Tab: Each tablet contains 2 mg melphalan.
Inj: Each injection is supplied as a unit pack comprising a vial containing sterile, anhydrous mephalan hydrochloride 50 mg with a vial containing a 10 ml solvent-diluent.
Solvent Diluent for Alkeran Injection is a clear, colourless solution with an alcoholic odour, practically free from visible particles.
Excipients/Inactive Ingredients: Tablet Core: Microcrystalline cellulose, Crospovidone, Colloidal anhydrous silica, Magnesium stearate.
Tablet Film Coating: Hypromellose, Titanium dioxide, Macrogol.
Inj: Hydrochloric Acid, Povidone K12, Water for Injections.
Pharmacotherapeutic group: antineoplastic and immunomodulating agents, antineoplastic agents, alkylating agents, nitrogen mustard analogues. ATC Code: L01AA03.
Pharmacology: Pharmacodynamics: Mechanism of Action: Melphalan is a bifunctional alkylating agent. Formation of carbonium intermediates from each of the two bis-2-chloroethyl groups enables alkylation through covalent binding with the 7-nitrogen of guanine on DNA, cross-linking two DNA strands and thereby preventing cell replication.
Pharmacokinetics: Absorption: Tab: The absorption of oral melphalan is highly variable with respect to both the time to first appearance of the drug in plasma and peak plasma concentration.
In studies of the absolute bioavailability of melphalan, the mean absolute bioavailability ranged from 56 to 85%.
In a study of 18 patients administered melphalan 0.2 to 0.25 mg/kg body weight orally, a maximum plasma concentration (range 87 to 350 ng/mL) was reached within 0.5 to 2.0 hours.The administration of melphalan immediately after food delayed the time to achieving peak plasma concentrations and reduced the area under the plasma concentration-time curves by between 39 and 54%.
Inj: Intravenous administration can be used to avoid variability in absorption associated with myeloablative treatment.
Distribution: Melphalan is moderately bound to plasma proteins with reported percent binding ranging from 69 to 78%. There is evidence that the protein binding is linear in the range of plasma concentrations usually achieved in standard dose therapy, but that the binding may become concentration-dependent at the concentrations observed in high-dose therapy. Serum albumin is the major binding protein, accounting for about 55 to 60% the binding, and 20% is bound to α1-acid glycoprotein. In addition, melphalan binding studies have revealed the existence of an irreversible component attributable to the alkylation reaction with plasma proteins.
Melphalan displays limited penetration of the blood-brain barrier. Several investigators have sampled cerebrospinal fluid and found no measurable drug. Low concentrations (~10% of that in plasma) were observed in a single high-dose study in children.
Inj: Following administration of a two-minute infusion of doses ranging from 5 to 23 mg/m2 body surface area (approximately 0.1 to 0.6 mg/kg body weight) to 10 patients with ovarian cancer or multiple myeloma, the mean volumes of distribution at steady state and central compartment were 29.1 ± 13.6 litres and 12.2 ± 6.5 litres, respectively.
In 28 patients with various malignancies who were given doses of between 70 and 200 mg/m2 body surface area as a 2- to 20-min infusion, the mean volumes of distribution at steady state and central compartment were, respectively, 40.2 ± 18.3 litres and 18.2 ± 11.7 litres.
Following hyperthermic (39°C) perfusion of the lower limb with melphalan at 1.75 mg/kg body weight in 11 patients with advanced malignant melanoma, mean volumes of distribution at steady state and central compartment were, respectively, 2.87 ± 0.8 litres and 1.01 ± 0.28 litres.
Biotransformation/Metabolism: In vivo and in vitro data suggest that spontaneous degradation rather than enzymatic metabolism is the major determinant of the drugs half-life in man.
Elimination: Tab: In 13 patients given oral melphalan at 0.6 mg/kg body weight, the plasma mean terminal elimination half-life was 90 ± 57 min with 11% of the drug being recovered in the urine over 24 h.
In 18 patients administered melphalan 0.2 to 0.25 mg/kg body weight orally, the mean elimination half-life was 1.12 ± 0.15 h.
Inj: In 8 patients given a single bolus dose of 0.5 to 0.6 mg/kg body weight, the composite initial and terminal half-lives were reported to be 7.7 ± 3.3 minutes and 108 ± 20.8 minutes, respectively. Following injection of melphalan, monohydroxymelphalan and dihydroxymelphalan were detected in the patients' plasma, reaching peak levels at approximately 60 minutes and 105 minutes, respectively. A similar half-life of 126 ± 6 minutes was seen when melphalan was added to the patients' serum in vitro (37°C), suggesting that spontaneous degradation rather than enzymatic metabolism may be the major determinant of the drug's half-life in man.
