Pharmacology: Antiplatelet Action: In vitro studies: Cilostazol inhibited platelet aggregation induced by ADP, collagen, arachidonic acid, adrenaline and thrombin in humans. The drug also inhibited shear stress-induced platelet aggregation.
Cilostazol inhibited ADP- and adrenaline-induced primary aggregation and exhibited a dispersing effect on human platelet aggregates induced by various aggregating agents.
Cilostazol inhibited thromboxane A
2 (TXA
2) production in activated human platelets.
Cilostazol inhibited the procoagulant activity of human platelets.
In vivo studies: Cilostazol inhibited ADP- and collagen-induced platelet aggregation when orally administered to beagle dogs and pigs.
The inhibitory effect of cilostazol on ADP-induced platelet aggregation was unchanged during repeated oral administration in rats.
Cilostazol prevented platelet aggregation induced by ADP, collagen, arachidonic acid, and adrenaline when orally administered to patients with chronic arterial occlusion or cerebral infarction.
The onset of cilostazol's platelet aggregation inhibitory effect was prompt in humans, and the effect persisted during repeated administration.
Following discontinuation of cilostazol administration, as the plasma concentration of the drug declined, platelet aggregability returned to baseline levels with no rebound phenomenon (no increase of platelet aggregation).
Antithrombotic Action: Cilostazol reduced mortality due to pulmonary embolism induced experimentally in mice by intravenous administration of ADP or collagen.
Cilostazol suppressed the progression of peripheral thrombotic circulatory insufficiency in the hind limbs induced by the intra-arterial injection of sodium laurate solution into the femoral artery of dogs.
Cilostazol inhibited thrombotic occlusion of prosthetic artificial grafts placed in the femoral artery of dogs.
Cilostazol inhibited electrical stimulation-induced thrombus formation in the carotid artery of pigs.
Cilostazol reduced the size of cerebral infarction induced by injection of arachidonic acid into the internal carotid artery of rabbits.
Cilostazol reduced the incidence of ischemic attacks in patients with transient ischemic attacks.
Vasodilating Action: Cilostazol inhibited KCl- and prostaglandin F2α-induced contraction of the isolated femoral, middle cerebral, and basilar arteries in dogs.
Cilostazol increased blood flow in the femoral, vertebral, common carotid, and internal carotid arteries in anesthetized dogs.
Cilostazol increased blood flow in the cerebral cortex in anesthesized dogs and cats.
Cilostazol increased blood flow in the cerebral cortex and hypothalamus in conscious rats.
Results of a plethysmographic study showed that cilostazol increased blood flow in the occluded ankle and calf region in patients with chronic arterial occlusion, and results of a thermographic plethysmographic study demonstrated that the drug induced an increase in skin temperature of the extremities and increased cutaneous blood flow in patients with chronic arterial occlusion.
Cilostazol increased cerebral blood flow in patients with ischemic cerebrovascular diseases, as determined by the xenon-inhalation method.
Effects on Vascular Smooth Muscle Cells: Cilostazol suppressed the proliferation of vascular smooth muscle cells in cultured human vascular smooth muscle.
Cilostazol suppressed intimal thickening of rat carotid arteries induced by intimal balloon injury.
Effects on Vascular Endothelial Cells: Cilostazol augmented NO production by cultured human endothelial cells.
Cilostazol suppressed injuries of cultured human endothelial cells.
Cilostazol suppressed the depletion of lactate dehydrogenase from cultured human endothelial cells stimulated with homocysteine or lipopolysaccharide.
Mechanism of Action: Experiments in rabbits showed that cilostazol suppressed serotonin release from platelets without affecting serotonin and adenosine uptake by platelets. The drug inhibited platelet aggregation induced by thromboxane A
2 (TXA
2).
Cilostazol exerts its antiplatelet and vasodilating actions by selectively inhibiting PDE3 (cGMP-inhibited PDE) in platelets and vascular smooth muscle.
Cilostazol's antiaggregation effect in human platelets was augmented in the presence of vascular endothelial cells
25 or prostaglandin E
1.
Cilostazol's antiaggregation effect in canine platelets was augmented in the presence of prostaglandin I
2 or adenosine.
