Pharmacology: Pharmacodynamics: Mechanism of Action: B-Lymphocyte Stimulator (BLyS, also referred to as BAFF and TNFSF13), a member of the tumour necrosis factor (TNF) ligand family, inhibits B cell apoptosis and stimulates the differentiation of B cells into immunoglobulin-producing plasma cells. BLyS is overexpressed in patients with SLE, leading to elevated plasma BLyS levels. There is a strong association between SLE disease activity (as assessed by the Safety of Estrogen in Lupus Erythematosus National Assessment-Systemic Lupus Erythematosus Disease Activity Index [SELENA-SLEDAI]) and plasma BLyS levels.
Belimumab is a fully human IgG1λ monoclonal antibody that specifically binds to soluble human BLyS and inhibits its biological activity. Belimumab does not bind B cells directly, but by binding BLyS, belimumab inhibits the survival of B cells, including autoreactive B cells, and reduces the differentiation of B cells into immunoglobulin-producing plasma cells.
Pharmacodynamic Effect: In adult patients with SLE, reductions in elevated levels of serum IgG and in anti-dsDNA antibodies were observed as early as Week 8 and continued to Week 52. In patients with hypergammaglobulinaemia at baseline, normalisation of IgG levels was observed by week 52 in 49% and 20% of patients receiving belimumab and placebo, respectively. In patients with anti-dsDNA antibodies at baseline, reductions in patients receiving belimumab were evident as early as Week 8, and by Week 52, 16% of patients treated with belimumab had converted to anti-dsDNA negative compared with 7% of the patients receiving placebo.
In patients with SLE with low complement levels at baseline, belimumab treatment resulted in increases in complement C3 and C4 which were seen as early as Week 4 and continued over time. By Week 52, levels of C3 and C4 had normalised in 38% and 44% of patients receiving belimumab compared with 17% and 19% of patients receiving placebo.
The target of belimumab, BLyS, is a critical cytokine for B cell survival, differentiation, and proliferation. Belimumab significantly reduced circulating B cells, naive, activated, plasma, and the SLE B cell subset at Week 52. Reductions in naive, plasma and short-lived plasma cells as well as the SLE B cell subset were observed as early as Week 8. Memory cells increased initially and slowly declined toward baseline levels by Week 52.
In a long-term uncontrolled extension study, B cells (including naive, activated, plasma cells and the SLE B cell subset) and IgG levels were followed for more than 7 years with ongoing treatment. A substantial and sustained decrease in various B cell subsets was observed leading to median reductions of 87% in naive B cells, 67% in memory B cells, 99% in activated B cells, and 92% in plasma cells after more than 7 years of treatment. After about 7 years, a 28% median reduction in IgG levels was observed with 1.6% of subjects experiencing a decrease in IgG levels to below 400 mg/dL. Over the course of the study, the reported incidence of AEs generally remained stable or declined.
In patients with active lupus nephritis, following treatment with belimumab or placebo, there was an increase in serum IgG levels which was associated with decreased proteinuria. Relative to placebo, smaller increases in serum IgG levels were observed in the belimumab group as expected with the known mechanism of belimumab. At Week 104, the median percent increase from baseline in IgG was 17% for belimumab and 37% for placebo. Reductions in autoantibodies, increases in complement, and reductions in circulating total B cells and B-cell subsets observed were consistent with the SLE studies.
Immunogenicity: In the two Phase III SLE studies with BENLYSTA administered intravenously in adult patients, 4 out of 563 (0.7%) patients in the 10 mg/kg group and 27 out of 559 (4.8%) patients in the 1 mg/kg group developed persistent anti-belimumab antibodies. The reported frequency for the 10 mg/kg group may underestimate the actual frequency due to lower assay sensitivity in the presence of high drug concentrations. Neutralising antibodies were detected in three patients receiving belimumab 1 mg/kg.
In a Phase III/IV study with BENLYSTA 10 mg/kg administered intravenously to black patients, two of the 321 (0.6%) patients developed anti-belimumab antibodies.
In a Phase III study with BENLYSTA 10 mg/kg administered intravenously to adult patients with active lupus nephritis, none of the 224 patients developed anti-belimumab antibodies.
The presence of anti-belimumab antibodies was relatively uncommon and no definitive conclusions can be drawn regarding the effect of immunogenicity on belimumab pharmacokinetics due to low numbers of anti-belimumab antibody-positive subjects.