Following administration of a 2-minute infusion of doses ranging from 5 to 23 mg/m2 body surface area (approximately 0.1 to 0.6 mg/kg body weight) to 10 patients with ovarian cancer or multiple myeloma, the pooled initial and terminal half-lives were, respectively, 8.1 ± 6.6 minutes and 76.9 ± 40.7 minutes.
In 15 children and 11 adults given high-dose intravenous ALKERAN (140 mg/m2 body surface area) with forced diuresis, the mean initial and terminal half-lives were found to be 6.5 ± 3.6 minutes and 41.4 ± 16.5 minutes, respectively (Ardiet et al., 1986). Mean initial and terminal half-lives of 8.8 ± 6.6 minutes and 73.1 ± 45.9 minutes, respectively, were recorded in 28 patients with various malignancies who were given doses of between 70 and 200 mg/m2 body surface area as a 2- to 20-minute infusion.
Following hyperthermic (39°C) perfusion of the lower limb with 1.75 mg/kg body weight, mean initial and terminal half-lives of 3.6 ± 1.5 minutes and 46.5 ± 17.2 minutes, respectively, were recorded in 11 patients with advanced malignant melanoma.
Special Patient Populations: Renal Impairment: Melphalan clearance may be decreased in renal impairment (see Renal Impairment under Dosage & Administration and Renal impairment under Precautions).
Elderly: No correlation has been shown between age and melphalan clearance or with melphalan terminal elimination half-life (see Dosage & Administration).
Toxicology: Preclinical Safety Data: Carcinogenesis, mutagenesis: Melphalan is mutagenic in animals.
Tab: Fertility studies: In mice, melphalan administered intraperitoneally at a dose of 7.5 mg/kg, showed reproductive effects attributable to cytotoxicity in specific male germ cell stages and induced dominant lethal mutations and heritable translocations in post-meiotic germ cells, particularly in mid to late stage spermatids.
A study was performed to measure the total reproductive capacity of melphalan in female mice. Females received a single intraperitoneal dose of 7.5 mg/kg melphalan and were then housed with an untreated male for most of their reproductive life span (a minimum of 347 days post-treatment). A pronounced reduction in litter size occurred within the first post-treatment interval, followed by an almost complete recovery. Thereafter, a gradual decline in litter size occurred. This was simultaneous with a reduction in the proportion of productive females, a finding associated with an induced reduction in the number of small follicles (see Use in Pregnancy & Lactation).
Tab: Melphalan tablets are indicated in the treatment of: multiple myeloma; advanced ovarian adenocarcinoma.
Melphalan tablets may be used in the treatment of: breast carcinoma: melphalan either alone or in combination with other drugs has a significant therapeutic effect in a proportion of patients suffering from advanced breast carcinoma; polycythaemia rubra vera: melphalan is effective in the treatment of a proportion of patients suffering from polycythaemia vera.
Inj: ALKERAN Injection, administered by regional arterial perfusion, is indicated in the treatment of: localised malignant melanoma of the extremities; localised soft tissue sarcoma of the extremities.
ALKERAN Injection, at conventional intravenous dosage, may be used in the treatment of: multiple myeloma: ALKERAN Injection, either alone or in combination with other cytotoxic drugs, is as effective as the oral formulation in the treatment of multiple myeloma; advanced ovarian cancer: ALKERAN Injection produces an objective response in approximately 50% of the patients with advanced ovarian adenocarcinoma, when given alone, or in combination with other cytotoxic.
ALKERAN Injection, at high intravenous dosage, may be used in the treatment of: multiple myeloma: complete remissions have been achieved in up to 50% of patients given high-dose ALKERAN Injection, with or without haematopoietic stem cell rescue, either as first-line treatment or to consolidate a response to conventional cytoreductive chemotherapy; advanced neuroblastoma in childhood: high-dose ALKERAN Injection with haematopoietic stem cell rescue has been used either alone, or combined with radiotherapy and/or other cytotoxic drugs, to consolidate a response to conventional treatment.
A significant increase in the duration of disease-free survival was demonstrated in a prospective randomised trial of high-dose Alkeran injection versus no further treatment.
