


 Sign Out
Sign Out


Pharmacology: Pharmacokinetics: General Characteristics: Daptomycin pharmacokinetics were generally linear (dose-proportional) and time-independent at CUBICIN doses of 4 to 12 mg/kg administered by IV infusion over a 30-minute period as a single daily dose for up to 14 days in adults. Steady-state concentrations were achieved by the third daily dose.
Distribution: Daptomycin is reversibly bound to human plasma proteins (mean binding range of 90 to 93%) in a concentration-independent manner, and serum protein binding trended lower (mean binding range of 84 to 88%) in adult subjects with significant renal impairment (CLCR <30 mL/min or on dialysis). The protein binding of daptomycin in adult subjects with mild to moderate hepatic impairment (Child-Pugh Class B) was similar to that in healthy adult subjects.
The volume of distribution at steady-state of daptomycin in healthy adult subjects was approximately 0.1 L/kg and was independent of dose. Tissue distribution studies in rats showed that daptomycin appears to penetrate the blood-brain barrier and the placental barrier only minimally following single and multiple doses.
Metabolism: In in vitro studies, daptomycin was not metabolized by human liver microsomes. In vitro studies with human hepatocytes indicate that daptomycin does not inhibit or induce the activities of the following human cytochrome P450 isoforms: 1A2, 2A6, 2C9, 2C19, 2D6, 2E1, and 3A4. It is unlikely that daptomycin will inhibit or induce the metabolism of drugs metabolized by the P450 system.
After infusion of 14C-daptomycin in healthy adults, the plasma radioactivity was similar to the concentration determined by microbiological assay. Inactive metabolites were detected in urine, as determined by the difference between total radioactive concentrations and microbiologically active concentrations. In a separate study, no metabolites were observed in plasma, and minor amounts of three oxidative metabolites and one unidentified compound were detected in urine. The site of metabolism has not been identified.
Elimination: Daptomycin is excreted primarily by the kidneys. There is minimal to no active tubular secretion of daptomycin. In a mass balance study of adult subjects using radiolabeled daptomycin, 78% of the administered dose was recovered from the urine based on total radioactivity, while urinary recovery of unchanged daptomycin was approximately 52% of the dose. About 6% of the administered dose was excreted in the feces based on total radioactivity. Plasma clearance of daptomycin is approximately 7 to 9 mL/h/kg, and its renal clearance is 4 to 7 mL/h/kg.
Specific Populations: Elderly: The pharmacokinetics of daptomycin were evaluated in 12 healthy elderly subjects (≥75 years of age) and 11 healthy young adult controls (18 to 30 years of age). Following administration of a single 4 mg/kg dose of CUBICIN by IV infusion over a 30-minute period, the mean total clearance of daptomycin was approximately 35% lower and the mean AUC was approximately 58% higher in elderly subjects than in healthy young adult subjects. There were no differences in Cmax.
Renal Impairment: Following administration of a single 4 mg/kg or 6 mg/kg dose of CUBICIN by IV infusion over a 30-minute period to adult subjects with various degrees of renal impairment, total daptomycin clearance was lower and systemic exposure (AUC) was higher than in subjects with normal renal function. The mean AUC for patients with CLCR <30 mL/min and for patients on dialysis (CAPD and hemodialysis dosed post-dialysis) was approximately 2 and 3 times higher, respectively, than for patients with normal renal function.
Hepatic Impairment: The pharmacokinetics of daptomycin were evaluated in 10 adult subjects with moderate hepatic impairment (Child-Pugh Class B) and compared with those in healthy adult volunteers (N=9) matched for gender, age, and weight. The pharmacokinetics of daptomycin were not altered in subjects with moderate hepatic impairment. The pharmacokinetics of daptomycin in patients with severe hepatic impairment (Child-Pugh Class C) have not been evaluated.
