Ergotamine tartrate, caffeine.
Cafergot tablets contain 1 mg ergotamine tartrate and 100 mg caffeine.
Excipients/Inactive Ingredients: Tartaric acid; magnesium stearate; talc; maize starch, cellulose; iron oxide yellow (E 172).
Pharmacotherapeutic Group: Antimigraine preparations. ATC Code: N02CA52.
Pharmacology: Pharmacodynamics: Ergotamine has a tonic action on vascular smooth muscle and has a special affinity for arterial monoaminergic receptors (NA and HT), especially in the external carotid network.
Ergotamine may lead to vasoconstriction by stimulating alpha-adrenergic and 5-HT receptors. It has a moderate to elevated affinity for several sub-types of serotoninergic receptors, but its beneficial effect on migraine is mainly linked to its action as an agonist of 5-HT1B and 5-HT1D receptors.
Ergotamine aborts attacks of migraine with or without aura by its specific vasotonic action on distended extracranial arteries. Caffeine accelerates and increases the enteral absorption of egotamine.
Pharmacokinetics: Ergotamine: Absorption: Ergotamine is rapidly absorbed following oral administration. Maximum plasma concentrations are reached 1.5 to 2 hours after administration.
Studies with tritium-labelled ergotamine have shown that approximately 62% of the oral dose is absorbed via the gastrointestinal route. Maximum plasma concentrations are reached approximately 2 hours after ingestion.
Any potential increase in plasma caffeine concentrations due to an interaction with one or more other medicinal products may lead to a rise in ergotamine absorption. Caffeine is significantly metabolised by CYP1A2 and medicinal products that increase or reduce enzyme activity may affect the metabolic clearance of caffeine.
Distribution: Oral bioavailability is 62 ± 3%.
The medicinal product has a high level of tissue affinity.
Protein binding of ergotamine is 98%. The absolute bioavailability of the parent drug is approximately 2% following oral administration and approximately 5% following rectal administration.
Biotransformation: Ergotamine is significantly metabolised in the liver and is a substrate of the CYP3A4 enzyme system. It has been suggested that the therapeutic effects of the medicinal product are partially linked to the active metabolites.
Elimination: The parent drug and metabolites are excreted mainly in the bile. Plasma elimination takes place in two stages, with alpha and beta half-lives of 2.7 and 21 hours, respectively.
Elimination in the urine is low (4.3 ± 0.4%). The drug is primarily eliminated via the biliary and faecal routes.
The addition of caffeine speeds up excretion into the blood and increases gastric absorption by at least 44%.
Caffeine: Absorption: Following oral administration, caffeine is rapidly and almost completely absorbed via the gastrointestinal route, and the maximum concentrations reached after the oral administration of 175 mg are between 5 and 10 μg/ml. Maximum plasma concentrations are reached between 15 and 120 minutes after administration.
Distribution: Plasma protein binding of caffeine is 35%. Tissue distribution of caffeine in the body is relatively uniform, including in the cerebrospinal fluid, breast milk, saliva and sperm. The volume of distribution is approximately 0.7 l/kg. Caffeine crosses the placental barrier.
Biotransformation: Caffeine is mostly metabolised by CYP1A2 into paraxanthine. Paraxanthine is metabolised in turn into uracil and uric acid derivatives by demethylation and hydroxylation. The plasma elimination half-life is approximately 3.5 hours.
Elimination: Metabolites are predominantly excreted in the urine. Caffeine clearance is increased by smoking.
Acute attacks of migraine (classical migraine) and related types of vascular headache.
Cafergot should be given at the first symptoms of an attack.
Adults: The first time Cafergot is taken, an initial dose of 2 Cafergot tablets orally is recommended. If relief is not obtained within half an hour, a further tablet should be administered; this may be repeated at half-hourly intervals, but the maximum daily dose indicated below should not be exceeded. For subsequent attacks the initial dose may be increased to 3 tablets, depending on the total dose required in previous attacks. If pain persists, additional doses of 1 tablet may be taken at half-hourly intervals up to the maximum dose (see as follows).
The following restriction must be observed: If supplementary antimigraine medication is required, the use of any ergotamine-containing preparations, intranasal or parenteral dihydroergotamine or sumatriptan or other 5HT1-receptor agonists must be avoided (see CONTRAINDICATIONS).
Maximum dose per attack or per day: Adults: 6 mg ergotamine tartrate = 6 tablets.
Maximum weekly dose: Adults: 10 mg ergotamine tartrate = 10 tablets.
