Pharmacology: Pharmacodynamics: Dexmedetomidine is a potent and highly selective α
2-adrenoreceptor agonist with a broad range of pharmacologic properties. It provides sedation and analgesia without respiratory depression during which patients are arousable and cooperative. Additional sympatholytic properties include less anxiety, hemodynamic stability, blunting of stress hormone response and reduction of intraocular pressure.
The sedative actions of dexmedetomidine are believed to be mediated primarily by post-synaptic α
2-adrenoreceptors, which in turn act on inhibitory pertussis-toxin-sensitive G protein, thereby increasing conductance through potassium channels. The site of sedative effects of dexmedetomidine has been attributed to the locus ceruleus. The analgesic actions are believed to be mediated by a similar mechanism of action at the brain and spinal cord level.
Alpha
2 selectivity is demonstrated following low and medium doses given slowly. Alpha
2 and α
1-activity is seen following rapid administration or very high doses. Dexmedetomidine has no affinity for β-adrenergic, muscarinic, dopaminergic or serotonin receptors.
In clinical trials evaluating patients requiring intensive care, patients receiving dexmedetomidine reached desired levels of sedation, were less anxious and had a significant reduction in the need for analgesia. However, patients could be easily aroused, were cooperative and orientated, resulting in increased ease of patient management. In phase I studies in healthy volunteers, dexmedetomidine did not cause respiratory depression and demonstrated attenuation of the heart rate and blood pressure responses to stress. These effects were confirmed in phase III studies in intensive care patients.
Two phase III ICU sedation studies were conducted comparing the effects of dexmedetomidine HCl with placebo including propofol or midazolam as rescue medications for sedation. Results from these studies support the unique profile of dexmedetomidine HCl.
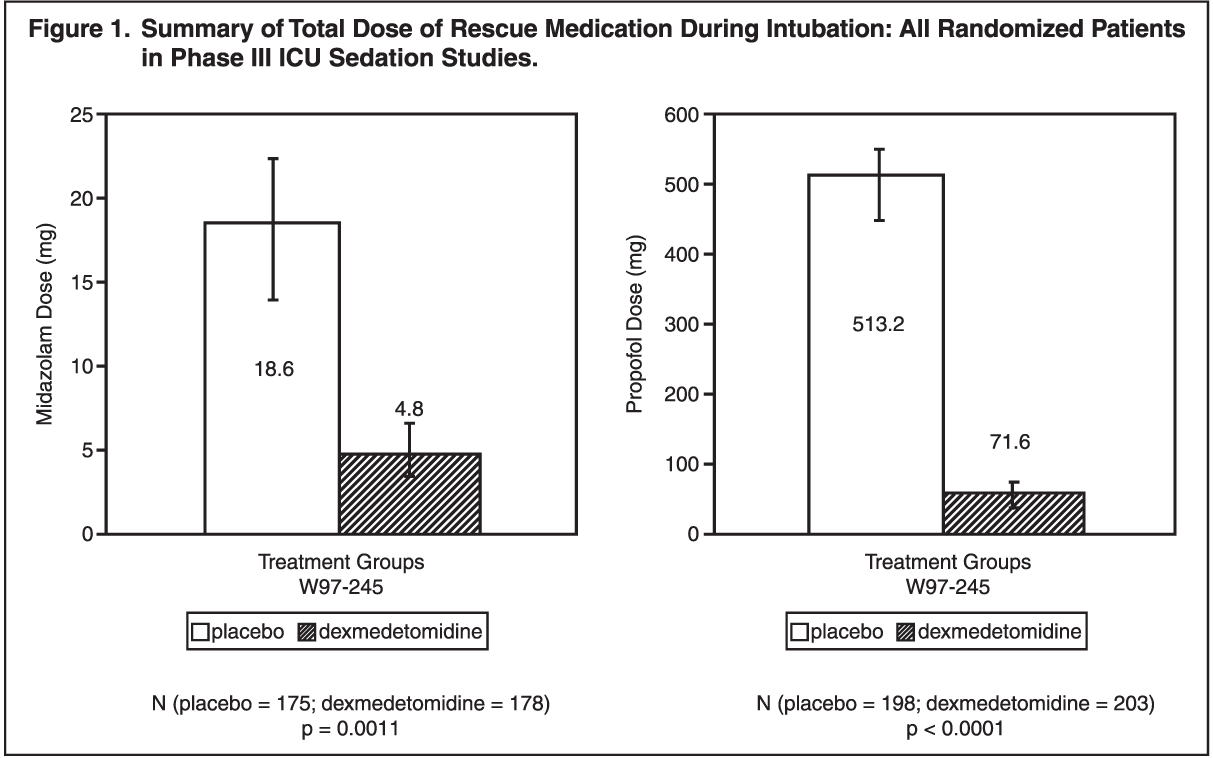
Sedation: Dexmedetomidine HCl-treated patients reached clinically indicated levels of sedation, as measured by Ramsay sedation scores, and were easily arousable and cooperative. Dexmedetomidine HCl-treated patients also required statistically significant less rescue sedative medication than placebo-treated patients. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In addition, at least 60% of dexmedetomidine HCl-treated patients required no midazolam or propofol to achieve clinically required levels of sedation, compared to approximately 60% of placebo-treated patients who required midazolam >4 mg or propofol >50 mg. (See Table 1.)