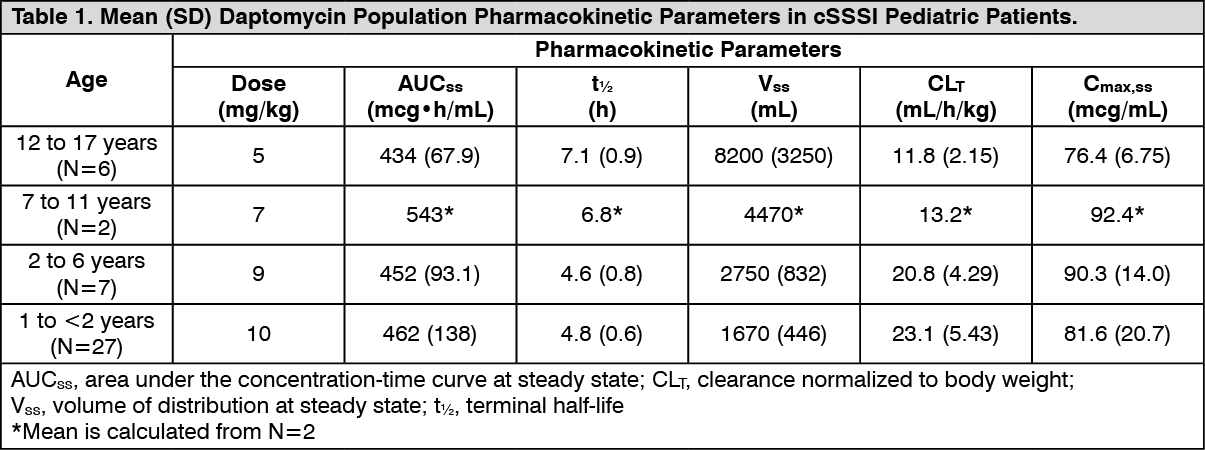
Pediatric: The pharmacokinetics of daptomycin in pediatric subjects was evaluated in 3 single-dose pharmacokinetic studies. In general, body weight-normalized total body clearance in pediatric patients was higher than in adults and increased with a decrease of age, whereas elimination half-life tends to decrease with a decrease of age. Body weight-normalized total body clearance and elimination half-life of daptomycin in children 2 to 6 years of age were similar at different doses.
A study was conducted to assess safety, efficacy, and pharmacokinetics of daptomycin in pediatric patients (1 to 17 years old, inclusive) with cSSSI caused by Gram-positive pathogens. Patients were enrolled into 4 age groups, and intravenous CUBICIN doses of 5 to 10 mg/kg once daily were administered. Following administration of multiple doses, daptomycin exposure (AUCss and Cmax,ss) was similar across different age groups after dose adjustment based on body weight and age (Table 1). (See Table 1.)
 Click on icon to see table/diagram/image
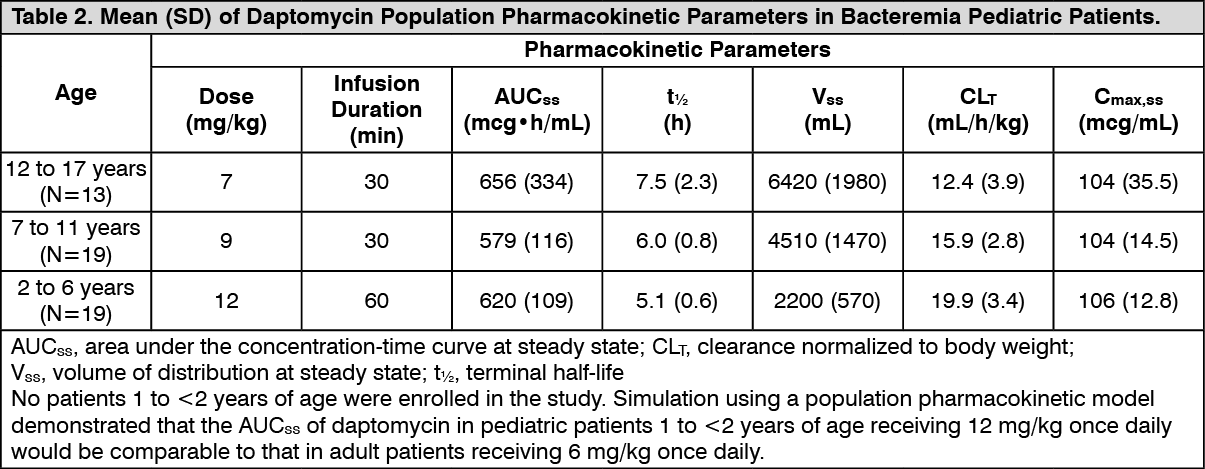
Click on icon to see table/diagram/imageA study was conducted to assess safety, efficacy, and pharmacokinetics of daptomycin in pediatric patients (1 to 17 years old, inclusive) with SAB. Patients were enrolled into 3 age groups and intravenous doses of 7 to 12 mg/kg once daily were administered. Following administration of multiple doses, daptomycin exposure (AUCss and Cmax,ss) was similar across different age groups after dose adjustment based on body weight and age (Table 2). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageGender: No clinically significant gender-related differences in daptomycin pharmacokinetics have been observed.
Obesity: The pharmacokinetics of daptomycin were evaluated in 6 moderately obese (Body Mass Index [BMI] 25 to 39.9 kg/m2) and 6 extremely obese (BMI ≥40 kg/m2) adult subjects. The AUC was approximately 30% higher in moderately obese subjects and 31% higher in extremely obese subjects than in nonobese controls.