Clinical Studies: SLE: The efficacy of BENLYSTA was evaluated in two randomised, double-blind, placebo-controlled Phase III studies in 1,684 patients with a clinical diagnosis of SLE according to the American College of Rheumatology (ACR) classification criteria. Eligible patients had active SLE disease, defined as a SELENA-SLEDAI score greater than or equal to 6 and positive anti-nuclear antibody (ANA or anti-dsDNA) test results (ANA titre greater than or equal to 1:80 and/or a positive anti-dsDNA [greater than or equal to 30 units/mL]) at screening. Patients were on a stable SLE treatment regimen (standard of care) consisting of any of the following (alone or in combination): corticosteroids, anti-malarials, NSAIDs or other immunosuppressives. Patients were excluded from the study if they had severe active central nervous system lupus or severe active lupus nephritis, had ever received treatment with any B cell targeted therapy, if they had received another biological investigational agent in the previous year, or if they had a positive response to testing for HIV antibody, hepatitis B surface antigen, or hepatitis C antibody. The two studies were similar in design except that Study 1 was a 76-week study and Study 2 was a 52-week study. Both studies had 52-week primary endpoints.
Study 1 (HGS1006-C1056) was conducted primarily in North America and Western Europe. The racial distribution was 70% white/Caucasian, 14% black/African American, 13% Alaska native or American Indian, and 3% Asian. Background medications included corticosteroids (76%), immunosuppressives (56%), and anti-malarials (63%).
Study 2 (HGS1006-C1057) was conducted in South America, Eastern Europe, Asia, and Australia. The racial distribution was 38% Asian, 26% white/Caucasian, 32% Alaska native or American Indian, and 4% black/African American. Background medications included corticosteroids (96%), immunosuppressives (42%), and anti-malarials (67%).
Patient median age across both studies was 37 years (range: 18 to 73 years), and the majority (94%) were female. At screening, patients were stratified by disease severity based on their SELENA-SLEDAI score (less than or equal to 9 vs greater than or equal to 10), proteinuria level (less than 2 g per 24 hr vs greater than or equal to 2 g per 24 hr), and race, and then randomly assigned to receive BENLYSTA 1 mg/kg, BENLYSTA 10 mg/kg, or placebo in addition to standard of care. The patients were administered study medication intravenously over a 1-hour period on Days 0, 14, 28, and then every 28 days for 48 or 72 weeks.
The primary efficacy endpoint was a composite endpoint (SLE Responder Index) that defined response as meeting each of the following criteria at Week 52 compared with baseline: greater than or equal to 4-point reduction in the SELENA-SLEDAI score, and no new British Isles Lupus Assessment Group (BILAG) A organ domain score or two new BILAG B organ domain scores, and no worsening (less than 0.30 point increase) in Physician's Global Assessment score (PGA).
The SLE Responder Index uses the SELENA-SLEDAI score as an objective measure of reduction in global disease activity; the BILAG index to ensure no significant worsening in any specific organ system; and the PGA to ensure that improvements in disease activity are not achieved at the expense of the patient's overall condition.
BENLYSTA produced significant improvements in the SLE Responder Index as well as in the individual component SELENA-SLEDAI score in both studies, (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a pooled analysis of the two studies, the percentage of patients receiving greater than 7.5 mg/day prednisone (or equivalent) at baseline whose average corticosteroid dose was reduced by at least 25% from baseline to a dose equivalent to prednisone less than or equal to 7.5 mg/day during Weeks 40 through 52, was 17.9% in the group receiving belimumab and 12.3% in the group receiving placebo (P=0.0451).
Flares in SLE were defined by the Modified SELENA-SLEDAI SLE Flare Index where the modification excludes severe flares that are triggered only by an increase of SELENA-SLEDAI score to greater than 12. The median time to the first flare was delayed in the pooled group receiving belimumab compared to the group receiving placebo (hazard ratio=0.84, P=0.012). The risk of severe flares was also reduced by 36% over the 52 weeks of observation in the group receiving belimumab compared to the group receiving placebo (hazard ratio=0.64, P=0.0011).
Univariate and multivariate analysis of the primary endpoint demonstrated that the greatest benefit was observed in patients with higher disease activity including patients with SELENA-SLEDAI scores greater than or equal to 10, patients requiring steroids to control their disease, and patients with low complement levels.
Post-hoc analysis identified a high responding subgroup as those patients with low complement and positive anti-dsDNA at baseline, see Table 2 or results of this example of a higher disease activity group. Of these patients, 64.5% had SELENA-SLEDAI scores greater than or equal to 10 at baseline. (See Table 2.)
