ACTILYSE should be given as early as possible after symptom onset.
Posology: Acute myocardial infarction: a) 90 minutes (accelerated) dose regimen: for patients with acute myocardial infarction, in whom treatment can be started within 6 hours after symptom onset.
In patients with a body weight ≥ 65 kg: 15 mg as an intravenous bolus, immediately followed by 50 mg as an intravenous infusion over the first 30 minutes, followed by an intravenous infusion of 35 mg over 60 minutes, until the maximum dose of 100 mg.
In patients with a body weight < 65 kg the total dose should be weight adjusted with: 15 mg as an intravenous bolus, immediately followed by 0.75 mg/kg body weight as an intravenous infusion over the first 30 minutes (maximum 50 mg), followed by an intravenous infusion of 0.5 mg/kg over 60 minutes (up to a maximum of 35 mg).
b) 3 hours dose regimen: for patients with acute myocardial infarction, in whom treatment can be started between 6 and 12 hours after symptom onset.
In patients with a body weight ≥ 65 kg: 10 mg as an intravenous bolus, immediately followed by 50 mg as an intravenous infusion over the first hour, followed by an intravenous infusion of 40 mg for the next two hours, until the maximum dose of 100 mg.
In patients with a body weight < 65 kg: 10 mg as an intravenous bolus, immediately followed by an intravenous infusion up to a maximum total dose of 1.5 mg/kg.
Adjunctive therapy: Antithrombotic adjunctive therapy is recommended according to the current international guidelines for the management of patients with ST-elevation myocardial infarction.
Acute massive pulmonary embolism: In patients with a body weight ≥ 65 kg: A total dose of 100 mg should be administered in 2 hours. The most experience available is with the following dose regimen: 10 mg as an intravenous bolus over 1 - 2 minutes, immediately followed by 90 mg as an intravenous infusion over two hours until the total dose of 100 mg.
In patients with a body weight < 65 kg: 10 mg as an intravenous bolus over 1 - 2 minutes, immediately followed by an intravenous infusion up to a maximum total dose of 1.5 mg/kg.
Adjunctive therapy: After treatment with ACTILYSE heparin therapy should be initiated (or resumed) when aPTT values are less than twice the upper limit of normal. The infusion should be adjusted to maintain aPTT between 50 - 70 seconds (1.5 to 2.5 fold of the reference value).
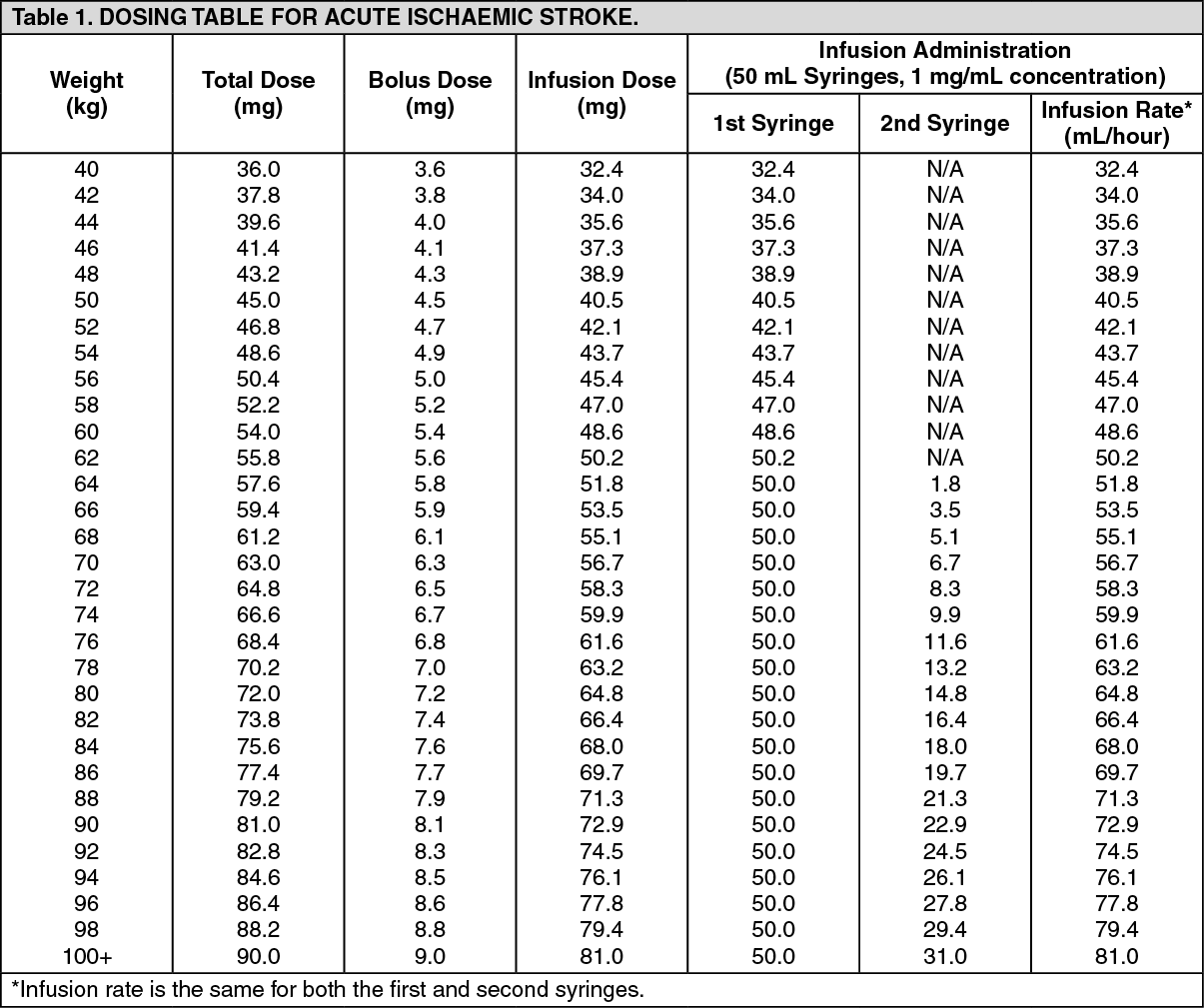
Acute ischaemic stroke: The recommended total dose is 0.9 mg/kg body weight (maximum of 90 mg) infused starting with 10% of the total dose as an initial intravenous bolus, immediately followed by the remainder of the total dose infused intravenously over 60 minutes.