Click on icon to see table/diagram/image
Analgesia: Dexmedetomidine HCl-treated patients required statistically significantly less treatment with an analgesic (morphine) than placebo-treated patients in the intensive care setting. (See Figure 2.)
Click on icon to see table/diagram/image
Less Anxiety: Dexmedetomidine HCl-treated patients exhibited statistically less anxiety than placebo-treated patients. The mean percentage of the Ramsay assessments that equaled one (anxious, agitated or restless patient) for the dexmedetomidine HCl group (4%) was statistically significantly (p<0.0001) less than for the placebo group (7%).
Hemodynamic Stability: Dexmedetomidine HCl-treated patients exhibited lower blood pressure and heart rate values, attenuating stress-related increases in blood pressure and heart rate seen in placebo-treated patients. (See Figures 3-5.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional Studies: Reduction of Intraocular Pressure: Dexmedetomidine produced bilateral, dose-related decreases in intraocular pressure in rabbits when used topically unilaterally.
Clinical Trials: ICU Sedation: Dexmedetomidine HCl has been evaluated in 3 double-blind, placebo-controlled clinical trials in the surgical ICU involving 766 randomized patients. Of these, 387 received dexmedetomidine HCl. In these trials, dexmedetomidine was titrated to a desired level of sedation using a loading dose of 1 mcg/kg over 10 mins, followed by a maintenance infusion of 0.2-0.7 mcg/kg/hr. Doses as low as 0.05 mcg/kg/hr have been used with infusions up to 24 hrs. Results from these studies demonstrated a statistically significant reduction in the sedative medication and analgesia (morphine), as compared to the placebo group. At least 60% of dexmedetomidine HCl-treated patients required no midazolam or propofol to achieve clinically required levels of sedation, compared to approximately 60% of placebo-treated patients who required midazolam >4 mg or propofol >50 mg. Results also indicated significantly less anxiety, no respiratory depression and significantly increased ease of patient management, as compared to the placebo group.
Perioperative Studies: Dexmedetomidine HCl has been evaluated in 7 clinical trials involving a total of 1199 patients, with 761 receiving dexmedetomidine HCl. A loading dose followed by a maintenance infusion was administered to achieve target concentrations of 0.15, 0.3 or 0.6 ng/mL using continuous infusions of 15 min prior to anethesia induction and continued until determination of MAC response, the end of surgery, 1, 2, 6 or 12 hrs postoperatively. Dexmedetomidine HCl was well-tolerated during pre-, intra- and postoperative administration.
Pharmacokinetics: Following Precedex administration, dexmedetomidine HCl exhibits the following pharmacokinetic characteristics: Rapid distribution phase with a distribution half-life (t
½a) of about 6 min: terminal elimation half-life (t
½) approximately 2 hrs; steady-state volume of distribution (V
ss) approximately 118 L. Clearance has an estimated value of about 39 L/hr. The mean body weight associated with this clearance estimate was 72 kg. Dexmedetomidine HCl is eliminated almost exclusively by metabolism with 95% of a radiolabeled dose being excreted in the urine and 4% in the feces. The major excreted metabolites are glucuronides.