Click on icon to see table/diagram/image
Lupus Nephritis: The efficacy and safety of Benlysta 10 mg/kg administered intravenously over a 1-hour period on Days 0, 14, 28, and then every 28 days, were evaluated in a 104-week randomised (1:1), double-blind, placebo-controlled, Phase III study (BEL114054) in 448 patients with active lupus nephritis. The patients had a clinical diagnosis of SLE according to ACR classification criteria, biopsy proven lupus nephritis Class III, IV, and/or V and had active renal disease at screening requiring standard therapy. Standard therapy included corticosteroids, 0 to 3 intravenous administrations of methylprednisolone (500 to 1000 mg per administration), followed by oral prednisone 0.5 to 1 mg/kg/day with a total daily dose ≤60 mg/day and tapered to ≤10 mg/day by Week 24, with: mycophenolate mofetil 1 to 3 g/day orally or mycophenolate sodium 720 to 2160 mg/day orally for induction and maintenance, or cyclophosphamide 500 mg intravenously every 2 weeks for 6 infusions for induction followed by azathioprine orally at a target dose of 2 mg/kg/day for maintenance.
This study was conducted in Asia, North America, South America, and Europe. Patient median age was 31 years (range: 18 to 77 years); the majority (88%) were female.
The primary efficacy endpoint was Primary Efficacy Renal Response (PERR) at Week 104 defined as a response at Week 100 confirmed by a repeat measurement at Week 104 of the following parameters: urinary protein: creatinine ratio (uPCR) ≤700 mg/g (79.5 mg/mmol) and estimated glomerular filtration rate (eGFR) ≥60 mL/min/1.73 m
2 or no decrease in eGFR of >20% from pre-flare value.
The major secondary endpoints included: Complete Renal Response (CRR) defined as a response at Week 100 confirmed by a repeat measurement at Week 104 of the following parameters: uPCR <500 mg/g (56.8 mg/mmol) and eGFR ≥90 mL/min/1.73 m
2 or no decrease in eGFR of >10% from pre-flare value; PERR at Week 52; Time to renal-related event or death (renal-related event defined as first event of end-stage renal disease, doubling of serum creatinine, renal worsening [defined as increased proteinuria, and/or impaired renal function], or receipt of renal disease-related prohibited therapy).
For PERR and CRR endpoints, steroid treatment had to be reduced to ≤10 mg/day from Week 24 to be considered a responder. For these endpoints, patients who discontinued treatment early, received prohibited medication, or withdrew from the study early were considered non-responders.
The proportion of patients achieving PERR at Week 104 was significantly higher in patients receiving Benlysta compared with placebo. The major secondary endpoints also showed significant improvement with Benlysta compared with placebo (Table 3). (See Table 3.)
Click on icon to see table/diagram/image
A numerically greater percentage of patients receiving Benlysta achieved PERR beginning at Week 24 compared with placebo, and this treatment difference was maintained through to Week 104. Beginning at Week 12, a numerically greater percentage of patients receiving Benlysta achieved CRR compared with placebo and the numerical difference was maintained through to Week 104 (Figure 1). (See Figure 1.)
Click on icon to see table/diagram/image
In descriptive subgroup analyses, key efficacy endpoints (PERR and CRR) were examined by induction regimen (mycophenolate or cyclophosphamide) and biopsy class (Class III or IV, Class III + V or Class IV + V, or Class V) (Figure 2). (See Figure 2.)
Click on icon to see table/diagram/image
Black patients: BENLYSTA was administered intravenously to black patients in a randomised (2:1), double-blind, placebo-controlled 52-week Phase III/IV study (BEL115471). Efficacy was evaluated in 448 patients. The study design was the same as the pivotal studies summarised above apart from: eligible patients had a SELENA-SLEDAI score ≥8 and the primary endpoint was the SRI response at Week 52 with modified SLEDAI-2K scoring for proteinuria (SRI-S2K). The study was conducted in North America, South America, Europe and Africa. Patient median age was 38 years (range: 18 to 71 years), and the majority of patients (97%) were female.
The proportion of black patients achieving an SRI-S2K response was higher in patients receiving BENLYSTA but the difference was not statistically significant compared with placebo. The trends in comparisons between the treatment groups for the rates of response for the individual components of the endpoint were generally consistent with that of the SRI-S2K (Table 4). (See Table 4.)
Click on icon to see table/diagram/image
The safety profile of BENLYSTA in black patients (n=331) was consistent with the known safety profile of BENLYSTA in the overall population.