General: ALKERAN is a cytotoxic drug which falls into the general class of alkylating agents. It should be prescribed only by physicians experienced in the management of malignant disease with such agents.
Since ALKERAN is myelosuppressive, frequent blood counts are essential during therapy and the dosage should be delayed or adjusted if necessary (see Precautions).
The absorption of melphalan after oral administration is variable.
Dosage may need to be cautiously increased until myelosuppression is seen, in order to ensure that potentially therapeutic levels have been reached.
Tab: Thromboembolic events: Melphalan in combination with lenalidomide and prednisone or in combination with thalidomide and prednisone or dexamethasone is associated with an increased risk of venous thromboembolism. Thromboprophylaxis should be administered for at least the first 5 months of treatment especially in patients with additional thrombotic risk factors. The decision to take antithrombotic prophylactic measures should be made after careful assessment of an individual patient's underlying risk factors (see Precautions and Adverse Reactions).
If the patient experiences any thromboembolic events, treatment must be discontinued and standard anticoagulation therapy started. Once the patient has been stabilised on the anticoagulation treatment and any complications of the thromboembolic event have been managed, melphalan in combination with lenalidomide and prednisone or thalidomide and prednisone or dexamethasone may be restarted at the original dose dependent upon a benefit-risk assessment. The patient should continue anticoagulation therapy during the course of melphalan treatment.
Multiple Myeloma: A typical oral dosage schedule is 0.15 mg/kg body weight daily in divided doses for 4 days repeated at intervals of 6 weeks. Numerous regimens have, however, been used and the scientific literature should be consulted for details.
The administration of oral melphalan and prednisone may be more effective than melphalan alone. The combination is usually given on an intermittent basis.
Prolonging treatment beyond one year in responders does not appear to improve results.
Advanced Ovarian Adenocarcinoma: A typical regimen is 0.2 mg/kg body weight daily orally for 5 days. This is repeated every 4-8 weeks or as soon as the peripheral blood count has recovered.
Carcinoma of the breast: Melphalan has been given orally at a dose of 0.15 mg/kg body weight or 6 mg/m2 body surface area/day for 5 days and repeated every 6 weeks. The dose was decreased if bone marrow toxicity was observed.
Polycythaemia rubra vera: For remission induction, doses of 6 to 10 mg daily for 5 to 7 days have been used, after which 2 to 4 mg daily were given until satisfactory disease control was achieved.
A dose of 2 to 6 mg once per week has been used for maintenance therapy.
In view of the possibility of severe myelosuppression if melphalan is given on a continuous basis, it is essential that frequent blood counts are taken throughout therapy, with dosage adjustment or breaks in treatment, as appropriate, to maintain careful haematological control.
Inj: Multiple myeloma: ALKERAN injection has been used on an intermittent basis alone, or in combination with other cytotoxic drugs, at doses varying between 8 mg/m2 body surface area and 30 mg/m2 body surface area, given at intervals of between 2 to 6 weeks. Additionally, administration of prednisolone has been included in a number of regimens. The literature should be consulted for precise details on treatment protocols.
When used as a single agent, a typical intravenous dosage schedule is 0.4 mg/kg body weight (16 mg/m2 body surface area) repeated at appropriate intervals (e.g. once every 4 weeks), provided there has been recovery of the peripheral blood count during this period.
High-dose regimens generally employ single intravenous doses of between 100 and 200 mg/m2 body surface area (approximately 2.5 to 5 mg/kg body weight), but haematopoietic stem cell rescue becomes essential following doses in excess of 140 mg/m2 body surface area. In cases of renal impairment, the dose should be reduced by 50% (see Dosage in renal impairment as follows). In view of the severe myelosuppression induced by high-dose ALKERAN injection, treatment should be confined to specialist centres with the appropriate facilities, and only be administered by experienced clinicians (see Precautions).
Advanced ovarian adenocarcinoma: When used intravenously as a single agent, a dose of 1 mg/kg body weight (approximately 40 mg/m2 body surface area) given at intervals of 4 weeks has often been used.
When combined with other cytotoxic drugs, intravenous doses of between 0.3 and 0.4 mg/kg body weight (12-16 mg/m2 body surface area) have been used at intervals of 4 to 6 weeks.
Malignant melanoma: Hyperthermic regional perfusion with Alkeran has been used as an adjuvant to surgery for early malignant melanoma and as palliative treatment for advanced but localised disease.