Dexmedetomidine HCl protein binding was assessed in the plasma of normal healthy male and female human subjects: The average binding was 94% and constant across the different concentrations tested. Protein binding was similar in males and females. The fraction of dexmedetomidine HCl that was bound to plasma proteins was statistically significantly decreased in subjects with hepatic impairment compared to healhty subjects.
The possibility of binding displacement of dexmedetomidine HCl by fentanyl, ketorolac, theophylline, digoxin and lidocaine was explored
in vitro, showing negligible change in the plasma protein binding of dexmedetomidine HCl.
The possibility of binding displacement of phenytoin, warfarin, ibuprofen, propranolol, theophylline and digoxin by dexmedetomidine HCl was explored
in vitro and none of these compounds appeared to be significantly displaced by dexmedetomidine HCl. Dexmedetomidine HCl is unlikely to cause clinically significant changes in the plasma protein binding of these medications.
Hepatic Impairment: In subjects with varying degrees of hepatic impairment (Child-Pugh class A, B or C), clearance values were lower than in healthy subjects. The mean clearance values for subjects with mild, moderate and severe hepatic impairment were 74%, 64% and 53%, of those observed in the normal healthy subjects, respectively. Mean clearances for free drug were 59%, 51% and 32%, of those observed in the normal healthy subjects, respectively.
Although dexmedetomidine HCl is dosed to effect, it may be necessary to consider dose reduction depending on the degree of hepatic impairment.
Renal Impairment: Dexmedetomidine HCl pharmacokinetics (C
max, T
max, AUC, t, CL and V
ss) were not different in subjects with severe renal impairment (CrCl <30 mL/min) compared to healthy subjects.
Gender: No difference in dexmedetomidine HCl pharmacokinetics due to gender was observed.
Geriatrics: The pharmacokinetic profile of dexmedetomidine HCl was not altered by age.