Nonclinical Toxicology and Animal Pharmacology: In rats and dogs, daptomycin administration has been associated with effects on skeletal muscle. However, there were no changes in cardiac or smooth muscle. Skeletal muscle effects were characterized by microscopic degenerative/regenerative changes and variable elevations in CPK. No fibrosis or rhabdomyolysis was observed. All muscle effects, including microscopic changes, were fully reversible within 30 days following the cessation of dosing.
In adult rats and dogs, effects on peripheral nerve (characterized by axonal degeneration and frequently accompanied by functional changes) were observed at daptomycin doses higher than those associated with skeletal myopathy. Reversal of both the microscopic and functional effects was essentially complete within 6 months post-dose.
Target organs of daptomycin-related effects in 7-week-old juvenile dogs were skeletal muscle and nerve, the same target organs as in adult dogs. In juvenile dogs, nerve effects were noted at lower daptomycin blood concentrations than in adult dogs following 28 days of dosing. In contrast to adult dogs, juvenile dogs also showed evidence of effects in nerves of the spinal cord as well as peripheral nerves after 28 days of dosing. Following a 28-day recovery phase, microscopic examination revealed full recovery of the skeletal muscle and the ulnar nerve effects, and partial recovery of the sciatic nerve and spinal cord effects. No nerve effects were noted in juvenile dogs following 14 days of dosing.
Effects of daptomycin were assessed in neonatal dogs following once-daily IV administration for 28 consecutive days from postnatal days (PND) 4 through 31 at nominal dosage levels of 10 [no observed adverse effect level (NOAEL)], 25, 50, and 50/75 mg/kg/day.
At dose levels of 50 and 75 mg/kg/day with associated Cmax and AUCinf values of ≥321 μg/mL and ≥1470 μg·h/mL, respectively, marked clinical signs of twitching, muscle rigidity in the limbs, and impaired use of limbs were observed. Resulting decreases in body weights and overall body condition at doses ≥50 mg/kg/day necessitated early discontinuation by PND19. At the dose level of 25 mg/kg/day with associated Cmax and AUCinf values of 147 μg/mL and 717 μg·h/mL, respectively, mild clinical signs of twitching and one incidence of muscle rigidity were observed without any effects on body weight and were reversible over a 28-day recovery period. These data indicate a limited margin between doses associated with mild versus marked adverse clinical signs. Histopathological assessment did not reveal any daptomycin-related changes in the peripheral and central nervous system tissue, as well as in the skeletal muscle or other tissues assessed, at any dose level. No adverse clinical signs for these target organs of toxicity were observed in the dogs that received daptomycin at 10 mg/kg/day, the NOAEL, with associated Cmax and AUCinf values of 62 μg/mL and 247 μg·h/mL, respectively.
Carcinogenesis/Mutagenesis: Long-term carcinogenicity studies in animals have not been conducted. Daptomycin was not mutagenic or clastogenic in a battery of in vivo and in vitro genotoxicity tests.
Reproduction: Reproductive studies performed in rats revealed no effect of daptomycin on fertility or reproductive performance.
Microbiology: Daptomycin belongs to the cyclic lipopeptide class of antibacterials. Daptomycin is a natural product that has clinical utility in the treatment of infections caused by aerobic, Gram-positive bacteria. The in vitro spectrum of activity of daptomycin encompasses most clinically relevant Gram-positive pathogenic bacteria. Daptomycin retains potency against Gram-positive bacteria that are resistant to other antibacterials, including isolates resistant to methicillin, vancomycin, and linezolid.
Mechanism of Action: The mechanism of action of daptomycin is distinct from that of any other antibacterial. Daptomycin binds to bacterial cell membranes and causes a rapid depolarization of membrane potential. This loss of membrane potential causes inhibition of DNA, RNA, and protein synthesis, which results in bacterial cell death.
Mechanism of Resistance: The mechanism(s) of daptomycin resistance is not fully understood. There are no known transferable elements that confer resistance to daptomycin.
There is no cross-resistance due to resistance mechanisms that are specific for another class of antibacterials.
Emergent decreases in susceptibility have been observed in both S. aureus and enterococcal isolates following CUBICIN therapy.
PK/PD Relationship: Daptomycin exhibits rapid, concentration-dependent bactericidal activity against Gram-positive bacteria in vitro and in in vivo animal models.
Interactions with Other Antibacterials: In vitro studies have investigated daptomycin interactions with other antibacterials. Antagonism, as determined by kill curve studies, has not been observed. In vitro synergistic interactions of daptomycin with aminoglycosides, β-lactam antibacterials, and rifampin have been shown against some isolates of staphylococci (including some methicillin-resistant isolates) and enterococci (including some vancomycin-resistant isolates).