The scientific literature should be consulted for details of perfusion technique and dosage used.
Soft tissue sarcoma: Hyperthermic regional perfusion with Alkeran has been used in the management of all stages of localised soft tissue sarcoma, usually in combination with surgery.
ALKERAN has also been given with actinomycin D and the scientific literature should be consulted for details of dosage regimens.
Advanced neuroblastoma in childhood: Doses including 100 and 240 mg/m2 body surface area (sometimes divided equally over 3 consecutive days) together with haematopoietic stem cell rescue have been used either alone or in combination with radiotherapy and/or other cytotoxic drugs.
Preparation of ALKERAN Injection Solution: (see Instructions for Use/Handling under Cautions for Usage).
Parenteral administration: Except in cases where regional arterial perfusion is indicated, ALKERAN Injection is for intravenous use only.
For intravenous administration, it is recommended that ALKERAN Injection solution is injected slowly into a fast-running infusion solution via a swabbed injection port.
If direct injection into a fast-running infusion is not appropriate, ALKERAN Injection solution may be administered diluted in an infusion bag. ALKERAN Injection is not compatible with infusion solutions containing dextrose, and it is recommended that ONLY Sodium Chloride Intravenous Infusion 0.9% w/v is used.
Care should be taken to avoid possible extravasation of ALKERAN and in cases of poor peripheral venous access, consideration should be given to use of a central venous line.
If high-dose ALKERAN Injection is administered with or without autologous bone marrow transplantation, administration via a central venous line is recommended.
For regional arterial perfusion, the literature should be consulted for detailed methodology.
Use in children: ALKERAN, within the conventional dosage range, is only rarely indicated in children and absolute dosage guidelines cannot be provided.
Inj: High-dose ALKERAN Injection, in association with bone marrow rescue, has been used in childhood neuroblastoma and dosage guidelines based on body surface area are used in this situation (see Advanced neuroblastoma in childhood as previously mentioned).
Use in the elderly: Although ALKERAN is frequently used at conventional dosage in the elderly, there is no specific information available relating to its administration to this patient sub-group.
Inj: Experience in the use of ALKERAN in elderly patients is limited.
Consideration should therefore be given to ensure adequate performance status and organ function before using high-dose ALKERAN Injection in elderly patients.
The pharmacokinetics of intravenous melphalan has not shown a correlation between age and melphalan clearance or with melphalan terminal elimination half-life. The limited data available do not support specific dosage adjustment recommendations for elderly patients receiving intravenous melphalan and suggested that current practice of dosage adjustment based upon the general condition if the geriatric patient and the degree of myelosuppression incurred during therapy should be continued.
Dosage in renal impairment: ALKERAN clearance, though variable, may be decreased in renal impairment (see Precautions).
Tab: Currently available pharmacokinetic data do not justify an absolute recommendation on dosage reduction when administering melphalan to patients with renal impairment, but it may be prudent to use a reduced dosage initially until tolerance is established.
Inj: When ALKERAN Injection is used at conventional intravenous dosage (8 to 40 mg/m2 body surface area), it is recommended that the initial dose should be reduced by 50% in patients with moderate to severe renal impairment and subsequent dosage determined according to the degree of haematological suppression.
For high intravenous doses of Alkeran (100 to 240 mg/m2 body surface area), the need for dose reduction depends upon the degree of renal impairment, whether haematopoietic stem cells are reinfused and therapeutic need.
As a guide, for high-dose ALKERAN treatment without haematopoietic stem cell rescue in patients with moderate renal impairment (creatinine clearance 30 to 50 ml/min), a dose reduction of 50% is usual. High-dose Alkeran without haematopoietic stem cell rescue is not recommended in patients with more severe renal impairment.
High-dose ALKERAN with haematopoietic stem cell rescue has been used successfully even in dialysis-dependent patients with end-stage renal failure. The relevant literature should be consulted for details.
Symptoms and signs: The principal toxic effect is bone marrow suppression, leading to leucopenia, thrombocytopenia and anaemia.
Tab: Gastrointestinal effects, including nausea, vomiting and diarrhoea are the most likely early signs of acute oral overdosage.
Inj: The immediate effects of acute intravenous overdosage are nausea and vomiting. Damage to the gastrointestinal mucosa may also ensue, and diarrhoea, sometimes haemorrhagic, has been reported after overdosage.
