


 Sign Out
Sign Out



The proportion of patients who discontinued treatment due to adverse events during the double-blind, controlled portion of pivotal studies was 5.9% for patients taking adalimumab and 5.4% for control-treated patients.
The most commonly reported adverse reactions are infections (such as nasopharyngitis, upper respiratory tract infection and sinusitis), injection site reactions (erythema, itching, haemorrhage, pain or swelling), headache and musculoskeletal pain.
Serious adverse reactions have been reported for adalimumab. TNF-antagonists, such as adalimumab affect the immune system and their use may affect the body's defence against infection and cancer.
Fatal and life-threatening infections (including sepsis, opportunistic infections and TB), HBV reactivation and various malignancies (including leukaemia, lymphoma and HSTCL) have also been reported with use of adalimumab.
Serious haematological, neurological and autoimmune reactions have also been reported. These include rare reports of pancytopenia, aplastic anaemia, central and peripheral demyelinating events and reports of lupus, lupus-related conditions and Stevens-Johnson syndrome.
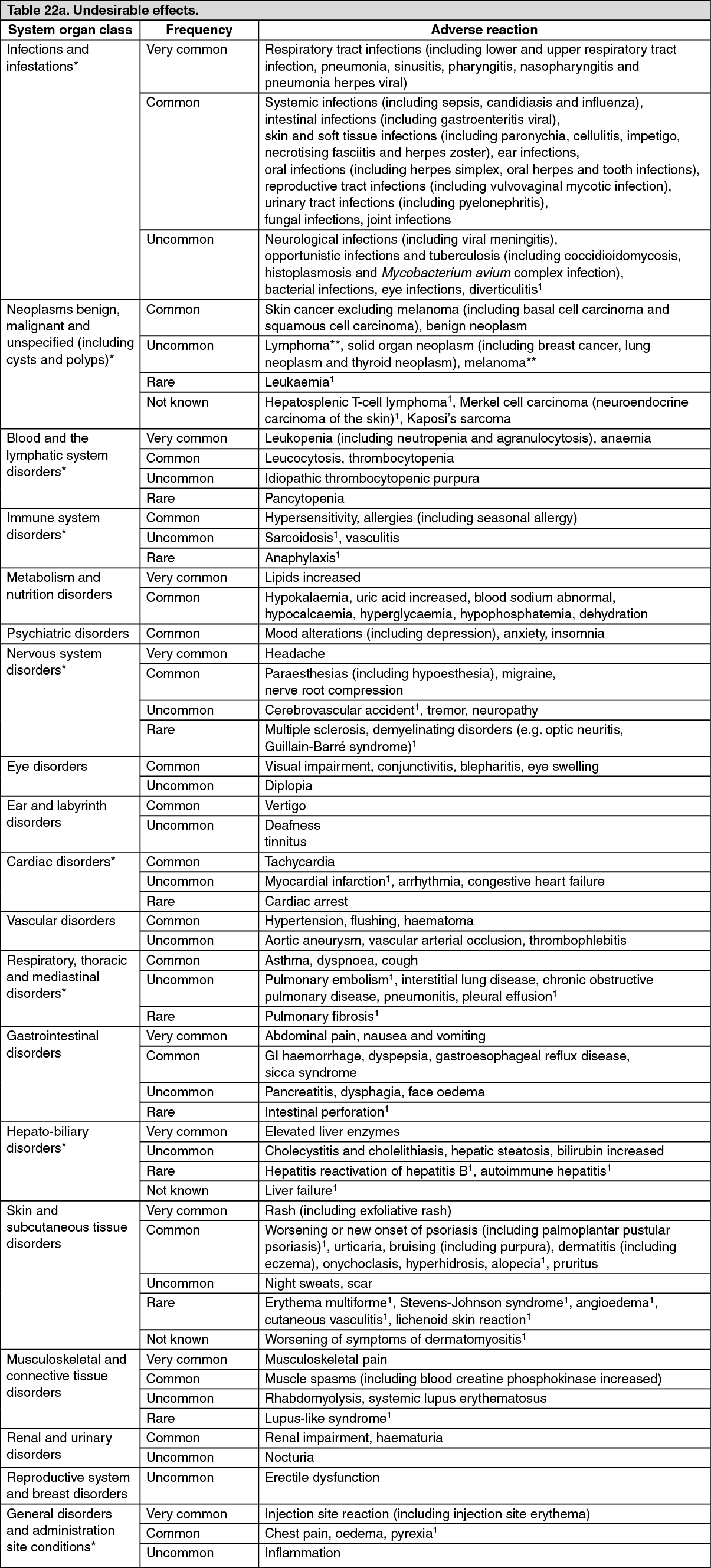
Tabulated list of adverse reactions: The following list of adverse reactions is based on experience from clinical trials and on postmarketing experience and are displayed by system organ class and frequency in Table 22 as follows: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); and not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. The highest frequency seen among the various indications has been included. An asterisk (*) appears in the SOC column if further information is found elsewhere in Contraindications, Precautions and as follows. (See Table 22.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image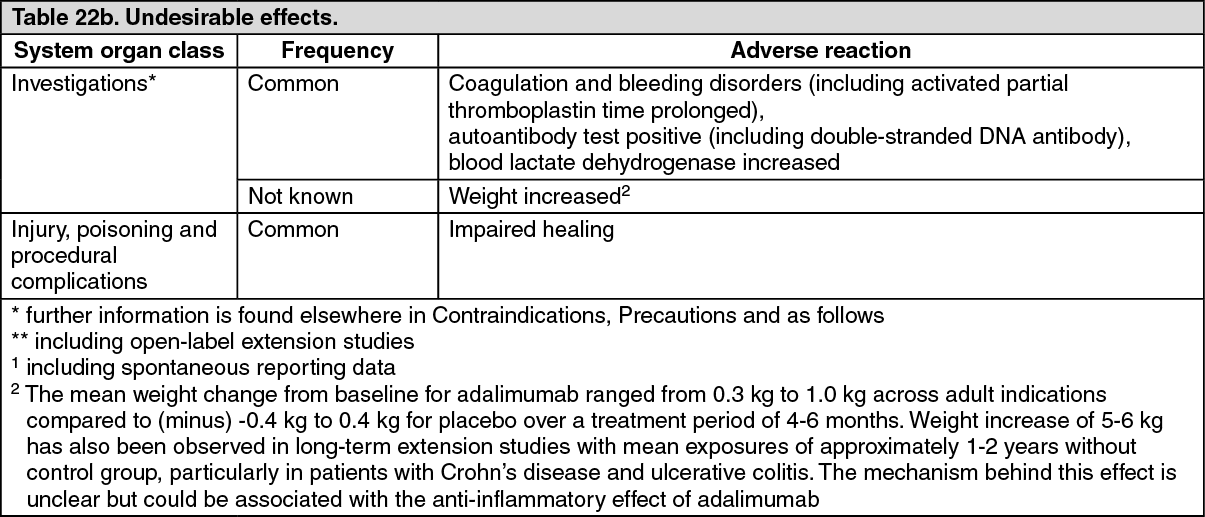 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHidradenitis suppurativa: The safety profile for patients with HS treated with adalimumab weekly was consistent with the known safety profile of adalimumab.
Uveitis: The safety profile for patients with uveitis treated with adalimumab every other week was consistent with the known safety profile of adalimumab.
Description of selected adverse reactions: Injection site reactions: In the pivotal controlled trials in adults and children, 12.9% of patients treated with adalimumab developed injection site reactions (erythema and/or itching, haemorrhage, pain or swelling), compared to 7.2% of patients receiving placebo or active control. Injection site reactions generally did not necessitate discontinuation of the medicinal product.