Pharmacokinetics: Plasma Concentration: Following single oral administration of Cilostazol 100 mg to fasted normal healthy individuals, the plasma cilostazol concentration promptly rose to a maximum level of 763.9 ng/mL in 3 hours. The plasma half life of the drug estimated using a two-compartment model was 2.2 hours in the α-phase and 18.0 hours in the β-phase. Two metabolites were found to be active: OPC-13015 (dehydrated metabolite) and OPC-13213 (hydroxylated metabolite).
Administration of a single oral dose of cilostazol 50 mg in a fed state was associated with a 2.3-fold increase in C
max and a 1.4-fold increase in AUC
inf compared with administration in fasted state.
When PLETAAL SR capsule was administered orally to healthy adult male subjects at multiple dose of 200 mg as cilostazol in fasting condition for 5 days, the following pharmacokinetic parameters were obtained at steady state. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following single oral administration of cilostazol to healthy adult male subjects, two metabolites were found to be active: OPC-13015 (dehydrated metabolite) and OPC-13213 (hydroxylated metabolite).
Metabolizing Enzymes: Cilostazol is extensively metabolized by hepatic cytochrome P-450 enzymes, mainly CYP3A4, and to a lesser extent, CYP2D6 and CYP2C19 (
in vitro).
Protein Binding: Cilostazol: Greater than 95% (equilibrium dialysis
in vitro, 0.1-6 μg/mL).
Active metabolite OPC-13015H 97.4% (ultrafiltration
in vitro, 1 μg/mL).
Active metabolite OPC-13213: 53.7% (ultrafiltration
in vitro, 1 μg/mL).
Pharmacokinetics in Patients with Renal Impairment (Outside Japan): Repeated oral administration of cilostazol at a daily dose of 100 mg for 8 days in patients with severe renal impairment showed decreases (C
max by 29% and AUC by 39%) in plasma concentrations of cilostazol and marked increases (C
max by 173% and AUC by 209%) in plasma concentrations of the active metabolite OPC-13213 compared with administration in normal healthy individuals. However, the concentrations of cilostazol and OPC-13213 in patients with mild to moderate renal impairment were similar to those in normal healthy individuals.
Pharmacokinetics in Patients with Hepatic Impairment (Outside Japan): Plasma concentrations of cilostazol following single oral administration of cilostazol 100 mg in patients with mild to moderate hepatic impairment were similar (C
max decreased by 7%, AUC increased by 8%) to those in normal healthy individuals.
Drug Interactions (Outside Japan): Cilostazol 100 mg did not inhibit either the metabolism or pharmacological effects of R- and S-warfarin when administered in combination with a single dose of warfarin 25 mg.
Coadministration of a single dose of cilostazol 100 mg and erythromycin 500 mg tid after 7-day treatment with erythromycin 500 mg tid increased cilostazol C
max by 47% and AUC by 87% compared with administration of cilostazol alone.
Coadministration of a single dose of ketoconazole 400 mg with a single dose of cilostazol 100 mg increased cilostazol C
max by 94% and AUC by 129% compared with administration of cilostazol alone. (The oral formulation of the azole antimycotic ketoconazole has not yet been approved in Japan.)
Coadministration of diltiazem hydrochloride 180 mg with a single dose of cilostazol 100 mg increased cilostazole C
max by 34% and AUC by 44% compared with administration of cilostazol alone.
Administration of a single dose of cilostazol 100 mg with 240 mL of grapefruit juice increased cilostazol C
max by 46% and AUC by 14% compared with administration of cilostazol without grapefruit juice.
Coadministration of cilostazol 100 mg and omeprazole 40 mg qd after 7-day treatment with omeprazole 40 mg qd increased cilostazol C
max by 18% and AUC by 26% compared with administration of cilostazol alone.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image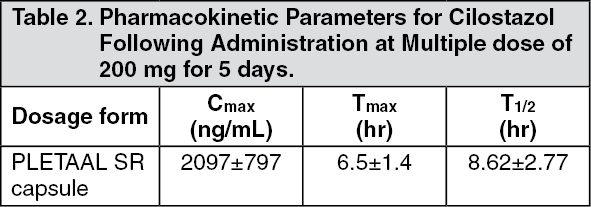 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