Treatment: General supportive measures, together with appropriate blood and platelet transfusions, should be instituted if necessary and consideration given to hospitalisation, cover with anti-infective agents, and the use of haematological growth factors.
There is no specific antidote. The blood picture should be closely monitored for at least 4 weeks following overdosage until there is evidence of recovery.
Tab: Hypersensitivity to the active substance or to any of the excipients.
Lactation.
Inj: ALKERAN should not be given to patients who have suffered a previous hypersensitivity reaction to melphalan.
ALKERAN is an active cytotoxic agent for use under the direction of physicians experienced in the administration of such agents.
Immunisation using a live organism vaccine has the potential to cause infection in immunocompromised hosts. Therefore, immunisations with live organism vaccines are not recommended.
Inj: ALKERAN Injection solution may cause local tissue damage should extravasation occur and consequently, it should not be administered by direct injection into a peripheral vein. It is recommended that ALKERAN Injection solution is administered by injecting slowly into a fast-running intravenous infusion via a swabbed injection port or via a central venous line.
In view of the hazards involved and the level of supportive care required, the administration of high-dose ALKERAN Injection should be confined to specialist centres, with the appropriate facilities and only be conducted by experienced clinicians.
In patients receiving high-dose ALKERAN Injection, consideration should be given to the prophylactic administration of anti-infective agents and the administration of blood products as required.
Consideration should be given to ensure adequate performance status and organ function before using high-dose ALKERAN Injection.
Safe Handling of ALKERAN: Safe handling of ALKERAN (see Instructions for Use/Handling under Cautions for Usage).
The handling of ALKERAN formulations should follow guidelines for the handling of cytotoxic drugs according to prevailing local recommendations and/or regulations (for example, Royal Pharmaceutical Society of Great Britain Working Party on the Handling of Cytotoxic Drugs).
Monitoring: Since ALKERAN is a potent myelosuppressive agent, it is essential that careful attention should be paid to the monitoring of blood counts to avoid the possibility of excessive myelosuppression and the risk of irreversible bone marrow aplasia.
Blood counts may continue to fall after treatment is stopped, so at the first sign of an abnormally large fall in leucocyte or platelet counts, treatment should be temporarily interrupted.
ALKERAN should be used with caution in patients who have undergone recent radiotherapy or chemotherapy in view of increased bone marrow toxicity.
Tab: Contraception: Due to an increased risk of venous thromboembolism in patients undergoing treatment with melphalan in combination with lenalidomide and prednisone or in combination with thalidomide and prednisone or dexamethasone, combined oral contraceptive pills are not recommended. If a patient is currently using combined oral contraception, she should switch to another reliable contraceptive method (i.e. barrier method etc). The risk of venous thromboembolism continues for 4-6 weeks after discontinuing combined oral contraception.
It is recommended that men who are receiving treatment with melphalan not father a child during treatment and up to 6 months afterwards and that they have a consultation on sperm preservation before treatment due to the possibility of irreversible infertility as a result of melphalan treatment.
Effects on Ability to Drive and Use Machines: No data.
Renal Impairment: ALKERAN clearance may be reduced in patients with renal impairment, who may also have uraemic bone marrow suppression. Dosage reduction may therefore be necessary (see Dosage & Administration), and these patients should be closely observed.
Carcinogenicity: ALKERAN, in common with other alkylating agents, has been reported to be leukaemogenic. There have been reports of acute leukaemia occurring after ALKERAN treatment for diseases such as amyloid, malignant melanoma, multiple myeloma, macroglobulinaemia, cold agglutinin syndrome and ovarian cancer.
A comparison of patients with ovarian cancer who received alkylating agents with those who did not show that the use of alkylating agents, including ALKERAN, significantly increased the incidence of acute leukaemia.
The leukaemogenic risk must be balanced against the potential therapeutic benefit when considering the use of ALKERAN.
Tab: Solid tumours: Use of alkylating agents has been linked with the development of second primary malignancy (SPM). In particular, melphalan in combination with lenalidomide and prednisone and, to a lesser extent, thalidomide and prednisone has been associated with the increased risk of solid SPM in elderly newly diagnosed multiple myeloma patients.
Patient characteristics (eg. age, ethnicity), primary indication and treatment modalities (e.g. radiation therapy, transplantation), as well as environmental risk factors (e.g. tobacco use) should be evaluated prior to melphalan administration.
Mutagenicity: Chromosome aberrations have been observed in patients being treated with the drug.
