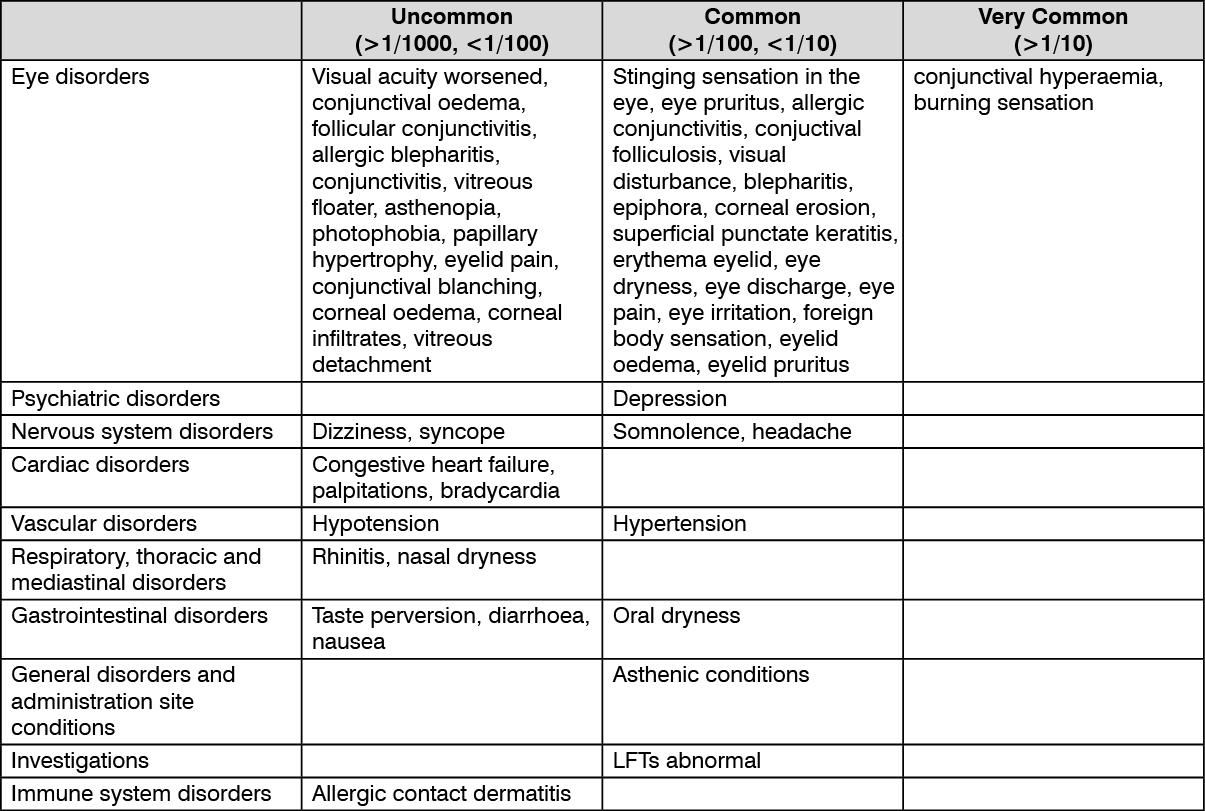
The most common ADRs were conjunctival hyperaemia and burning sensation in the eye. The majority of cases was mild. Adverse drug reactions reported: (See table.)
 Click on icon to see table/diagram/image
Additional Adverse Reactions:
Click on icon to see table/diagram/image
Additional Adverse Reactions: Additional adverse events that have been seen with one of the components and may potentially occur also with YSP BRIMOLOL EYE DROP:
Brimonidine: Eye disorders: blurring, ocular allergic reaction, corneal staining, conjunctival discharge, conjunctival papillae, iritis, iridiocyclitis (anterior uveitis), miosis.
Immune system disorders: hypersensitivity, skin reaction (including erythema, face oedema, pruritus, rash), vasodilation.
Psychiatric disorders: insomnia.
Cardiac disorders: arrhythmias, tachycardia.
Respiratory, thoracic and mediastinal disorders: upper respiratory symptoms.
Gastrointestinal disorders: gastrointestinal symptoms.
General disorders and administration site conditions: fatigue/drowsiness and systemic allergic reactions.
In cases where brimonidine has been used as part of the medical treatment of congenital glaucoma, symptoms of brimonidine overdose such as loss of consciousness, hypotension, hypotonia, bradycardia, hypothermia, cyanosis and apnoea have been reported in neonates and infants (less than 2 years of age) receiving brimonidine. A high incidence of somnolence has been reported in children 2 years of age and above, especially those in 2-7 age range and/or weighing <20 kg.
Timolol: Eye disorders: decreased corneal sensitivity, blepharoptosis, diplopia, keratitis, ptosis, choroidal detachment (following filtration surgery), refractive changes (due to withdrawal of miotic therapy in some cases), cystoid macular oedema, pseudopemphigoid.
Psychiatric disorders: insomnia, nightmares, decreased libido, behavioral changes and psychic distrubances including anxiety, confusion, disorientation, hallucinations, memory loss, nervousness.
Nervous system disorders: increase in signs and symptoms of myasthenia gravis, paresthesia, cerebral ischaemia, cerebral vascular accident, insomnia, nightmares. behavioural changes and psychic disturbances including confusion, hallucinations, anxiety, disorientation, nervousness, memory loss, fatigue and paraesthesia.
Ear and labyrinth disorders: tinnitus.
Cardiac disorders: heart block, cardiac arrest, arrhythmia, bradycardia, atrioventricular block, cardiac failure, chest pain, oedema, pulmonary oedema, worsening of angina pectoris.
Vascular disorders: syncope.
Respiratory, thoracic and mediastinal disorders: bronchospasm (predominantly in patients with pre-existing bronchospastic disease) dyspnoea, cough, respiratory failure, exacerbation of asthma, nasal congestion, upper respiratory infection.
Gastrointestinal disorders: dyspepsia, abdominal pain, anorexia, vomiting.
Skin and subcutaneous tissue disorders: alopecia, psoriasiform rash or exacerbation of psoriasis, skin rash.
Musculoskeletal, connective tissue and bone disorders: myalgia.
Renal and urinary disorders: Peyronie's disease, retroperitoneal fibrosis.
Immune system disorders: Signs and symptoms of systemic allergic reactions including angioedema, generalized and localized rash, pruritus, urticaria; Systemic lupus erythematosus.
Endocrine disorders: Masked symptoms of hypoglycaemia in diabetes patients.
Other: Decreased libido, sexual dysfunction.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
