Each containing 500 mg valaciclovir as valaciclovir hydrochloride 556 mg.
Excipients/Inactive Ingredients: Tablet core: Microcrystalline cellulose, Crospovidone, Povidone K90, Magnesium stearate, Colloidal silicon dioxide, Purified water.
Film coat: Hydroxypropylmethylcellulose, Titanium dioxide, Polyethylene glycol, Polysorbate 80 (500 and 1,000 mg tablets only), Purified water, Carnauba wax.
Pharmacology: Pharmacodynamics: Mechanism of Action: Valaciclovir, an antiviral, is the L-valine ester of aciclovir. Aciclovir is a purine (guanine) nucleoside analogue.
Valaciclovir is rapidly and almost completely converted in man to aciclovir and valine, probably by the enzyme referred to as valaciclovir hydrolase. Aciclovir is a specific inhibitor of the herpes viruses with in vitro activity against herpes simplex viruses (HSV) types 1 and 2, varicella-zoster virus (VZV), cytomegalovirus (CMV), Epstein-Barr Virus (EBV), and human herpes virus 6 (HHV-6). Aciclovir inhibits herpes virus DNA synthesis once it has been phosphorylated to the active triphosphate form.
The first stage of phosphorylation requires the activity of a virus-specific enzyme. In the case of HSV, VZV and EBV, this enzyme is the viral thymidine kinase (TK), which is only present in virus-infected cells.
Selectivity is maintained in CMV with phosphorylation, at least in part, being mediated through the phosphotransferase gene product of UL97.
This requirement for activation of aciclovir by a virus-specific enzyme largely explains its selectivity.
The phosphorylation process is completed (conversion from mono- to triphosphate) by cellular kinases. Aciclovir triphosphate competitively inhibits the virus DNA polymerase and incorporation of this nucleoside analogue results in obligate chain termination, halting virus DNA synthesis and thus blocking virus replication.
Pharmacodynamic Effects: Resistance is normally due to a thymidine kinase-deficient phenotype which results in a virus which is profoundly disadvantaged in the natural host. Infrequently, reduced sensitivity to aciclovir has been described as a result of subtle alterations in either the virus thymidine kinase or DNA polymerase. The virulence of these variants resembles that of the wild-type virus.
Extensive monitoring of clinical isolates from patients receiving aciclovir therapy or prophylaxis has revealed that virus with reduced sensitivity to aciclovir is extremely rare in the immunocompetent and is only found infrequently in severely immunocompromised individuals e.g. organ or bone marrow transplant recipients, patients receiving chemotherapy for malignant disease and people infected with the human immunodeficiency virus (HIV).
Pharmacokinetics: Absorption: After oral administration, valaciclovir is well absorbed and rapidly and almost completely converted to aciclovir and valine. This conversion is probably mediated by an enzyme isolated from human liver referred to as valaciclovir hydrolase. The bioavailability of aciclovir from 1,000 mg valaciclovir is 54%, and is not reduced by food.
VALTREX pharmacokinetics are not dose-proportional. The rate and extent of absorption decrease with increasing dose, resulting in a less than proportional increase in Cmax over the therapeutic dose range and a reduced bioavailability at doses above 500 mg.
Mean peak aciclovir concentrations are 10 to 37 micromoles (2.2 to 8.3 micrograms/mL) following single doses of 250 to 2,000 mg valaciclovir to healthy subjects with normal renal function, and occur at a median time of 1 to 2 h post dose.
Peak plasma concentrations of valaciclovir are only 4% of aciclovir levels, occur at a median time of 30 to 100 min post dose, and are at or below the limit of quantification 3 h after dosing. The valaciclovir and aciclovir pharmacokinetic profiles are similar after single and repeat dosing.
Herpes zoster and herpes simplex do not significantly alter the pharmacokinetics of valaciclovir and aciclovir after oral administration of valaciclovir.
Pregnant women: In a study of the pharmacokinetics of valaciclovir and aciclovir during late pregnancy, the steady-state daily aciclovir AUC (area under plasma concentration-time curve) following valaciclovir 1,000 mg was approximately 2 times greater than that observed with oral aciclovir at 1,200 mg daily.