Fertility: ALKERAN causes suppression of ovarian function in premenopausal women resulting in amenorrhoea in a significant number of patients.
There is evidence from some animal studies that ALKERAN can have an adverse effect on spermatogenesis. Therefore, it is possible that ALKERAN may cause temporary or permanent sterility in male patients.
Pregnancy: The teratogenic potential of ALKERAN has not been studied. In view of its mutagenic properties and structural similarity to known teratogenic compounds, it is possible that melphalan could cause congenital defects in the offspring of patients treated with the drug.
As with all cytotoxic chemotherapy, adequate contraceptive precautions should be practised when either partner is receiving ALKERAN.
The use of melphalan should be avoided whenever possible during pregnancy, particularly during the first trimester. In any individual case the potential hazard to the foetus must be balanced against the expected benefit to the mother.
Breastfeeding: Mothers receiving ALKERAN should not breast-feed.
For this product there is no modern clinical documentation which can be used as support for determining the frequency of undesirable effects. Undesirable effects may vary in their incidence depending on the indication and dose received and also when given in combination with other therapeutic agents.
The following convention has been utilised for the classification of frequency: Very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1000 and <1/100); rare (≥1/10,000 and <1/1000); very rare (<1/10,000), not known (cannot be estimated from the available data).
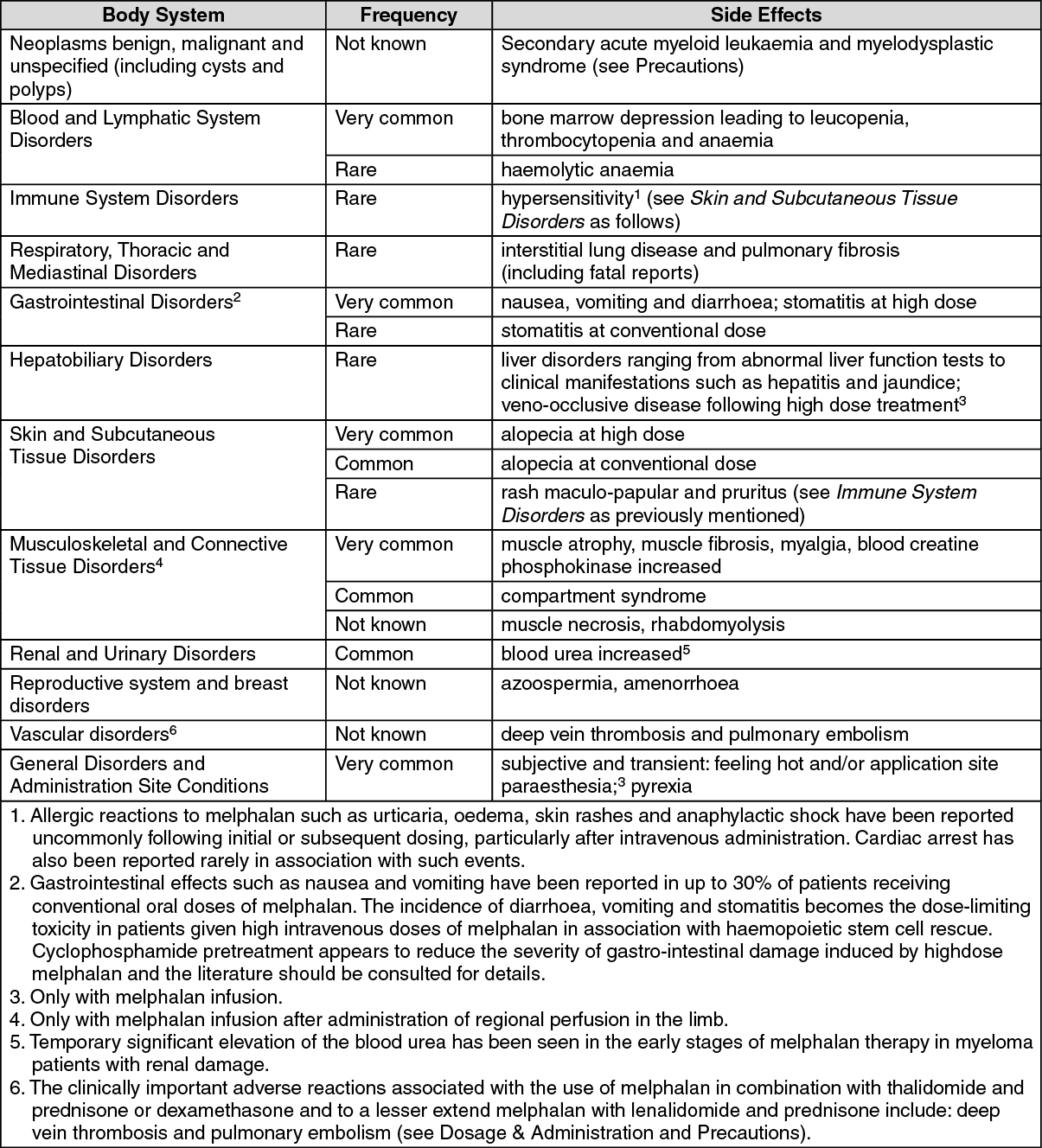
Tab: Tabulated list of adverse reactions: (see table.)