Infections: In the pivotal controlled trials in adults and children, the rate of infection was 1.51 per patient year in the adalimumab-treated patients and 1.46 per patient year in the placebo and active control-treated patients. The infections consisted primarily of nasopharyngitis, upper respiratory tract infection, and sinusitis. Most patients continued on adalimumab after the infection resolved.
The incidence of serious infections was 0.04 per patient year in adalimumab-treated patients and 0.03 per patient year in placebo and active control-treated patients.
In controlled and open-label adult and paediatric studies with adalimumab, serious infections (including fatal infections, which occurred rarely) have been reported, which include reports of tuberculosis (including miliary and extra-pulmonary locations) and invasive opportunistic infections (e.g. disseminated or extrapulmonary histoplasmosis, blastomycosis, coccidioidomycosis, pneumocystis, candidiasis, aspergillosis and listeriosis). Most of the cases of tuberculosis occurred within the first eight months after initiation of therapy and may reflect recrudescence of latent disease.
Malignancies and lymphoproliferative disorders: During the controlled portions of pivotal adalimumab trials in adults of at least 12 weeks in duration in patients with moderately to severely active rheumatoid arthritis, ankylosing spondylitis, axial spondyloarthritis without radiographic evidence of AS, psoriatic arthritis, psoriasis, hidradenitis suppurativa, Crohn's disease, ulcerative colitis and uveitis, malignancies, other than lymphoma and non-melanoma skin cancer, were observed at a rate (95% confidence interval) of 6.8 (4.4, 10.5) per 1,000 patient-years among 5,291 adalimumab-treated patients versus a rate of 6.3 (3.4, 11.8) per 1,000 patient-years among 3,444 control patients (median duration of treatment was 4.0 months for adalimumab and 3.8 months for control-treated patients). The rate (95% confidence interval) of non-melanoma skin cancers was 8.8 (6.0, 13.0) per 1,000 patient-years among adalimumab-treated patients and 3.2 (1.3, 7.6) per 1,000 patient-years among control patients. Of these skin cancers, squamous cell carcinomas occurred at rates (95% confidence interval) of 2.7 (1.4, 5.4) per 1,000 patient-years among adalimumab-treated patients and 0.6 (0.1, 4.5) per 1,000 patient-years among control patients. The rate (95% confidence interval) of lymphomas was 0.7 (0.2, 2.7) per 1,000 patient-years among adalimumab-treated patients and 0.6 (0.1, 4.5) per 1,000 patient-years among control patients.