Pediatrics: The pharmacokinetic profile of dexmedetomidine HCl has not been studied in children.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image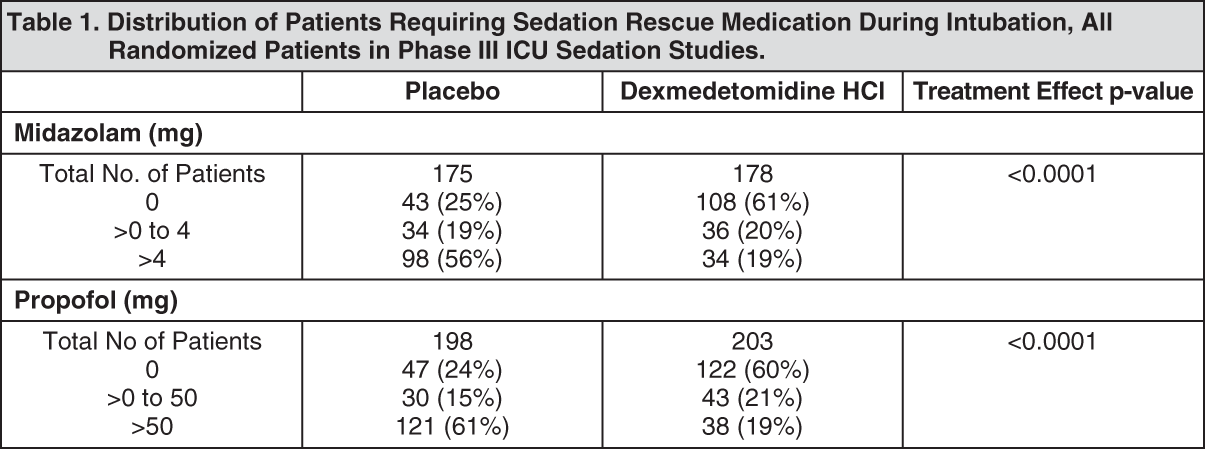 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image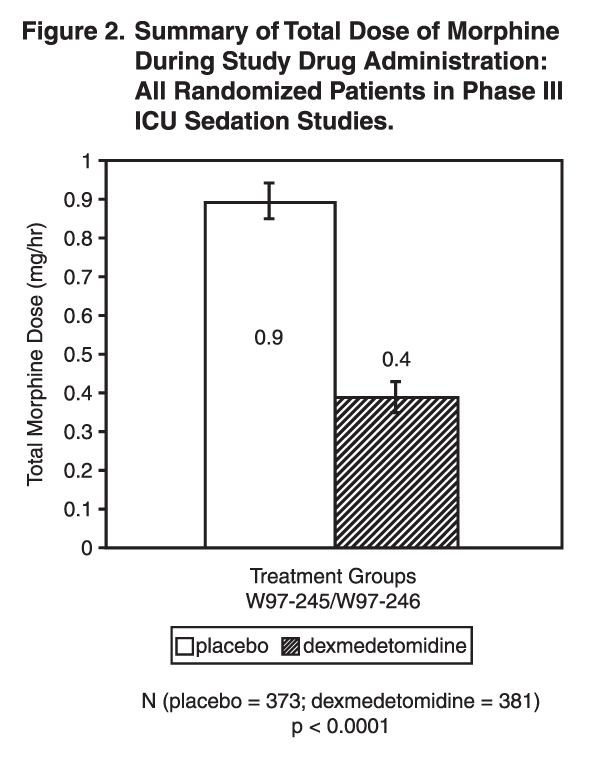 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image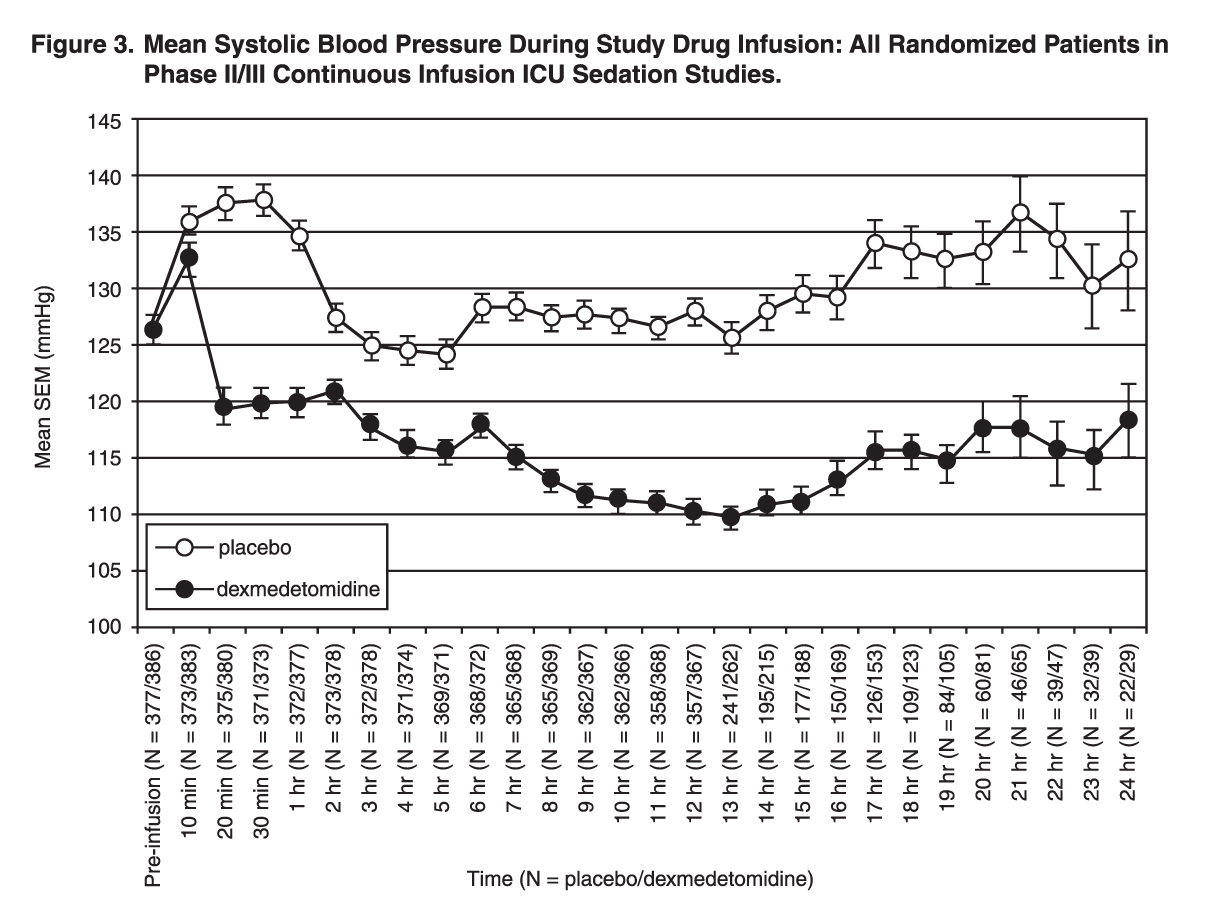 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image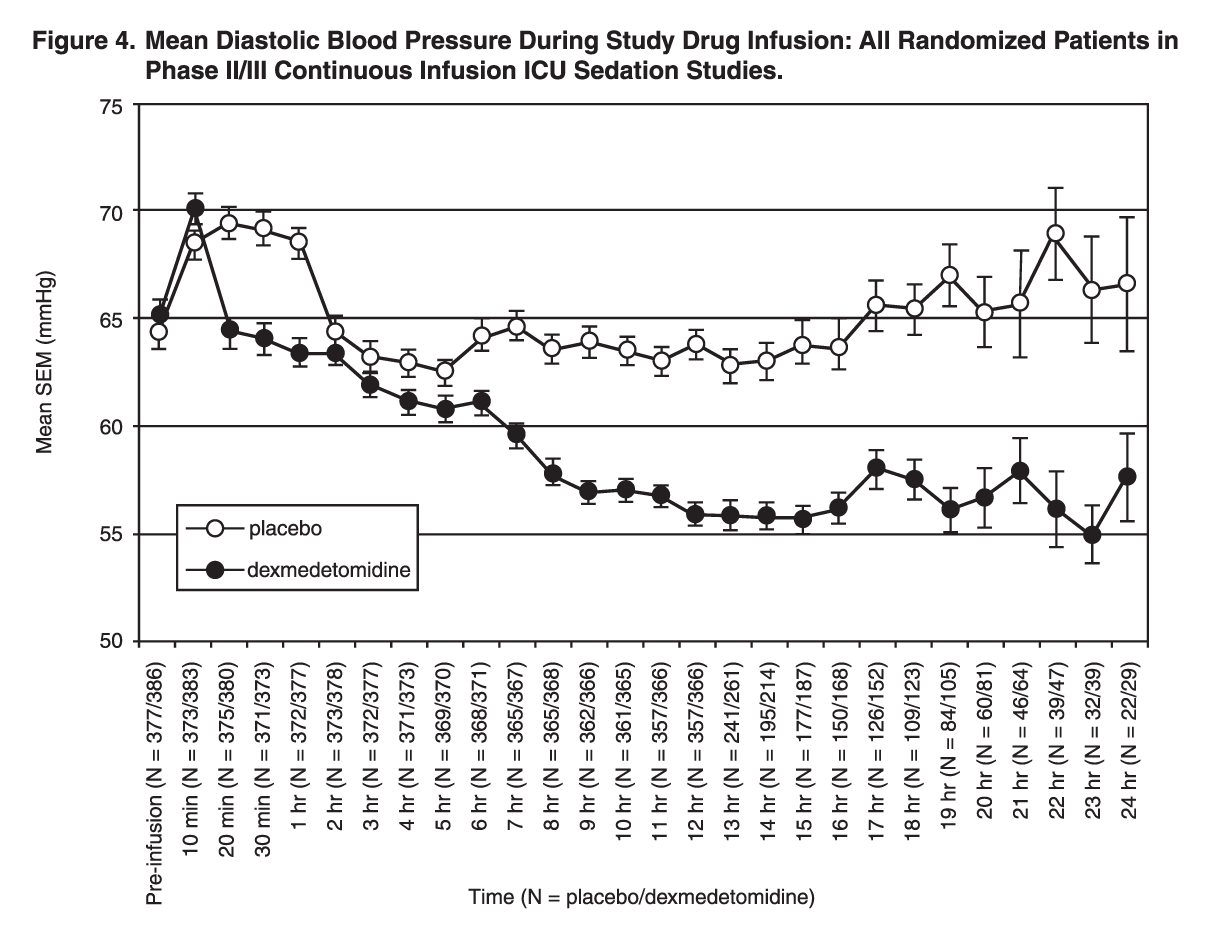 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image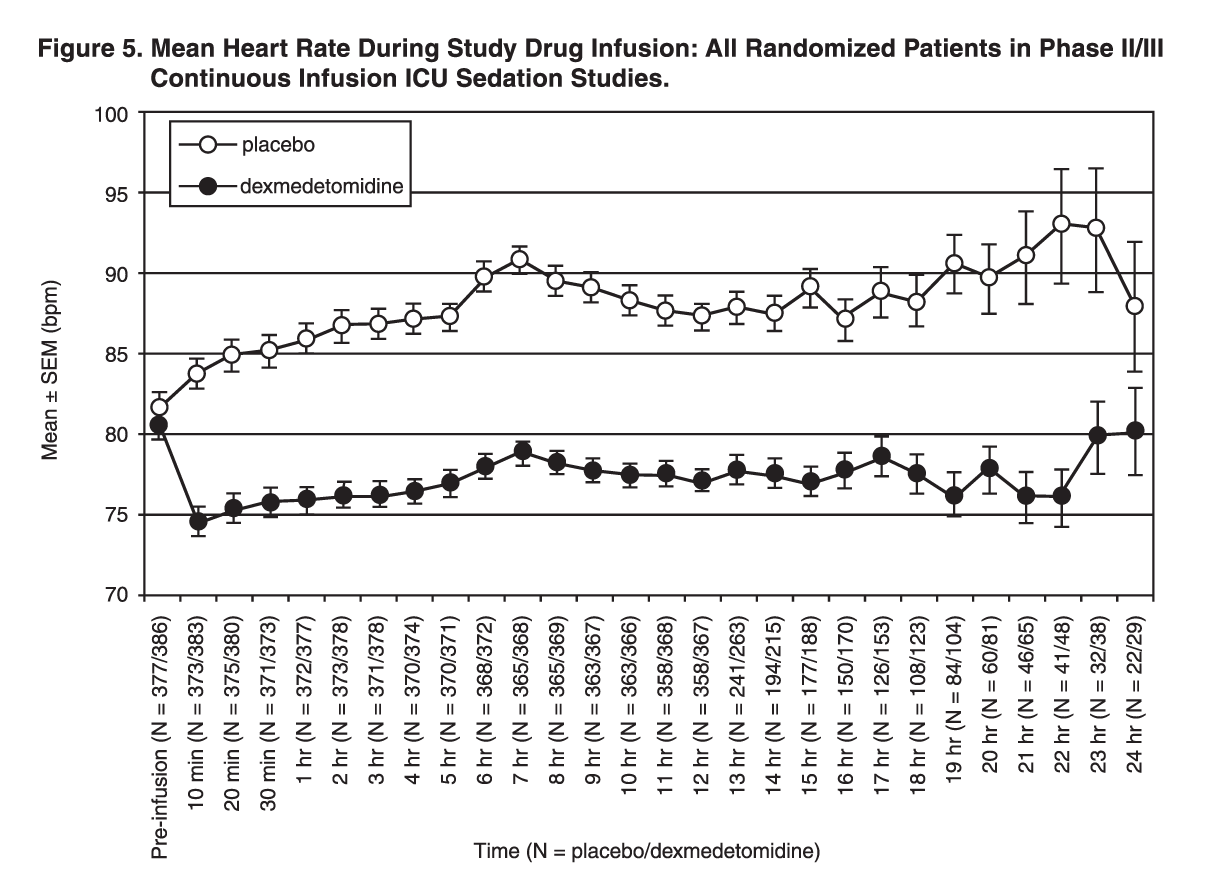 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