Consistent with results from other studies, in patients with high disease activity (low complement and positive anti-dsDNA at baseline, n=141) the SRI-S2K response was 45.1% for BENLYSTA 10 mg/kg compared with 24.0% for placebo (odds ratio 3.00; 95% CI: 1.35, 6.68). These results suggest a greater relative response to BENLYSTA compared to placebo in black patients with high disease activity.
Other special patient groups: There were too few males, patients over 65 years of age enrolled in the controlled clinical trials to draw meaningful conclusions about the effects of gender, age, or race on clinical outcomes.
Pharmacokinetics: SLE studies: The pharmacokinetic parameters as follows are based on population parameter estimates which are specific to the 563 patients with SLE who received belimumab 10 mg/kg (Days 0, 14, 28, and then every 28 days up to 52 weeks) in the two Phase III studies in adults.
Absorption: Belimumab is administered by intravenous infusion. Maximum serum concentrations of belimumab were generally observed at, or shortly after, the end of the infusion. The maximum serum concentration was 313 micrograms/mL based on simulating the concentration time profile using the typical parameter values of the population pharmacokinetic model.
Distribution: Belimumab distributed to tissues with an overall volume of distribution of 5 L.
Metabolism: Belimumab is a protein for which the expected metabolic pathway is degradation to small peptides and individual amino acids by widely distributed proteolytic enzymes. Classical biotransformation studies have not been conducted.
Elimination: Serum belimumab concentrations declined in a bi-exponential manner, with a distribution half-life of 1.75 days and terminal half-life 19.4 days. The systemic clearance was 215 mL/day.
Lupus nephritis study: A population pharmacokinetic analysis was conducted in 224 adult patients with lupus nephritis who received BENLYSTA 10 mg/kg intravenously (Days 0, 14, 28, and then every 28 days up to 104 weeks). In patients with lupus nephritis, due to renal disease activity, belimumab clearance was initially higher than observed in SLE studies; however, after 24 weeks of treatment and throughout the remainder of the study, belimumab clearance and exposure were similar to that observed in adult patients with SLE who received BENLYSTA 10 mg/kg intravenously.
Transitioning from Intravenous to Subcutaneous Administration: SLE: Patients with SLE transitioning from 10 mg/kg intravenously every 4 weeks to 200 mg subcutaneously weekly using a 1 to 4 week switching interval had pre-dose belimumab serum concentrations at their first subcutaneous dose close to their eventual subcutaneous steady-state trough concentration (see Dosage & Administration). Based on simulations with population PK parameters the steady-state average belimumab concentrations for 200 mg subcutaneous every week were similar to 10 mg/kg intravenous every 4 weeks.
Lupus nephritis: One to 2 weeks after completing the first 2 intravenous doses, patients with lupus nephritis transitioning from 10 mg/kg intravenously to 200 mg subcutaneously weekly, are predicted to have average belimumab serum concentrations similar to patients dosed with 10 mg/kg intravenously every 4 weeks based on population PK simulations (see Dosage & Administration).
Drug interactions: Concomitant use of mycophenolate mofetil, cyclophosphamide, azathioprine, methotrexate and hydroxychloroquine did not substantially influence belimumab pharmacokinetics based on the results of the population pharmacokinetic analysis. Neither did a wide range of other co-medications (non-steroidal anti-inflammatory medications, aspirin, and HMG-CoA reductase inhibitors) significantly influence belimumab pharmacokinetics. Co-administration of steroids and ACE inhibitors resulted in a statistically significant increase of systemic clearance in the population pharmacokinetic analysis. However, these effects were not clinically meaningful as their magnitude was well within the range of normal variability of clearance.
Special Patient Groups: Elderly: Belimumab has been studied in a limited number of elderly patients. Within the overall SLE intravenous study population, age did not affect belimumab exposure in the population pharmacokinetic analysis. However, given the small number of subjects 65 years or older, an effect of age cannot be ruled out conclusively.
Children and adolescents: No pharmacokinetic data are available in paediatric patients.
Renal impairment: No formal studies were conducted to examine the effects of renal impairment on the pharmacokinetics of belimumab. During clinical development, belimumab was studied in a limited number of SLE patients with renal impairment (creatinine clearance less than 60 mL/min, including a small number with creatinine clearance less than 30 mL/min). Although proteinuria (greater than or equal to 2 g/day) increased belimumab clearance, and decreases in creatinine clearance decreased belimumab clearance, these effects were within the expected range of variability. Therefore, no dose adjustment is recommended for patients with renal impairment.
