


 Sign Out
Sign Out

Clinical Studies: Adult and Adolescent Seasonal Allergic Rhinitis: Once daily 110 micrograms AVAMYS Nasal Spray resulted in a significant improvement in daily reflective (how patient felt over the preceding 12 hours) and instantaneous (how patient felt at the time of assessment) pre-dose total nasal symptom scores (rTNSS and iTNSS, comprising rhinorrhea, nasal congestion, sneezing and nasal itching) and daily reflective and instantaneous total ocular symptom scores (rTOSS, comprising itching/burning, tearing/watering and redness of the eyes) versus placebo (see table 1 as follows). The improvement in nasal and ocular symptoms was maintained over the full 24 hours after once daily administration. (See Table 1.)
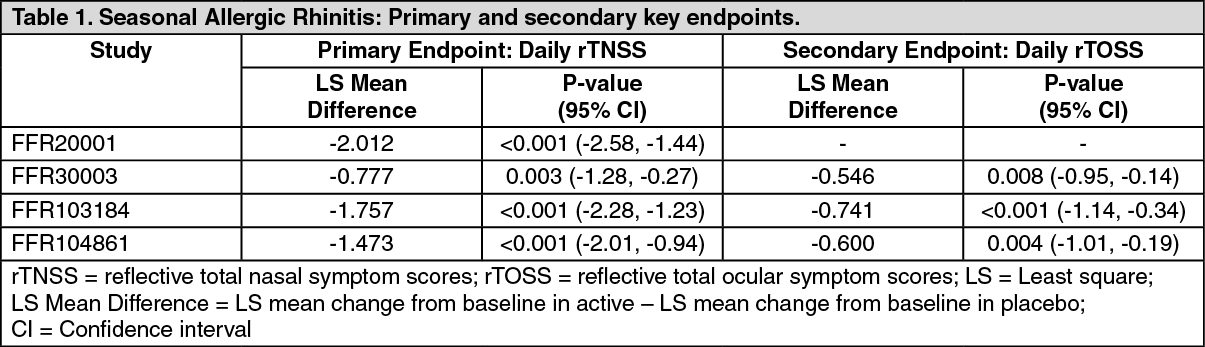 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe distribution of the patients' perception of overall response to therapy (using a 7-point scale ranging from significantly improved to significantly worse) favoured AVAMYS Nasal Spray 110 micrograms over placebo, with a statistically significant treatment difference. Onset of action was experienced as early as eight hours after initial administration in two studies. Significant improvement in symptoms was observed in the first 24 hours in all four studies, and continued to improve over several days. The patients' quality of life (as assessed by the Rhinoconjunctivitis Quality of Life Questionnaire - RQLQ), was significantly improved from baseline with AVAMYS Nasal Spray compared to placebo (Minimum Important Difference in all studies = improvement of at least -0.5 over placebo; treatment difference -0.690, p<0.001, 95% CI -0.84, -0.54).
Adult and Adolescent Perennial Allergic Rhinitis: AVAMYS Nasal Spray 110 micrograms once daily resulted in a significant improvement in daily rTNSS (LS mean difference = -0.706, P=0.005, 95% CI -1.20, -0.21). The improvement in nasal symptoms was maintained over the full 24 hours after once daily administration. The distribution of patients' perception of overall response to therapy was also significantly improved compared to placebo.
In a two-year study designed to assess the ocular safety of fluticasone furoate (110 micrograms once daily intranasal spray), adults and adolescents with perennial allergic rhinitis received either fluticasone furoate (n=367) or placebo (n=181). The primary outcomes [time to increase in posterior subcapsular opacity (≥0.3 from baseline in Lens Opacities Classification System, Version III (LOCS III grade)) and time to increase in intraocular pressure (IOP; ≥7 mmHg from baseline)] were not statistically significant between the two groups. Increases in posterior subcapsular opacity (≥0.3 from baseline) were more frequent in subjects treated with fluticasone furoate 110 micrograms [14 (4%)] versus placebo [4 (2%)] and were transient in nature for ten subjects in the fluticasone furoate group and two subjects in the placebo group. Increases in IOP (≥7 mmHg from baseline) were more frequent in subjects treated with fluticasone furoate 110 micrograms: 7 (2%) for fluticasone furoate 110 micrograms once daily and 1 (<1%) for placebo. These events were transient in nature for six subjects in the fluticasone furoate group and one placebo subject. At weeks 52 and 104, 95% of subjects in both treatment groups had posterior subcapsular opacity values within ±0.1 of baseline values for each eye and, at week 104, ≤1% of subjects in both treatment groups had ≥0.3 increase from baseline in posterior subcapsular opacity. At weeks 52 and 104, the majority of subjects (>95%) had IOP values of within ±5 mmHg of the baseline value. Increases in posterior subcapsular opacity or IOP were not accompanied by any adverse events of cataracts or glaucoma.
Children: The paediatric posology is based on assessment of the efficacy data across the allergic rhinitis population in children. In a seasonal allergic rhinitis study in children, AVAMYS Nasal Spray 110 micrograms over two weeks was effective on primary (daily rTNSS LS mean difference = -0.616, P=0.025, 95% CI -1.15, -0.08) and all secondary nasal endpoints, except the individual reflective score for rhinorrhea. No significant differences were observed between 55 micrograms AVAMYS Nasal Spray and placebo on any endpoint.
In a perennial allergic rhinitis study, Avamys Nasal Spray 55 micrograms was effective on daily rTNSS (LS mean difference = -0.754, P=0.003, 95% CI -1.24, -0.27). Although there was a trend towards improvement in rTNSS in 100 micrograms, this did not reach statistical significance (LS mean difference = -0.452, P=0.073, 95% CI -1.24, -0.04). Post-hoc analysis of efficacy data over 6 and 12 weeks from this study, and a 6-week HPA-axis safety study, each showed that the improvement in rTNSS for Avamys Nasal Spray 110 micrograms nasal spray over placebo was statistically significant.
