Epilepsy: Since Gabapentin was most often administered in combination with other antiepileptic agents. It was not possible to determine which agent(s), if any, was associated with adverse events.
Incidence in Controlled Adjunctive Therapy Clinical Trials: Lists treatment-emergent signs and symptoms that occurred in at least 1% of patients with partial seizure participating in placebo-controlled adjunctive therapy studies. In these studies, either gabapentin or placebo was added to the patient's current antiepileptic drug therapy.
Adverse events were usually reported as mild to moderate:
Body as a Whole: abdominal pain, back pain, fatigue, fever, headache, viral infection.
Cardiovascular: vasodilation.
Digestive System: constipation, dental abnormalities, diarrhea, increased appetite, mouth or throat dry, nausea and/or vomiting, dyspepsia.
Hematologic and Lymphatic: leucopenia, WBC decreased.
Metabolic and Nutritional: peripheral edema, weight increase.
Musculoskeletal system: fracture, myalgia.
Nervous system: amnesia, ataxia, confusion, coordination abnormal, depression, dizziness, dysarthria, emotional lability, insomnia, nervousness, nystagmus, somnolence, thinking abnormal, tremor, twitching.
Respiratory system: coughing, pharyngitis, rhinitis.
Skin and Appendages: abrasion, acne, pruritus, rash.
Special Senses: amblyopia, diplopia.
Urogenital system: impotence.
Other Adverse Events:
Body as A Whole: asthenia, malaise, facial edema.
Cardiovascular System: hypertension.
Digestive System: flatulence, anorexia, gingivitis.
Hemic, Limphatic Systems: purpura most often described as bruises resulting from physical trauma.
Musculoskeletal System: arthralgia.
Nervous System: vertigo, hyperkinesia, increased, decreased or absent reflexes, parasthesia, anxiety, hostility.
Respiratory System: pneumonia.
Urogenital System: urinary tract infection.
Special Senses: abnormal vision most often described as a visual disturbance.
Geriatric Use: Side effects reported among these patients did not differ in kind from those reported in younger individuals. For patients with compromised renal function, the dosage should be adjusted. (See DOSAGE & ADMINISTRATION).
Pediatric Use: The most commonly observed adverse events reported with the use of Gabapentin in combination with other antiepileptic drugs in children 3 to 12 years of age, not seen in equal frequency among placebo-treated patients, were viral infection, fever, nausea and/or vomiting, and somnolence.
Body system/Adverse Event:
Body as a Whole: viral infection, fever, weight increase, fatigue.
Digestive system: nausea and/or vomiting.
Nervous system: somnolence, hostility, emotional lability, dizziness, hyperkinesia.
Respiratory system: bronchitis, respiratory infection.
Other Adverse Events: pharyngitis, upper respiratory infection, headache, rhinitis, convulsions, diarrhea, anorexia, coughing, and otitis media.
Withdrawal from Treatment Due to Adverse Events: Adjunctive Therapy: The most frequently occurring events that contributed to discontinuation of Gabapentin included somnolence, ataxia, dizziness, fatigue, nausea and/or vomiting. Almost all participants had multiple complaints, none of which could be characterized as primary.
Pediatric: The adverse event most commonly associated with withdrawal in children were somnolence, hyperkinesia, and hostility.
Neuropathic Pain
Body system/Adverse Event:
Body as a whole: abdominal pain, accidental injury, asthenia, back pain, flu syndrome, headache, infection, pain.
Digestive system: constipation, diarrhea, dry mouth, dyspepsia, flatulence, nausea, vomiting.
Metabolic and Nutritional: peripheral edema, weight gain.
Nervous system: abnormal gait, amnesia, ataxia, confusion, dizziness, hypesthesia, somnolence, thinking abnormal, tremor, vertigo.
Respiratory system: dyspnea, pharyngitis.
Skin and Appendages: rash.
Special senses: amblyopia.
Post-marketing Experience: Sudden, unexplained deaths have been reported where a causal relationship to treatment with Gabapentin has not been established.
Acute kidney failure, allergic reaction including urticaria, alopecia, angioedema, blood glucose fluctuations in patients with diabetes, breast hypertrophy, chest pain, elevated liver function test (LFTs), erythema multiforme, generalized edema, gynecomastia, hallucinations, hepatitis, jaundice, movement disorders such as choreoathetosis, dyskinesia, and dystonia, myoclonus, palpitation, pancreatitis, Stevens-Johnson syndrome, thrombocytopenia, tinnitus, and urinary incontinence.
Adverse events following the abrupt discontinuation of Gabapentin have also been reported. The most frequently reported events were anxiety, insomnia, nausea, pain, and sweating.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image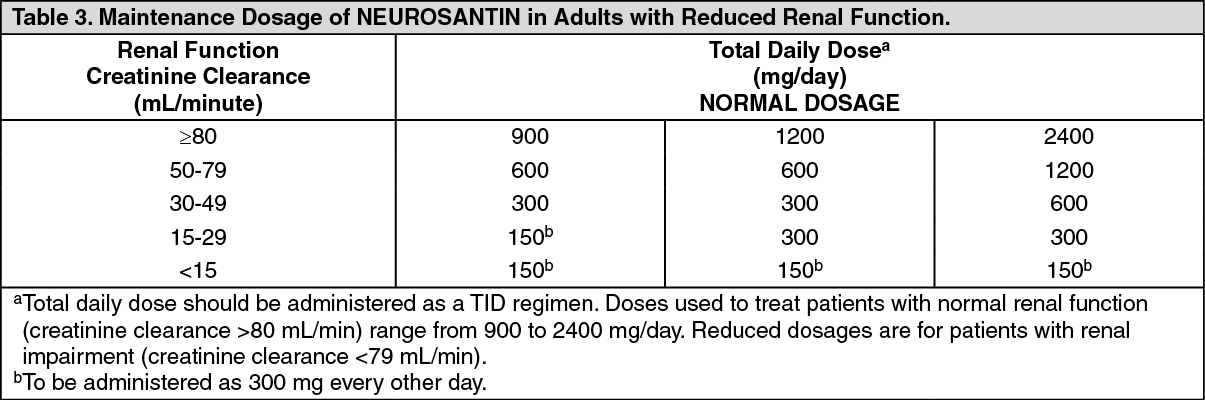 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