Hepatic impairment: No formal studies were conducted to examine the effects of hepatic impairment on the pharmacokinetics of belimumab. IgG1 molecules such as belimumab are catabolised by widely distributed proteolytic enzymes, which are not restricted to hepatic tissue; therefore, changes in hepatic function are unlikely to have any effect on the elimination of belimumab.
Other patient characteristics: There was no significant effect of gender, race or ethnicity on the pharmacokinetics of belimumab. The effects of body size on belimumab exposure are accounted for by weight normalised dosing.
Toxicology: Non-Clinical Information: Non-clinical data revealed no special hazard for humans based on studies of repeated dose toxicity and toxicity to reproduction.
Intravenous and subcutaneous administration to monkeys resulted in the expected reduction in number of peripheral and lymphoid tissue B-cell counts with no associated toxicological findings.
Reproductive studies have been performed in pregnant cynomolgus monkeys receiving belimumab 150 mg/kg by intravenous infusion (approximately nine times the anticipated maximum human clinical exposure) every two weeks for up to 21 weeks, and belimumab treatment was not associated with direct or indirect harmful effects with respect to maternal toxicity, developmental toxicity, or teratogenicity. Treatment-related findings were limited to the expected reversible reduction of B cells in both dams and infants and reversible reduction of IgM in infant monkeys. B cell numbers recovered after the cessation of belimumab treatment by about 1 year post-partum in adult monkeys and by three months of life in infant monkeys; IgM levels in infants exposed to belimumab in utero recovered by six months of age.
As belimumab is a monoclonal antibody, no genotoxicity studies have been conducted. No carcinogenicity or fertility studies (male or female) have