Treatment should be initiated as early as possible within 4.5 hours of symptom onset, see Precautions. The treatment effect is time-dependent; therefore earlier treatment increases the probability of a favourable outcome. Beyond 4.5 hours after onset of stroke symptoms there is a negative benefit risk ratio associated with Actilyse administration and so it should not be administered (see Pharmacology: Pharmacodynamics under Actions). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Adjunctive therapy: The safety and efficacy of this regimen with concomitant administration of heparin or platelet aggregation inhibitors such as acetylsalicylic acid during the first 24 hours after the symptom-onset has not been investigated sufficiently. Therefore, administration of intravenous heparin or platelet aggregation inhibitors such as acetylsalicylic acid should be avoided in the first 24 hours after treatment with ACTILYSE due to an increased haemorrhagic risk.
If heparin is required for other indications (e.g. prevention of deep vein thrombosis) the dose should not exceed 10,000 IU per day, administered subcutaneously.
Method of administration: The reconstituted solution should be administered intravenously and is for immediate use.
Instructions for use/Handling: Under aseptic conditions the contents of an injection vial of ACTILYSE (50 mg) dry substance is dissolved with sterilised water for injection according to the following table to obtain a final concentration of 1 mg alteplase per ml. (See Table 2.)
Click on icon to see table/diagram/image
For this purpose a transfer cannula is included with the pack-sizes of 50 mg.
Instructions for reconstituting Actilyse: 1. Reconstitute immediately before administration.
2. Remove the protective cap on the two vials containing the sterile water and ACTILYSE dry substance by flipping them up with a thumb.
3. Swab the rubber top of each vial with an alcohol wipe.
4. Remove the transfer cannula* from its cover. Do not disinfect or sterilize the transfer cannula; it is sterile. Take one cap off.
5. Stand the sterile water vial upright on a stable surface. From directly above, puncture the rubber stopper vertically in the stopper centre with the transfer cannula by pressing gently but firmly, without twisting.
6. Hold the sterile water vial and the transfer cannula steady with one hand using the two side flaps.
Remove the remaining cap on top of the transfer cannula.
7. Hold the sterile water vial and the transfer cannula steady with one hand using the two side flaps.
Hold the vial with ACTILYSE dry substance above the transfer cannula and position the tip of the transfer cannula right in the centre of the stopper.
Push down the vial with the dry substance onto the transfer cannula from directly above, puncturing the rubber stopper vertically and gently but firmly without twisting.
8. Invert the two vials and allow the water to drain completely into the dry substance.
9. Remove the empty water vial together with the transfer cannula.
They can be disposed of.
10. Take the vial with reconstituted ACTILYSE and swirl gently to dissolve any remaining powder, but do not shake, as this will produce foam.
If there are bubbles, let the solution stand undisturbed for a few minutes to allow them to disappear.
11. The solution consists of 1 mg/mL ACTILYSE. It should be clear and colourless to pale yellow and it should not contain any particles.
12. Remove the amount required using a needle and syringe. Do not use the puncture location from the transfer cannula to avoid leakage.
13. Use immediately.
Dispose of any unused solution.
(*if a transfer cannula is included in the kit. The reconstitution can also be performed with a syringe and a needle.)
The 1 mg/mL reconstituted solution may be diluted further with sterile sodium chloride 9 mg/mL (0.9%) solution for Injection up to a minimal concentration of 0.2 mg/mL since the occurrence of turbidity of the reconstituted solution cannot be excluded.
A further dilution of the 1 mg/mL reconstituted solution with sterilised water for injections or in general, the use of carbohydrate infusion solutions, e.g. dextrose is not recommended due to increasing formation of turbidity of the reconstituted solution.
ACTILYSE should not be mixed with other drugs, neither in the same infusion-vial nor the same venous line (not even with heparin).
Traceability: In order to improve traceability of biological medicinal products, the trade name and the batch number of the administered product should be clearly recorded in the patient file.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image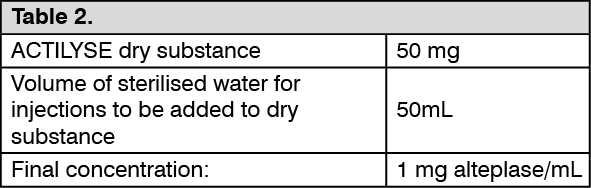 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image 50 mg9983b8c0-1d02-4815-b2cb-9faa0009b0e5.GIF)

 Sign Out
Sign Out