For information on transfer into breast milk see Use in Pregnancy & Lactation.
HIV infection: In patients with HIV infection, the disposition and pharmacokinetic characteristics of aciclovir after oral administration of single or multiple doses of 1,000 mg or 2,000 mg valaciclovir are unaltered compared with healthy subjects.
Distribution: Binding of valaciclovir to plasma proteins is very low (15%). CSF penetration, determined by CSF/plasma AUC ratio, is about 25% for aciclovir and the metabolite 8-hydroxy-aciclovir (8-OH-ACV), and about 2.5% for the metabolite 9-(carboxymethoxy) methylguanine (CMMG) (see Pharmacokinetics: Special Patient Populations).
Metabolism: After oral administration, VALTREX is converted to aciclovir and L-valine by first-pass intestinal and/or hepatic metabolism. Aciclovir is converted to a small extent to the metabolites 9-(carboxymethoxy) methylguanine (CMMG) by alcohol and aldehyde dehydrogenase and to 8-hydroxy-aciclovir (8-OH-ACV) by aldehyde oxidase. Approximately 88% of the total combined plasma exposure is attributable to aciclovir, 11% to CMMG and 1% to 8-OH-ACV. Neither VALTREX nor aciclovir is metabolised by cytochrome P450 enzymes.
Elimination: In patients with normal renal function, the plasma elimination half-life of aciclovir after both single and multiple dosing with valaciclovir is approximately 3 h.
Less than 1% of the administered dose of valaciclovir is recovered in the urine as unchanged drug. Valaciclovir is eliminated in the urine principally as aciclovir (greater than 80% of the recovered dose) and the known aciclovir metabolite, 9-(carboxymethoxy) methylguanine (CMMG).
Special Patient Populations: Renal impairment: The elimination of aciclovir is correlated to renal function, and exposure to aciclovir will increase with increased renal impairment. In patients with end-stage renal disease, the average elimination half-life of aciclovir after VALTREX administration is approximately 14 hours, compared with about 3 hours for normal renal function (see Dosage & Administration).
Exposure to aciclovir and its metabolites CMMG and 8-OH-ACV in plasma and cerebrospinal fluid (CSF) was evaluated at steady-state after multiple-dose VALTREX administration in 6 subjects with normal renal function (mean creatinine clearance 111 mL/min, range 91-144 mL/min) receiving 2,000 mg every 6 hours and 3 subjects with severe renal impairment (mean CLcr 26 mL/min, range 17-31 mL/min) receiving 1,500 mg every 12 hours. In plasma as well as CSF, concentrations of aciclovir, CMMG and 8-OH-ACV were on average 2, 4 and 5-6 times higher, respectively, in severe renal impairment compared with normal renal function. There was no difference in extent of CSF penetration (as determined by CSF/plasma AUC ratio) for aciclovir, CMMG or 8-OH-aciclovir between the two populations (see Pharmacokinetics: Distribution in the previous text).
Hepatic impairment: Pharmacokinetic data indicate that hepatic impairment decreases the rate of conversion of VALTREX to aciclovir but not the extent of conversion. Aciclovir half-life is not affected.
Toxicology: Preclinical Safety Data: The results of mutagenicity tests in vitro and in vivo indicate that Valtrex is unlikely to pose a genetic risk to humans.
Valaciclovir was not carcinogenic in bio-assays performed in mice and rats.
Valaciclovir did not affect fertility in male or female rats dosed by the oral route.
At high parenteral doses of aciclovir testicular atrophy and aspermatogenesis have been observed in rats and dogs.
Valaciclovir was not teratogenic in rats or rabbits. Valaciclovir is almost completely metabolised to aciclovir. Subcutaneous administration of aciclovir in internationally accepted tests did not produce teratogenic effects in rats or rabbits. In additional studies in rats, foetal abnormalities were observed at subcutaneous doses that produced plasma levels of 100 micrograms/mL and maternal toxicity.
VALTREX is indicated for the treatment of herpes zoster (shingles).