 Click on icon to see table/diagram/image
Inj: Blood and Lymphatic System Disorders:
Click on icon to see table/diagram/image
Inj: Blood and Lymphatic System Disorders: Very common: bone marrow depression leading to leucopenia, thrombocytopenia and anaemia. Rare: haemolytic anaemia.
Immune System Disorders: Rare: allergic reactions (see Skin and Subcutaneous Tissue Disorders as follows).
Allergic reactions to ALKERAN such as urticaria, oedema, skin rashes and anaphylactic shock have been reported uncommonly following initial or subsequent dosing, particularly after intravenous administration. Cardiac arrest has also been reported rarely in association with such events.
Respiratory, Thoracic and Mediastinal Disorders: Rare: interstitial pneumonitis and pulmonary fibrosis (including fatal reports).
Gastrointestinal Disorders: Very common: nausea, vomiting and diarrhoea; stomatitis at high dose. Rare: stomatitis at conventional dose.
The incidence of diarrhoea, vomiting and stomatitis becomes the dose-limiting toxicity in patients given high intravenous doses of ALKERAN in association with autologous bone marrow transplantation. Cyclophosphamide pre-treatment appears to reduce the severity of gastrointestinal damage induced by high-dose ALKERAN and the literature should be consulted for details.
Hepatobiliary Disorders: Rare: hepatic disorders ranging from abnormal liver function tests to clinical manifestations such as hepatitis and jaundice; veno-occlusive disease following high dose treatment.
Skin and Subcutaneous Tissue Disorders: Very common: alopecia at high dose. Common: alopecia at conventional dose. Rare: maculopapular rashes and pruritus (see Immune System Disorders as previously mentioned).
Musculoskeletal and Connective Tissue Disorders: Injection, following isolated limb perfusion: Very common: muscle atrophy, muscle fibrosis, myalgia blood creatine phosphokinase increased. Common: compartment syndrome. Not known: muscle necrosis, rhabdomyolysis.
Renal and Urinary Disorders: Common: temporary significant elevation of the blood urea has been seen in the early stages of ALKERAN therapy in myeloma patients with renal damage.
General Disorders and Administration Site Conditions: Very common: subjective and transient sensation of warmth and/or tingling.
Live organism vaccines: Vaccinations with live organism vaccines are not recommended in immunocompromised individuals (see Precautions).
Nalidixic Acid: Nalidixic acid together with high-dose intravenous ALKERAN has caused deaths in children due to haemorrhagic enterocolitis.
Cyclosporin: Impaired renal function has been described in bone marrow transplant patients who were conditioned with high-dose intravenous ALKERAN and who subsequently received cyclosporin to prevent graft-versus-host disease.
Tab: Busulfan: In paediatric population, for the Busulfan-Melphalan regimen it has been reported that the administration of melphalan less than 24 hours after the last oral busulfan administration may influence the development of toxicities.
Incompatibilities: Tab: None known.
Inj: ALKERAN Injection is not compatible with infusion solutions containing dextrose, and it is recommended that ONLY Sodium Chloride Intravenous Infusion 0.9% w/v is used.
Special Precautions for Disposal and Other Handling: Tab: Safe handling of melphalan tablets: The handling of melphalan should follow guidelines for the handling of cytotoxic drugs according to prevailing local recommendations and/or regulations.
Provided the outer coating of the tablet is intact, there is no risk in handling melphalan tablets.
Melphalan tablets should not be divided.
Inj: Alkeran injection should be prepared for administration either by or under the direct supervision of a pharmacist who is familiar with its properties and safe handling requirements.