A randomised, double-blind, parallel-group, multicenter, one-year placebo-controlled clinical growth study evaluated the effect of fluticasone furoate nasal spray 110 micrograms daily on growth velocity in 474 prepubescent children (5 to 7.5 years of age for girls and 5 to 8.5 years of age for boys) with stadiometry. Mean growth velocity over the 52-week treatment period was lower in the patients receiving fluticasone furoate (5.19 cm/year) compared to placebo (5.46 cm/year). The mean treatment difference was -0.27 cm per year [95% CI -0.48 to -0.06].
Pharmacokinetics: Absorption: Fluticasone furoate undergoes extensive first-pass metabolism and incomplete absorption in the liver and gut resulting in negligible systemic exposure. The intranasal dosing of 110 micrograms once daily does not typically result in measurable plasma concentrations (less than 10 picograms/mL). The absolute bioavailability for fluticasone furoate administered as 880 micrograms three times per day (2640 micrograms total daily dose) is 0.50%.
Distribution: The plasma protein binding of fluticasone furoate is greater than 99%. Fluticasone furoate is widely distributed with volume of distribution at steady-state of, on average, 608 L.
Metabolism: Fluticasone furoate is rapidly cleared (total plasma clearance of 58.7 L/h) from systemic circulation principally by hepatic metabolism to an inactive 17 beta-carboxylic metabolite (GW694301X), by the cytochrome P450 enzyme CYP3A4. The principal route of metabolism was hydrolysis of the S-fluoromethyl carbothioate function to form the 17 beta-carboxylic acid metabolite. In vivo studies have revealed no evidence of cleavage of the furoate moiety to form fluticasone.
Elimination: Elimination was primarily via the faecal route following oral and intravenous administration indicative of excretion of fluticasone furoate and its metabolites via the bile. Following intravenous administration, the elimination phase half-life averaged 15.1 hours. Urinary excretion accounted for approximately 1% and 2% of the orally and intravenously administered dose, respectively.
Special Patient Populations: Elderly: Only a small number of elderly subjects (n=23/872; 2.6%) provided pharmacokinetic data. There was no evidence for a higher incidence of subjects with quantifiable fluticasone furoate concentrations in the elderly, when compared to the younger subjects.
Children: Fluticasone furoate is not quantifiable (less than 10 picograms/mL) following intranasal dosing of 110 micrograms once daily. Quantifiable levels were observed in less than 16% of paediatric patients following intranasal dosing of 110 micrograms once daily and only less than 7% of paediatric patients following 55 micrograms once daily. There was no evidence for a higher incidence of quantifiable levels of fluticasone furoate in younger children (less than 6 years of age).
Renal impairment: Fluticasone furoate is not detectable in urine from healthy volunteers after intranasal dosing. Less than 1% of dose-related material is excreted in urine and therefore renal impairment would not be expected to affect the pharmacokinetics of fluticasone furoate.
Hepatic impairment: There are no data on intranasal fluticasone furoate in subjects with hepatic impairment. Data are available following inhaled administration of fluticasone furoate (as fluticasone furoate or fluticasone furoate/vilanterol) to subjects with hepatic impairment that are also applicable for intranasal dosing. A study of a single 400 microgram dose of orally inhaled fluticasone furoate in patients with moderate hepatic impairment (Child-Pugh B) resulted in increased Cmax (42%) and AUC(0-∞) (172%) compared to healthy subjects. Following repeat dosing of orally inhaled fluticasone furoate/vilanterol for 7 days, there was an increase in fluticasone furoate systemic exposure (on average two-fold as measured by AUC(0-24)) in subjects with moderate or severe hepatic impairment (Child-Pugh B or C) compared with healthy subjects. The increase in fluticasone furoate systemic exposure in subjects with moderate hepatic impairment (fluticasone furoate/vilanterol 200/25 micrograms) was associated with an average 34% reduction in serum cortisol compared with healthy subjects. There was no effect on serum cortisol in subjects with severe hepatic impairment (fluticasone furoate/vilanterol 100/12.5 micrograms). Based on these findings the average predicted exposure for 110 micrograms of intranasal fluticasone furoate in patients population would not be expected to result in suppression of cortisol.
Other pharmacokinetic: Fluticasone furoate is typically not quantifiable (less than 10 picograms/mL) following intranasal dosing of 110 micrograms once daily. Quantifiable levels were only observed in less than 31% of patients aged 12 years and above and in less than 16% of paediatric patients following intranasal dosing of 110 micrograms once daily. There was no evidence for gender, age (including paediatrics), or race to be related to those subjects with quantifiable levels, when compared to those without.
Toxicology: Pre-clinical Safety Data: Carcinogenesis, mutagenesis: There were no treatment-related increases in the incidence of tumours in two-year inhalation studies in rats and mice.
AVAMYS Nasal Spray was not genotoxic in vitro or in vivo.
Reproductive toxicology: The potential for reproductive toxicity was assessed in animals by inhalation administration to ensure high systemic exposure to fluticasone furoate. There were no effects on mating performance or fertility of male or female rats. In rats, developmental toxicity was confined to an increased incidence of incompletely ossified sternebrae in association with lower foetal weight. High doses in rabbits induced abortion. These findings are typical following systemic exposure to potent corticosteroids. There were no major skeletal or visceral abnormalities in either rats or rabbits, and no effect on pre- or post-natal development in rats.
Animal toxicology and/or pharmacology: Findings in general toxicology studies were similar to those observed with other glucocorticoids and are not considered to be clinically relevant to intranasal use of AVAMYS Nasal Spray.