VALTREX is indicated for the treatment of herpes simplex infections (HSV) of the skin and mucous membranes, including initial and recurrent genital herpes.
Adults: Treatment of herpes zoster (shingles): The dosage is 1,000 mg of VALTREX to be taken three times daily for seven days.
Treatment of herpes simplex infections: For treatment of herpes simplex, 500 mg of VALTREX to be taken twice daily.
For recurrent episodes, treatment should be for 5 days. For initial episodes, which can be more severe, treatment may have to be extended to 10 days. Dosing should begin as early as possible. For recurrent episodes of herpes simplex, this should ideally be during the prodromal period or immediately the first signs or symptoms appear.
Children: There are no data available on the use of VALTREX in children.
Elderly: The possibility of renal impairment in the elderly must be considered and the dosage should be adjusted accordingly (see Renal impairment as follows).
Adequate hydration should be maintained.
Renal Impairment: Caution is advised when administering valaciclovir to patients with impaired renal function. Adequate hydration should be maintained.
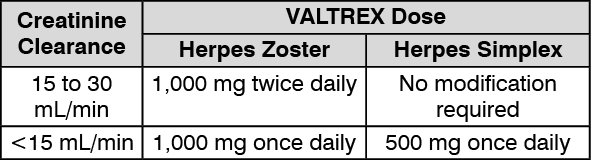
The dosage of Valtrex should be reduced in patients with significantly impaired renal function as shown in the table as follows: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In patients on hemodialysis, the VALTREX dosage recommended for patients with a creatinine clearance of less than 15 mL/min should be used. This should be administered after the haemodialysis has been performed.
Hepatic Impairment: Studies with a 1 g unit dose of VALTREX show that dose modification is not required in patients with mild or moderate cirrhosis (hepatic synthetic function maintained). Pharmacokinetic data in patients with advanced cirrhosis (impaired hepatic synthetic function and evidence of portal-systemic shunting) do not indicate the need for dosage adjustment; however, clinical experience is limited.
Dosage in special patient groups: No specific dosage recommendations.
Monitoring Advice: No special monitoring necessary.
Instruction for Use: No special instruction for use.
Symptoms and signs: Acute renal failure and neurological symptoms, including confusion, hallucinations, agitation, decreased consciousness and coma, have been reported in patients receiving overdoses of valaciclovir. Nausea and vomiting may also occur.
Caution is required to prevent inadvertent overdosing. Many of the reported cases involved renally impaired and elderly patients receiving repeated overdoses, due to lack of appropriate dosage reduction.
Treatment: Patients should be observed closely for signs of toxicity. Haemodialysis significantly enhances the removal of aciclovir from the blood and may, therefore, be considered a management option in the event of symptomatic overdose.
VALTREX is contraindicated in patients known to be hypersensitive to valaciclovir, aciclovir or any components of formulations of VALTREX.
Hydration Status: Care should be taken to ensure adequate fluid intake in patients who are at risk of dehydration, particularly the elderly.
Use in Patients with Renal Impairment and in Elderly Patients: Aciclovir is eliminated by renal clearance, therefore the dose of valaciclovir must be reduced in patients with renal impairment (see Dosage & Administration). Elderly patients are likely to have reduced renal function and therefore the need for dose reduction must be considered in this group of patients. Both elderly patients and patients with renal impairment are at increased risk of developing neurological side effects and should be closely monitored for evidence of these effects. In the reported cases, these reactions were generally reversible on discontinuation of treatment (see Adverse Reactions).
Effects on the Ability to Drive and Use Machines: The clinical status of the patient and the adverse event profile of VALTREX should be borne in mind when considering the patient's ability to drive or operate machinery. There have been no studies to investigate the effect of valaciclovir on driving performance or the ability to operate machinery. Further, a detrimental effect on such activities cannot be predicted from the pharmacology of the active substance.
Fertility: In animal studies, VALTREX did not affect fertility. However, high parenteral doses of aciclovir caused testicular effects in rats and dogs (see Toxicology: Preclinical Safety Data under Actions).