Alkeran injection should be prepared for use in the aseptic unit of a pharmacy equipped with a suitable vertical laminar flow cabinet. Where such a facility is not available, a specially designated side room of a ward or clinic may be used.
Personnel preparing or handling Alkeran injection should wear the following protective clothing: Disposable gloves of surgical latex or polyvinylchloride of a suitable quality (rubber gloves are not adequate); surgical face mask of suitable quality; protective goggles or glasses which should be washed thoroughly with water after use; disposable apron.
In an aseptic facility, other suitable clothing will be required.
Any spillage should be dealt with immediately (by personnel wearing suitable protective clothing), by mopping with damp, disposable paper towels which are placed in a high-risk waste disposal bag after use and disposed of in compliance with relevant local legislation. Contaminated surfaces should be washed with copious quantities of water.
Should Alkeran injection solution come into contact with the skin, wash immediately, and thoroughly with soap and plenty of cold water. In such instances, it may be prudent to seek medical advice.
In case of contact with eyes, immediate irrigation with sodium chloride eye wash should be carried out and medical attention sought without delay. If sodium chloride solution is not available, large volumes of water may be used.
Disposal: Tab: Melphalan tablets should be destroyed in accordance with relevant local regulatory requirements concerning the disposal of cytotoxic drugs.
Inj: ALKERAN Injection solution should be disposed of in compliance with relevant local legislation. In the absence of such guidelines, the solution should be disposed of in a manner appropriate for toxic chemicals, for example, high-temperature incineration or deep burial.
Disposal of sharp objects, such as needles, syringes, administration sets and ampoules should be in rigid containers labelled with a suitable hazard warning seal. Personnel involved in disposal should be aware of the precautions to be observed, and the material should be destroyed by incineration if appropriate. All disposal must be in accordance with local regulatory requirements.
Instructions for Use/Handling: Safe Handling of ALKERAN Injection: ALKERAN Injection should be prepared for administration either by or under the direct supervision of a pharmacist who is familiar with its properties and safe handling requirements.
ALKERAN Injection should be prepared for use in the aseptic unit of a pharmacy equipped with a suitable vertical laminar flow cabinet. Where such a facility is not available, a specially designated side room of a ward or clinic may be used.
Personnel preparing or handling ALKERAN Injection should wear the following protective clothing: Disposable gloves of surgical latex or polyvinylchloride of a suitable quality (rubber gloves are not adequate); Surgical facemask of suitable quality; Protective goggles or glasses which should be washed thoroughly with water after use; Disposable apron.
In an aseptic facility, other suitable clothing will be required.
Any spillage should be dealt with immediately (by personnel wearing suitable protective clothing), by mopping with damp, disposable paper towels which are placed in a high-risk waste disposal bag after use and disposed of in compliance with relevant local legislation. Contaminated surfaces should be washed with copious quantities of water.
Should ALKERAN Injection solution come into contact with the skin, wash immediately and thoroughly with soap and plenty of cold water. In such instances it may be prudent to seek medical advice.
In case of contact with eyes, IMMEDIATE irrigation with sodium chloride eye wash should be carried out and medical attention sought without delay. If sodium chloride solution is not available, large volumes of water may be used.
Preparation of ALKERAN Injection Solution: (See also Safe Handling of ALKERAN as previously mentioned).
ALKERAN Injection should be prepared, AT ROOM TEMPERATURE, by reconstituting the freeze-dried powder with the Solvent-Diluent provided. 10 ml of this vehicle should be added, as a single quantity, and the vial immediately shaken vigorously until solution is complete. The resulting solution contains the equivalent of 5 mg/ml anhydrous melphalan and has a pH of approximately 6.5.
ALKERAN Injection solution has limited stability and should be prepared immediately before use. Any unused solution should be discarded (see Disposal as previously mentioned).
The reconstituted solution should not be refrigerated as this will cause precipitation.
When further diluted in an infusion solution, ALKERAN Injection has reduced stability and the rate of degradation increases rapidly with rise in temperature. If administration occurs at a room temperature of approximately 25°C, the total time from preparation of the Injection solution to the completion of infusion should not exceed 1.5 hours.
Should any visible turbidity or crystallization appear in the reconstituted or diluted solutions the preparation must be discarded.
Tab: Store at 2°C to 8°C.
Inj: Store below 30°C. Protect from light.
L01AA03 - melphalan ; Belongs to the class of alkylating agents, nitrogen mustard analogues. Used in the treatment of cancer.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