When combining controlled portions of these trials and ongoing and completed open-label extension studies with a median duration of approximately 3.3 years including 6,427 patients and over 26,439 patient-years of therapy, the observed rate of malignancies, other than lymphoma and non-melanoma skin cancers is approximately 8.5 per 1,000 patient-years. The observed rate of non-melanoma skin cancers is approximately 9.6 per 1,000 patient-years, and the observed rate of lymphomas is approximately 1.3 per 1,000 patient-years.
In post-marketing experience from January 2003 to December 2010, predominantly in patients with rheumatoid arthritis, the reported rate of malignancies is approximately 2.7 per 1,000 patient treatment years. The reported rates for non-melanoma skin cancers and lymphomas are approximately 0.2 and 0.3 per 1,000 patient treatment years, respectively (see Precautions).
Rare post-marketing cases of hepatosplenic T-cell lymphoma have been reported in patients treated with adalimumab (see Precautions).
Autoantibodies: Patients had serum samples tested for autoantibodies at multiple time points in rheumatoid arthritis studies I - V. In these trials, 11.9% of patients treated with adalimumab and 8.1% of placebo and active control-treated patients that had negative baseline anti-nuclear antibody titres reported positive titres at Week 24. Two patients out of 3,441 treated with adalimumab in all rheumatoid arthritis and psoriatic arthritis studies developed clinical signs suggestive of new-onset lupus-like syndrome. The patients improved following discontinuation of therapy. No patients developed lupus nephritis or central nervous system symptoms.
Hepato-biliary events: In controlled Phase 3 trials of adalimumab in patients with rheumatoid arthritis and psoriatic arthritis with a control period duration ranging from 4 to 104 weeks, ALT elevations ≥3 x ULN occurred in 3.7% of adalimumab-treated patients and 1.6% of control-treated patients.
In controlled Phase 3 trials of adalimumab in patients with polyarticular juvenile idiopathic arthritis who were 4 to 17 years and enthesitis-related arthritis who were 6 to 17 years, ALT elevations ≥3 x ULN occurred in 6.1% of adalimumab-treated patients and 1.3% of control-treated patients. Most ALT elevations occurred with concomitant methotrexate use. No ALT elevations ≥3 x ULN occurred in the Phase 3 trial of adalimumab in patients with polyarticular juvenile idiopathic arthritis who were 2 to <4 years.
In controlled Phase 3 trials of adalimumab in patients with Crohn's disease and ulcerative colitis with a control period ranging from 4 to 52 weeks. ALT elevations ≥3 x ULN occurred in 0.9% of adalimumab-treated patients and 0.9% of controlled-treated patients.
In controlled Phase 3 trials of adalimumab in patients with plaque psoriasis with a control period duration ranging from 12 to 24 weeks, ALT elevations ≥3 x ULN occurred in 1.8% of adalimumab-treated patients and 1.8% of control-treated patients.
In controlled trials of adalimumab (initial doses of 160 mg at Week 0 and 80 mg at Week 2, followed by 40 mg every week starting at Week 4), in patients with hidradenitis suppurativa with a control period duration ranging from 12 to 16 weeks, ALT elevations ≥3 x ULN occurred in 0.3% of adalimumab-treated patients and 0.6% of control-treated patients.
In controlled trials of adalimumab (initial doses of 80 mg at Week 0 followed by 40 mg every other week starting at Week 1) in adult patients with uveitis up to 80 weeks with a median exposure of 166.5 days and 105.0 days in adalimumab-treated and control-treated patients, respectively, ALT elevations ≥3 x ULN occurred in 2.4% of adalimumab-treated patients and 2.4% of control-treated patients.
Across all indications in clinical trials patients with raised ALT were asymptomatic and in most cases elevations were transient and resolved on continued treatment. However, there have also been post-marketing reports of liver failure as well as less severe liver disorders that may precede liver failure, such as hepatitis including autoimmune hepatitis in patients receiving adalimumab.
Concurrent treatment with azathioprine/6-mercaptopurine: In adult Crohn's disease studies, higher incidences of malignant and serious infection-related adverse events were seen with the combination of adalimumab and azathioprine/6-mercaptopurine compared with adalimumab alone.
View ADR Monitoring Form