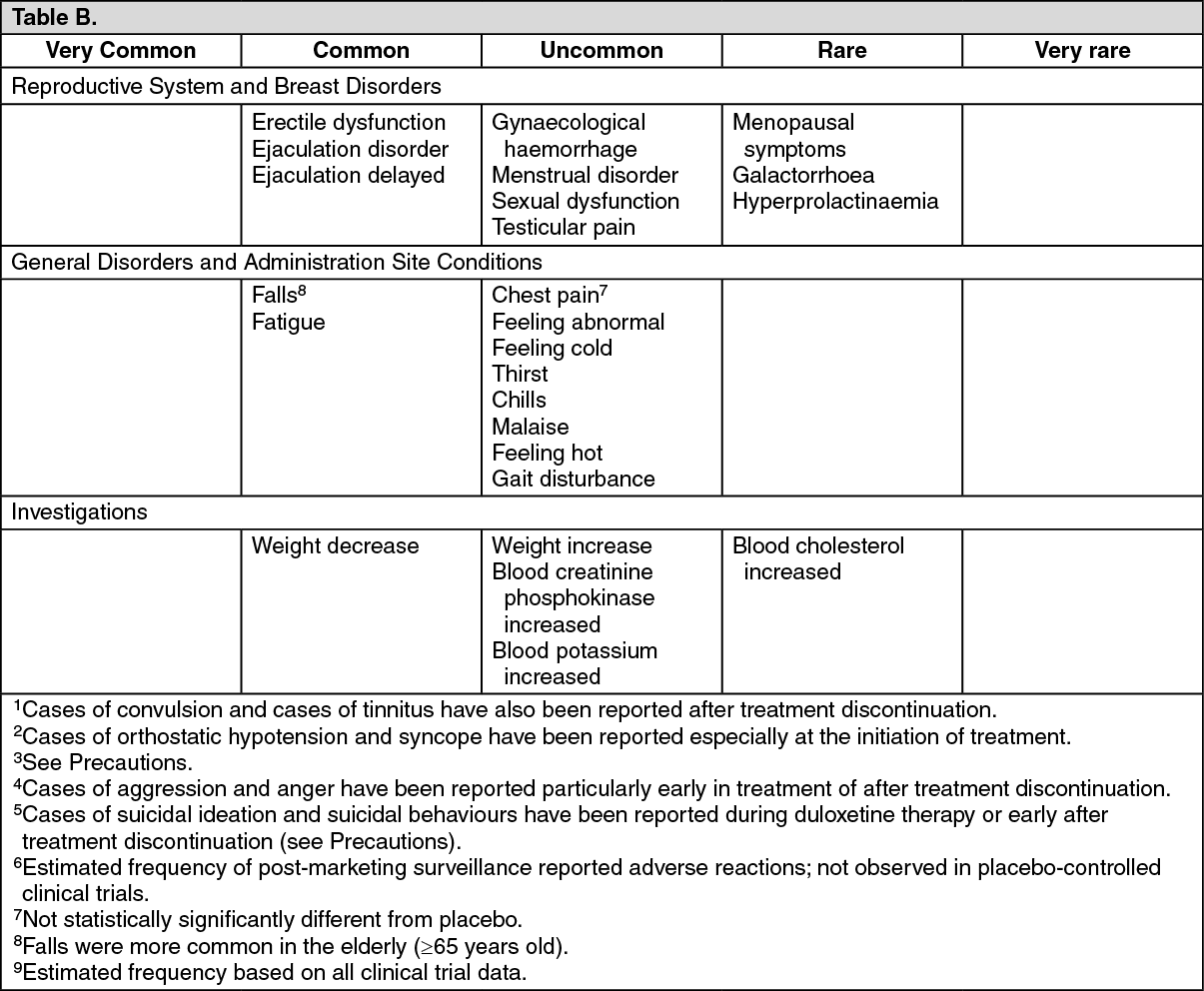 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Discontinuation of duloxetine (particularly when abrupt) commonly leads to withdrawal symptoms.
Dizziness, sensory disturbances (including paraesthesia or electric shock-like sensations, particularly in the head), sleep disturbances (including insomnia and intense dreams), fatigue, somnolence, agitation or anxiety, nausea and/or vomiting, tremor, headache, myalgia, irritability, diarrhoea, hyperhydrosis and vertigo are the most commonly reported reactions.
Generally, for SSRIs and SNRIs, these events are mild to moderate and self-limiting, however, in some patients they may be severe and/or prolonged. It is therefore advised that when duloxetine treatment is no longer required, gradual discontinuation by dose tapering should be carried out (See Dosage & Administration and Precautions).
In the 12 week acute phase of three clinical trials of duloxetine in patients with diabetic neuropathic pain, small but statistically significant increases in fasting blood glucose were observed in duloxetine-treated patients. HbA1c was stable in both duloxetine-treated and placebo-treated patients. In the extension phase of these studies, which lasted up to 52 weeks, there was an increase in HbA1c in both the duloxetine and routine care groups, but the mean increase was 0.3% greater in the duloxetine-treated group. There was also a small increase in fasting blood glucose and in total cholesterol in duloxetine-treated patients while those laboratory tests showed a slight decrease in the routine care group.
The heart rate-corrected QT interval in duloxetine-treated patients did not differ from that seen in placebo-treated patients. No clinically significant differences were observed for QT, PR, QRS, or QTcB measurements between duloxetine-treated and placebo-treated patients.
Paediatric population: A total of 509 paediatric patients aged 7 to 17 years with MDD were treated with duloxetine in clinical trials. In general, the adverse reaction profile of duloxetine in children and adolescents was similar to that seen for adults.
A total of 467 paediatric patients initially randomized to duloxetine in clinical trials experienced a 0.1 kg mean decrease in weight at 10-weeks compared with a 0.9 kg mean increase in 353 placebo-treated patients. Subsequently, over the four-to six-month extension period, patients on average trended toward recovery to their expected baseline weight percentile based on population data from age- and gender- matched peers.
In studies of up to 9 months an overall mean decrease of 1% in height percentile (decrease of 2% in children (7-11 years) and increase of 0.3% in adolescents (12-17 years)) was observed in duloxetine-treated paediatric patients (see Precautions).
View ADR Monitoring Form