No human fertility studies were performed with VALTREX, but no changes in sperm count, motility or morphology were reported in 20 patients after 6 months of daily treatment with 400 mg to 1 g aciclovir.
Use in pregnancy: There are limited data on the use of VALTREX in pregnancy. VALTREX should only be used in pregnancy if the potential benefits of treatment outweigh the potential risk.
Pregnancy registries have documented the pregnancy outcomes in women exposed to VALTREX or to any formulation of ZOVIRAX (aciclovir, the active metabolite of VALTREX); 111 and 1,246 outcomes (29 and 756 exposed during the first trimester of pregnancy), respectively, were obtained from women prospectively registered. The findings of the aciclovir pregnancy registry have not shown an increase in the number of birth defects amongst aciclovir-exposed subjects compared with the general population, and any birth defects showed no uniqueness or consistent pattern to suggest a common cause. Given the small number of women enrolled into the valaciclovir pregnancy registry, reliable and definitive conclusions could not be reached regarding the safety of VALTREX in pregnancy (see Pharmacology: Pharmacokinetics under Actions).
Use in lactation: Aciclovir, the principle metabolite of VALTREX, is excreted in breast milk. Following oral administration of a dose of a 500 mg dose of VALTREX, peak aciclovir concentrations (Cmax) in breast milk ranged from 0.5 to 2.3 (median 1.4) times the corresponding maternal aciclovir serum concentrations. The aciclovir breast milk to maternal serum AUC ratios ranged from 1.4 to 2.6 (median 2.2). The median aciclovir concentration in breast milk was 2.24 micrograms/mL (9.95 micromoles). With a maternal VALTREX dosage of 500 mg twice daily, this level would expose a nursing infant to a daily oral aciclovir dosage of about 0.61 mg/kg/day. The elimination half-life of aciclovir from breast milk was similar to that for serum.
Unchanged valaciclovir was not detected in maternal serum, breast milk, or infant urine.
Caution is advised if VALTREX is to be administered to a nursing woman.
Fertility: In animal studies, VALTREX did not affect fertility. However, high parenteral doses of aciclovir caused testicular effects in rats and dogs (see Toxicology: Preclinical Safety Data under Actions).
No human fertility studies were performed with VALTREX, but no changes in sperm count, motility or morphology were reported in 20 patients after 6 months of daily treatment with 400 mg to 1 g aciclovir.
Pregnancy: There are limited data on the use of VALTREX in pregnancy. VALTREX should only be used in pregnancy if the potential benefits of treatment outweigh the potential risk.
Pregnancy registries have documented the pregnancy outcomes in women exposed to VALTREX or to any formulation of ZOVIRAX (aciclovir, the active metabolite of VALTREX); 111 and 1,246 outcomes (29 and 756 exposed during the first trimester of pregnancy), respectively, were obtained from women prospectively registered. The findings of the aciclovir pregnancy registry have not shown an increase in the number of birth defects amongst aciclovir-exposed subjects compared with the general population, and any birth defects showed no uniqueness or consistent pattern to suggest a common cause. Given the small number of women enrolled into the valaciclovir pregnancy registry, reliable and definitive conclusions could not be reached regarding the safety of VALTREX in pregnancy (see Pharmacology: Pharmacokinetics under Actions).
Lactation: Aciclovir, the principle metabolite of VALTREX, is excreted in breast milk. Following oral administration of a dose of a 500 mg dose of VALTREX, peak aciclovir concentrations (Cmax) in breast milk ranged from 0.5 to 2.3 (median 1.4) times the corresponding maternal aciclovir serum concentrations. The aciclovir breast milk to maternal serum AUC ratios ranged from 1.4 to 2.6 (median 2.2). The median aciclovir concentration in breast milk was 2.24 micrograms/mL (9.95 micromoles). With a maternal VALTREX dosage of 500 mg twice daily, this level would expose a nursing infant to a daily oral aciclovir dosage of about 0.61 mg/kg/day. The elimination half-life of aciclovir from breast milk was similar to that for serum.
Unchanged valaciclovir was not detected in maternal serum, breast milk, or infant urine.