Ergotism is defined as intense arterial vasoconstriction that produces signs and symptoms of ischaemia in the extremities or other tissues (such as renal or cerebral vasospasms). Gangrene is possible if it is not treated. Most cases of ergotism are related to chronic intoxication and/or overdose and/or an interaction.
Symptoms: Abdominal pain, confusion, light-headedness, nausea, vomiting, headache, tachycardia or bradycardia associated with hypotension, respiratory disorders, dizziness, paresthesia, ischaemia, gangrene, seizure, shock, coma, as well as symptoms of vascular ischaemia, such as numbness, tingling, pain in the extremities, cyanosis and absence of pulse. In rare cases, patients may present myocardial infarction.
Treatment: In the case of orally ingested drug, administration of activated charcoal is recommended. In the case of very recent oral intake gastric lavage may be considered.
Treatment should be symptomatic. In the event of severe vasospastic reactions, intravenous administration of a peripheral vasodilator such as nitroprusside, phentolamine or dihydralazine, local application of warmth to the affected area and nursing care to prevent tissue damage are recommended. In the event of coronary constriction, appropriate treatment such as nitroglycerin should be initiated.
Known hypersensitivity to ergot alkaloids, caffeine, or any other components of the formulations (see DESCRIPTION).
Pregnancy and breast-feeding (see Use in PREGNANCY AND LACTATION).
Impaired peripheral circulation, obliterative vascular disease, coronary heart disease, inadequately controlled hypertension, septic conditions, shock.
Severe renal or hepatic impairment.
Temporal arteritis.
Hemiplegic or basilar migraine.
Severe renal or hepatic impairment.
Concomitant treatment with macrolide antibiotics, HIV protease or reverse transcriptase inhibitors, azole antifungals (see INTERACTIONS).
Concomitant treatment with vasoconstrictor agents (including ergot alkaloids, sumatriptan and other 5HT1 receptor agonists) (see INTERACTIONS).
Cafergot is not recommended in patients aged under 12 years or over 65 years.
Cafergot is only indicated for the treatment of acute migraine attacks and not for prevention.
Continued daily use of Cafergot or it's use in excess of the recommended doses must be avoided since it may cause vasospasm.
If contrary to recommendations (see PRECAUTIONS) ergotamine-containing drugs including Cafergot are used excessively over years, they may induce fibrotic changes, in particular of the pleura and the retroperitoneum. There have also been rare reports of fibrotic changes of the cardiac valves.
Treated patients must be informed of the maximum dose that should not be exceeded and of the initial symptoms of overdose: ischaemic and trophic episodes in the extremities: onset of paresthesia (numbness, tingling), pain or vasoconstriction, even at the usual doses, must be investigated, nausea and vomiting not related to the migraine, symptoms of myocardial ischaemia (precordialgia).
As soon as the symptoms of overdose appear, treatment should be discontinued and the patient should consult his or her doctor as soon as possible.
Long-term or excessive use is contraindicated as it may lead to: fibrosis (especially pleural or retroperitoneal). Rare cases of cardiac valve fibrosis have been reported.
Ergotism including severe symptoms of peripheral blood vessel vasoconstriction, which may be potentially fatal.
Patients suffering from mild to moderate liver failure, especially those with hepatic cholestasis, must receive suitable follow-up.
The excessive use of antimigraine treatment may lead to the onset of chronic daily headaches, requiring the temporary withdrawal of treatment.
Athletes' attention must be drawn to the fact that this medicinal product contains ergotamine, which is included in the list of doping substances.
The concomitant administration of this medicinal product and dopaminergic ergot alkaloids, alpha sympathomimetics (oral and/or nasal route), indirect sympathomimetics, crizotinib, idelalisib or enoxacin is inadvisable (see Interactions).
Effects on ability to drive and use machines: Patients experiencing dizziness should not drive or operate machinery.
Pregnancy: In animal studies, testing revealed a teratogenic effect with ergotamine tartrate. These effects can be attributed to a reduction in the utero-placental blood flow (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Data concerning the use of ergotamine tartrate during pregnancy are limited.
In addition, this product has vasoconstrictive and oxytocic properties. Consequently, Cafergot should not be used during pregnancy.
Breast-feeding: Ergot derivatives are excreted into breast milk, and therefore breast-feeding is contraindicated during treatment with this medicinal product. Ergotamine and caffeine are excreted into breast milk. Ergotamine may lead to symptoms such as vomiting, diarrhoea, weak pulse and irregular blood pressure in neonates. Cafergot is therefore contraindicated in breast-feeding mothers.