been performed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image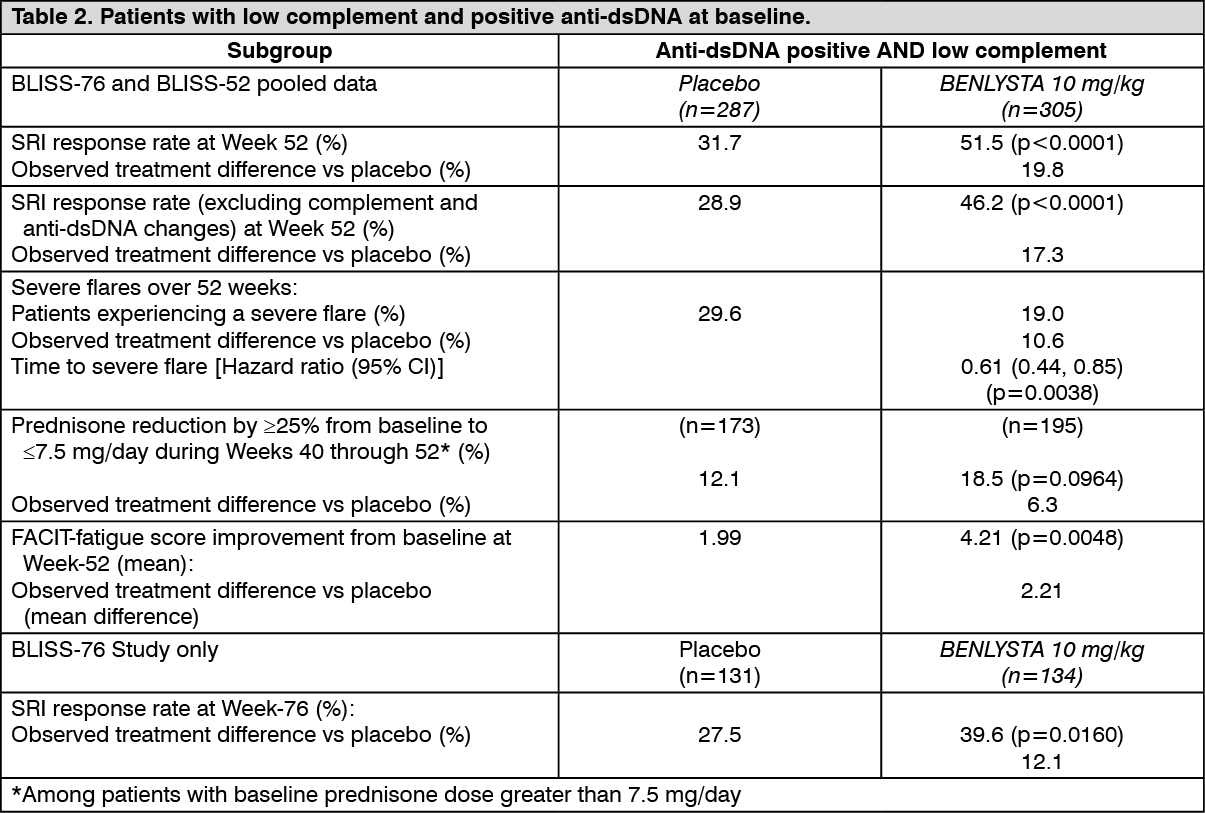 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image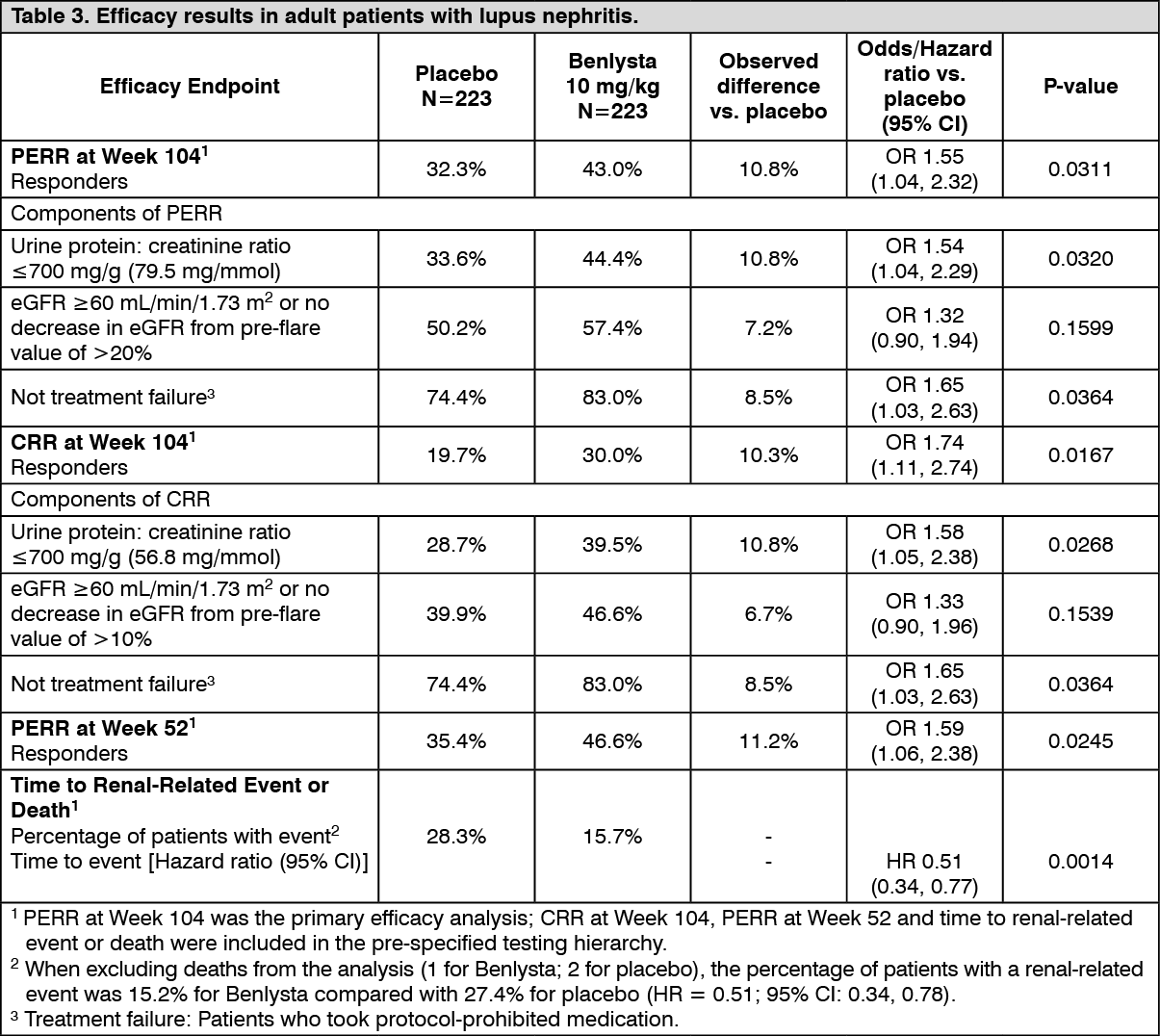 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image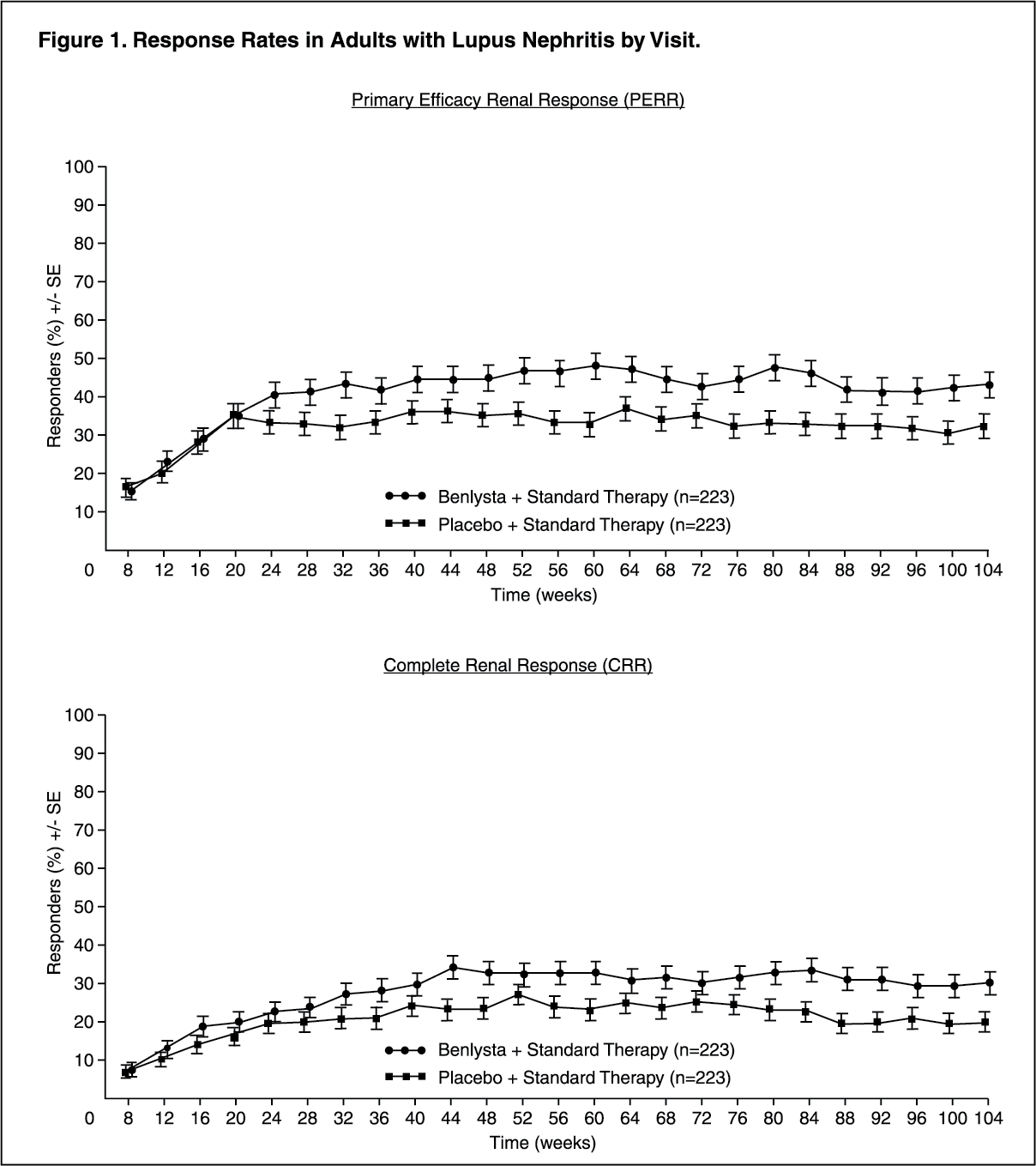 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image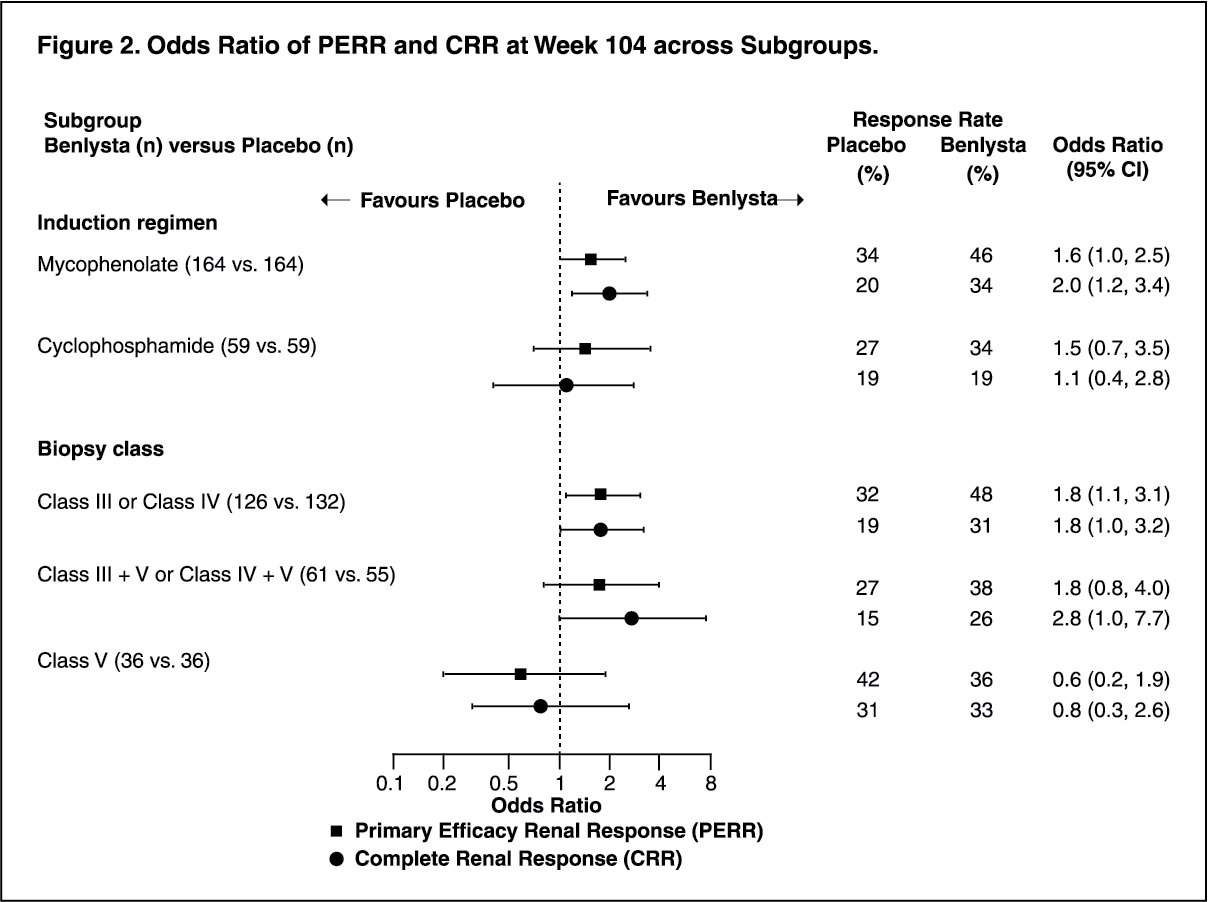 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image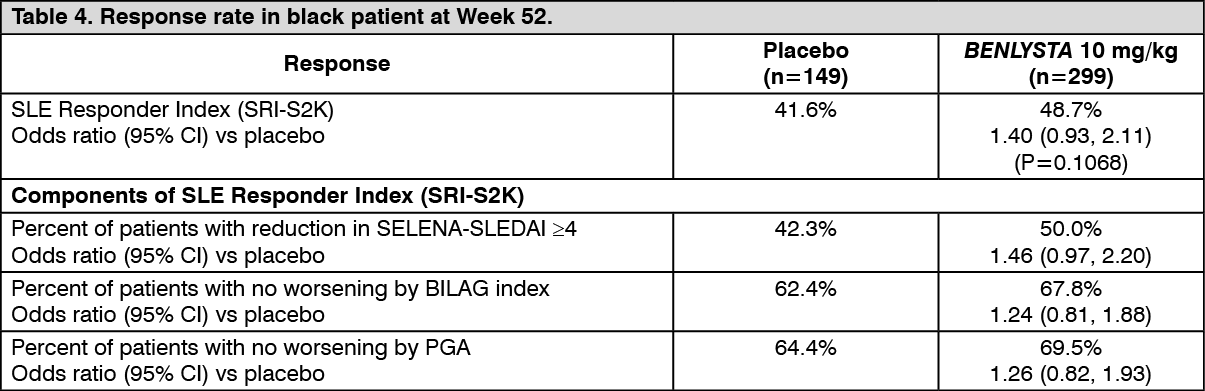 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 120 mg73dcb5e8-4aa0-4d68-966c-a427010f36d0.GIF)

 Sign Out
Sign Out