Caution is advised if VALTREX is to be administered to a nursing woman.
Adverse reactions are listed as follows by MedDRA body system organ class and by frequency:
The frequency categories used are: Very common ≥1 in 10, common ≥1 in 100 and <1 in 10, uncommon ≥1 in 1,000 and <1 in 100, rare ≥1 in 10,000 and <1 in 1,000, very rare <1 in 10,000.
Clinical trial data have been used to assign frequency categories to adverse reactions if, in the trials, there was evidence of an association with VALTREX (i.e. there was a statistically significant difference
between the incidence in patients taking VALTREX and placebo). For all other adverse events, spontaneous post-marketing data has been used as a basis for allocating frequency.
Clinical Trial Data: Nervous System Disorder: Common: Headache.
Gastrointestinal Disorder: Common: Nausea.
Post-Marketing Data: Blood and Lymphatic System Disorders: Very Rare: Leukopenia, thrombocytopenia.
Leukopenia is mainly reported in immunocompromised patients.
Immune System Disorders: Very Rare: Anaphylaxis.
Psychiatric and Nervous System Disorders: Rare: Dizziness, confusion, hallucinations, decreased consciousness. Very Rare: Agitation, tremor, ataxia, dysarthria, psychotic symptoms, convulsions, encephalopathy, coma.
The previously mentioned events are generally reversible and usually seen in patients with renal impairment or with other predisposing factors (see Precautions). In organ transplant patients receiving
high doses (8 g daily) of VALTREX for CMV prophylaxis, neurological reactions occurred more frequently compared with lower doses.
Respiratory, Thoracic and Mediastinal Disorders: Uncommon: Dyspnoea.
Gastrointestinal Disorders: Rare: Abdominal discomfort, vomiting, diarrhoea.
Hepatobiliary Disorders: Very Rare: Reversible increases in liver function tests. These are occasionally described as hepatitis.
Skin and Subcutaneous Tissue Disorders: Uncommon: Rashes including photosensitivity. Rare: Pruritus. Very Rare: Urticaria, angioedema.
Renal and Urinary Disorders: Rare: Renal impairment. Very Rare: Acute renal failure, renal pain. Renal pain may be associated with renal failure.
Other: There have been reports of renal insufficiency, microangiopathic haemolytic anaemia and thrombocytopenia (sometimes in combination) in severely immunocompromised patients,
particularly those with advanced HIV disease, receiving high doses (8 g daily) of VALTREX for prolonged periods in clinical trials. These findings have been observed in patients not treated with
VALTREX who have the same underlying or concurrent conditions.
No clinically significant interactions have been identified. Aciclovir is eliminated primarily unchanged in the urine via active renal tubular secretion. Any drugs administered concurrently that compete with this mechanism may increase aciclovir plasma concentrations following VALTREX administration.
Following 1 g valaciclovir, cimetidine and probenecid increase the AUC of aciclovir by this mechanism, and reduce aciclovir renal clearance. However, no dosage adjustment is necessary at this dose because of the wide therapeutic index of aciclovir.
In patients receiving higher doses of VALTREX (4 g or more/day), caution is required during concurrent administration with drugs which compete with aciclovir for elimination, because of the potential for increased plasma levels of one or both drugs or their metabolites. Increases in plasma AUCs of aciclovir and of the inactive metabolite of mycophenolate mofetil, an immunosuppressant agent used in transplant patients, have been shown when oral aciclovir and mycophenolate mofetil are co-administered.
Care is also required (with monitoring for changes in renal function) if administering higher doses of VALTREX (4 g or more/day) with drugs which affect other aspects of renal physiology (e.g. cyclosporin, tacrolimus).
Instructions for Use/Handling: No special instructions for use.
Incompatibilities: No data.
Store below 30°C.
Shelf-Life: The expiry date is indicated on the packaging.
J05AB11 - valaciclovir ; Belongs to the class of nucleosides and nucleotides excluding reverse transcriptase inhibitors. Used in the systemic treatment of viral infections.
Valtrex FC tab 500 mg
3 × 14's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
