Dosage: The recommended dose of SANBEPLATIN in previously untreated adult patients with normal kidney is 400 mg/m
2, as a single short term intravenous infusion over 15-60 minutes. Therapy should not be repeated until four weeks after the previous SANBEPLATIN course and/or the neutrophil count is at least 2,000 cells/mm
3 and the platelet count is at least 100,000 cells/mm
3. It is recommended that according to clinical circumstances the initial dosage may require reduction by 20-25% in patients with risk factors such as previous myelosuppressive therapy and poor performance status.
Determination of haematologic nadir by weekly blood counts during initial course is recommended for future dosage adjustment and scheduling SANBEPLATIN.
Combination Therapy: The optimal use of SANBEPLATIN in combination with other myelosuppressive agents requires dosage adjustments according to the regimen and schedule to be adopted.
Formula dosing: Because the pharmacokinetics and, ultimately, the pharmacodynamics of SANBEPLATIN are highly dependent on the status of renal function, fixed dosing based on body surface area has led to Carboplatin over-dosing or, especially, underdosing. Another approach for determining the initial dose of SANBEPLATIN using Calvert formula, a simple formula for calculating dosage based upon a patients glomerular filtration rate (GFR in mL/min) and SANBEPLATIN target area under the concentration versus time curve SANBEPLATIN (AUC in mg/mL.min). SANBEPLATIN dose could then be measured in milligrams. (See Equation 1 and Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
An approach in heavily pre-treated patients** receiving single-agent SANBEPLATIN, when there is the desire to target a particular platelet nadir, is the use of the Ergorin formula: See Equation 2.
Click on icon to see table/diagram/image
** Patients are considered heavily pre-treated if they have received any of the following: Mitomycin-C; a Nitrosurea; combination chemotherapy with Doxorubicin, Cyclophosphamide and Cisplatin; chemotherapy with ≥ 5 different agents; or radiotherapy ≥ 4500 rads to single port 20 x 20 cm or 1 field of therapy.
Impaired renal function: In patients with initial impaired renal function reduction of dosage of SANBEPLATIN may be required. Haematological nadirs and renal function should be monitored in these circumstances. The risk of bone marrow suppression may be increased in patients with creatinine clearance < 60 mL/min.
A suggested dosage schedule in patients with impaired renal function based in creatinine clearane is a follows: See Table 2.
Click on icon to see table/diagram/image
The dose should be adjusted according to patient condition. There are limited data in patients with creatinine clearance < 15 mL/min.
Use in children: Specific dosage recommendations cannot be made due to insufficient use in paediatrics at this time.
Administration: Preparation of SANBEPLATIN solution: Equipment containing aluminium components should be avoided. (See PRECAUTIONS)
SANBEPLATIN Injection: Is a ready to use solution containing 10 mg/mL SANBEPLATIN in water for injection. The solution maybe further diluted in glucose intravenous infusion 5% or Sodium Chloride Intravenous Infusion 0.9%.
Handling guidelines: Carboplatin should be prepared for administered only by professionals who have been trained in the safe use of the preparation.
The personnel carrying out these procedures should be adequately protected with clothing, gloves and eye shield.
Pregnant personnel are advised not to handle chemotherapeutic agents.
Contaminations: In the event of contact of with the skin or eyes, the affected area should be washed with copious amounts of water or normal saline. A bland cream may be used to treat transient stinging of skin. Medical advice should be sought if the eyes are affected.
In the event of a spillage, operators should use gloves and mop up the spilled material with a sponge kept in the area for that purpose. Rinse the area twice with water. Put all solutions and sponges into a plastic bag and then seal it. The bag should be prominently labelled with the words: "Cytotoxic Waste" or similar.
Disposal: Syringes, containers absorbent materials, solutions and any other material which has come into contact with Carboplatin should be placed in a thick plastic bag or other impervious container and incinerated at 1000°C or more.
Stability: The product and admixture contain no antimicrobial agent. In order to reduce microbiological contamination hazard, infusion should be commenced as soon as practicable after preparation.
The solution of Carboplatin should be kept at room temperature (25°C) and used within 8 hours.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image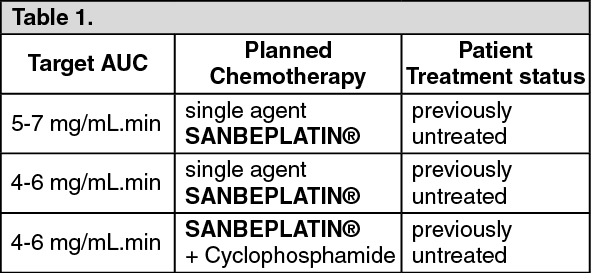 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image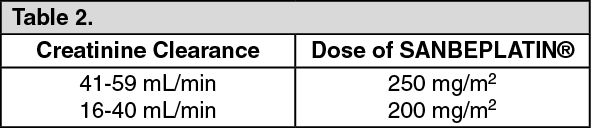 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
