


 Sign Out
Sign Out



Opioid agonist ceiling effects were observed during clinical pharmacology studies in opioid-dependent persons.
Naloxone is an antagonist at mu-opioid receptors. Because of its almost complete first pass metabolism, naloxone administered orally or sublingually has no detectable pharmacological activity. However, when administered IV to opioid-dependent persons, the presence of naloxone in Suboxone produces marked opioid antagonist effects and opioid withdrawal, thereby, deterring IV abuse.
Pharmacokinetics: Buprenorphine: Absorption: Buprenorphine, when taken orally, undergoes first pass metabolism with N-dealkylation and glucuroconjugation in the small intestine and the liver. The use of Suboxone by the oral route is therefore inappropriate.
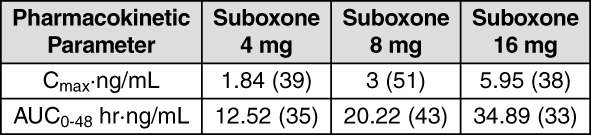
Peak plasma concentrations are achieved 90 min after sublingual administration. Plasma levels of buprenorphine increased with the sublingual dose of Suboxone. Both Cmax and AUC of buprenorphine increased with an increase in dose (in the range of 4-16 mg), although the increase was less than dose proportional.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageValues in the table represent the mean and [coefficient of variation in percentage (%)].
Distribution: The absorption of buprenorphine is followed by a rapid distribution phase (distribution half-life of 2-5 hrs).
Metabolism and Elimination: Buprenorphine is metabolized by 14-N-dealkylation and glucuroconjugation of the parent molecule and the dealkylated metabolite. Clinical data confirm that CYP3A4 is responsible for the N-dealkylation of buprenorphine. N-dealkylbuprenorphine is a mu-opioid agonist with weak intrinsic activity.
Elimination of buprenorphine is bi- or tri-exponential and has a mean half-life from plasma of 32 hrs. Buprenorphine is eliminated in the feces by biliary excretion of the glucuroconjugated metabolites (70%), the rest being eliminated in the urine. Naloxone: Absorption and Distribution: Following IV administration, naloxone is rapidly distributed (distribution half-life ~4 min). Following oral administration, naloxone is barely detectable in plasma, following sublingual administration of Suboxone, plasma naloxone concentrations are low and decline rapidly.
Metabolism and Elimination: Naloxone is metabolized in the liver, primarily by glucuronide conjugation and excreted in the urine. Naloxone has a mean half-life from plasma of 1.2 hrs.
Special Populations: Elderly: No pharmacokinetic data in elderly patients are available.
Renal Impairment: Renal elimination plays a relatively small role (~30%) in the overall clearance of Suboxone. No dose modification based on renal function is required but caution is recommended when dosing subjects with severe renal impairment.
Hepatic Impairment: Hepatic elimination plays a relatively large role (~70%) in the overall clearance of Suboxone and the action of buprenorphine may be prolonged in subjects with impaired hepatic clearance. Lower initial Suboxone doses and cautious titration of dosage may be required in patients with mild to moderate hepatic dysfunction. Suboxone is contraindicated in patients with severe hepatic dysfunction (see Contraindications).
Clinical Efficacy: Efficacy and safety data for Suboxone are primarily derived from a 1-year clinical trial, comprising a 4-week randomized double-blind comparison of Suboxone, buprenorphine and placebo tablets followed by a 48-week safety study of Suboxone. In this trial, 326 heroin-addicted subjects were randomly assigned to either Suboxone 16 mg/day, buprenorphine 16 mg/day or placebo tablets. For subjects randomized to either active treatment, dosing began with one 8-mg tablet of buprenorphine on day 1, followed by buprenorphine 16 mg (two 8-mg tablets) on day 2. On day 3, those randomized to receive Suboxone were switched to the combination tablet. Subjects were seen daily in the clinic (Monday through Friday) for dosing and efficacy assessments. Take-home doses were provided for weekends. The primary study comparison was to assess the efficacy of buprenorphine and Suboxone individually against placebo. The percentage of thrice-weekly urine samples that were negative for non-study opioids was statistically higher for both Suboxone versus placebo (p<0.0001) and buprenorphine versus placebo (p<0.0001).
In a double-blind, double-dummy, parallel-group study comparing buprenorphine ethanolic solution to a full agonist active control, 162 subjects were randomized to receive the ethanolic sublingual solution of buprenorphine at 8 mg/day (a dose which is roughly comparable to a dose of Suboxone 12 mg/day), or 2 relatively low doses of active control, 1 of which was low enough to serve as an alternative to placebo, during a 3- to 10-day induction phase, a 16-week maintenance phase and a 7-week detoxification phase. Buprenorphine was titrated to maintenance dose by day 3; active control doses were titrated more gradually. Based on retention in treatment and the percentage of thrice-weekly urine samples negative for non-study opioids, buprenorphine was more effective than the low dose of the control in keeping heroin addicts in treatment and in reducing their use of opioids while in treatment. The effectiveness of buprenorphine 8 mg/day was similar to that of the moderate active control dose, but equivalence was not demonstrated.