Fertility: In male rats receiving oral ergotamine and caffeine as combination therapy (1:100), fertility is not affected (see Pharmacology: Toxicology: Preclinical safety data under Actions).
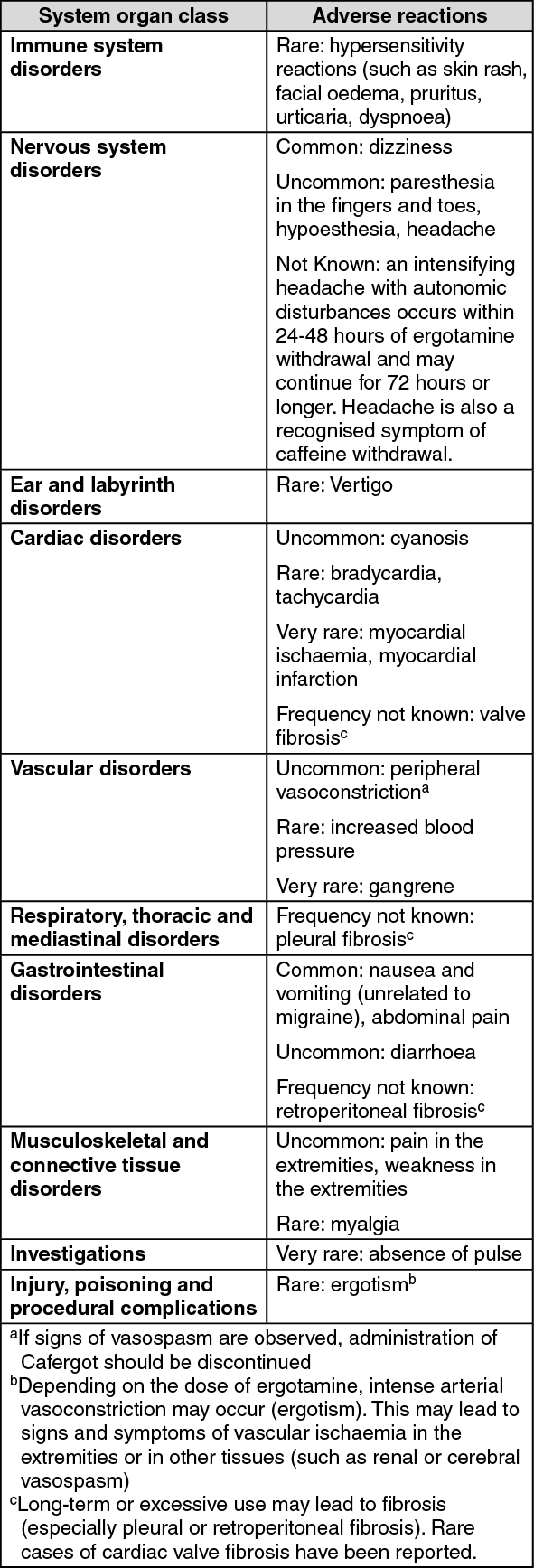
The most common undesirable effects are nausea and vomiting. The following undesirable effects have been determined based on clinical trials and post-marketing experience with Cafergot.
The frequencies in the table as follows are given as an indication, based on the following categories; very common (≥ 1/10); common (≥ 1/100, < 1/10); uncommon (≥ 1/1,000, < 1/100); rare (≥ 1/10,000, < 1/1,000); very rare (< 1/10,000); frequency not known (cannot be estimated based on available data). Adverse reactions to this medicinal product are listed according to MedDRA system organ class. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Expected interactions leading to a contraindication: Potent inhibitors of CYP3A4: The concomitant use of cytochrome P450 3A (CYP3A) inhibitors such as macrolide antibiotics (e.g. troleandomycin, erythromycin, clarithromycin), HIV protease or reverse transcriptase inhibitors (e.g. ritonavir, indinavir, nelfinavir, delavirdine or azole antifungals (e.g. ketoconazole, itraconazole, voriconazole) and Cafergot must be avoided (see CONTRAINDICATIONS), since this can result in an elevated exposure to ergotamine and ergot toxicity (vasospasm and ischemia of the extremities and other tissues).
Vasoconstrictors: Ergot alkaloids have also been shown to be inhibitors of CYP3A. No pharmacokinetic interactions involving other cytochrome P450 isoenzymes are known.
A few cases of vasospastic reactions have been reported among patients treated concomitantly with ergotamine-containing preparations and propranolol.
Concurrent use of vasoconstrictor agents including preparations containing ergot alkaloids, sumatriptan and other 5HT1 receptor agonists, and nicotine (e.g. heavy smoking) must be avoided since this may result in enhanced vasoconstriction (see CONTRAINDICATIONS)
Interactions observed leading to non-recommendation of concomitant use: Any potential increase in plasma caffeine concentrations due to an interaction with one or more other medicinal products may lead to a rise in ergotamine absorption. Caffeine is significantly metabolised by CYP1A2 and medicinal products that increase or reduce enzyme activity may affect the metabolic clearance of caffeine. Fluoroquinolones, mexiletine, fluvoxamine and oral contraceptives may increase plasma exposure to caffeine. Interactions between sympathomimetics and caffeine can cause a rise in blood pressure.
Observed interactions to be taken into account: Beta-blockers: A few cases of vasospastic reactions have been reported in patients treated concomitantly with medicinal products containing ergotamine and propranolol.
Expected interactions to be taken into account: Moderate/weak CYP3A4 inhibitors: Moderate to weak CYP3A4 inhibitors such as cimetidine, clotrimazole, fluconazole, grapefruit juice, quinupristin/dalfopristin and zileuton may also increase exposure to ergotamine and caution is required if they are used concomitantly.
Serotonin reuptake inhibitors: The concurrent use of ergotamine and serotonin reuptake inhibitors (e.g. amitriptyline), including selective agents (e.g. sertraline), may cause serotonin syndrome and requires caution.
CYP3A4 inducers: CYP3A4-inducing medicinal products (e.g. nevirapine, rifampicin) can cause a reduction in the pharmacological activity of ergotamine.
Absence of interaction: No pharmacokinetic interactions involving other cytochrome P450 isoenzymes are known.
Interactions related to ergotamine: Contraindicated combinations: Triptans (almotriptan, fovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan, eletriptan): risk of hypertension, coronary artery vasoconstriction. An interval of 24 hours should be left between discontinuation of the triptan and administration of the alkaloid.
Macrolides (except spiramycin): ergotism, with the possibility of necrosis in the extremities (decrease in hepatic elimination of ergot alkaloids).
Protease inhibitors (e.g. amprenavir, atazanavir, fosamprenavir, indinavir, lopinavir, nelfinavir, ritonavir, saquinavir, tipranavir): ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Reverse transcriptase inhibitors (delavirdine, efavirenz): ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Voriconazole: ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Quinupristin-dalfopristin (in combination): ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Stiripentol: ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Diltiazem: ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid).
Phenylpropanolamine: risk of vasoconstriction and/or episodes of hypertension.
Triclabendazole: ergotism, with the possibility of necrosis in the extremities (inhibition of hepatic metabolism of the ergot alkaloid). An interval of 24 hours should be left between the discontinuation of treatment and ergotamine, and vice versa.
Inadvisable combinations: Dopaminergic ergot alkaloids (bromocriptine, cabergolin, pergolide, lisuride): risk of vasoconstriction and/or episodes of hypertension.
Alpha sympathomimetics (oral and/or nasal route) (etilephrine, midodrine, naphazoline, oxymetazoline, phenylephrine, synephrine, tetryzoline, tuaminoheptane, tymazoline): risk of vasoconstriction and/or episodes of hypertension.
Indirect sympathomimetics (except phenylpropanolamine) (ephedrine, phenylephrine, pseudoephedrine): risk of vasoconstriction and/or episodes of hypertension.
Combinations requiring precautions for use: Beta-blockers (propanolol, oxprenolol): ergotism; some cases of arterial spasm with ischaemia in the extremities have been observed (cumulative vascular effects). Increased clinical monitoring, especially during the first weeks of combination therapy.
Interactions related to caffeine: Inadvisable combinations: Enoxacin: increase in plasma caffeine concentrations, which may lead to excitation and hallucinations due to a decrease in hepatic metabolism. Combinations to be taken into account: Ciprofloxacin, norfloxacin: increase in plasma caffeine concentrations, which may lead to excitation and hallucinations due to a decrease in hepatic metabolism.
Mexiletine: increase in plasma caffeine concentrations due to the inhibition of its hepatic metabolism by mexiletine.
Incompatibilities: Not applicable.
Store below 25°C. Protect from light.
N02CA52 - ergotamine, combinations excl. psycholeptics ; Belongs to the class of ergot alkaloids preparations. Used to relieve migraine.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
