Each 250 mL infusion solution contains: Moxifloxacin hydrochloride equivalent to Moxifloxacin 400 mg.
Pharmacology: Moxifloxacin is a fluoroquinolone antibacterial. In vitro, moxifloxacin has been shown to have activity against a wide range of Gram-positive and Gram-negative organisms.
The bacterial action of moxifloxacin results from the inhibition with topoisomerase II (DNA gyrase) and IV. Topoisomerases are essential enzymes which play a crucial part in the replication, transcription and repair of bacterial DNA. Topoisomerase IV is also known to influence bacterial chromosome division.
Intravenous moxifloxacin is only for patients that cannot take oral administration or have been clinically proven have to take parenteral administration. Moxifloxacin infusion 400 mg is indicated for the treatment in adults (≥18 years of age) for the following bacterial infections: Acute exacerbations of chronic bronchitis.
Community acquired pneumonia.
Acute bacterial sinusitis (adequately diagnosed).
Complicated skin and skin structure infections which require initial parenteral therapy; followed by oral; in patients who are intolerance to alternative agents (especially penicillin allergy), and when caused by organisms known to be susceptible to moxifloxacin.
Complicated intra-abdominal infections due to polymicrobial infections in patients who are intolerance to alternative agents; caused by organisms known to be susceptible to moxifloxacin.
Moxifloxacin infusion 400 mg is indicated for the treatment of the above infections if they are caused by bacteria susceptible to moxifloxacin.
Consideration should be given of official guidance on the appropriate use of antibacterial agents.
Moxifloxacin may only be used on prescription and under the constant supervision of doctor.
Dosage: The recommended dose for moxifloxacin is 400 mg once daily.
No adjustment of dosage is required in elderly patients.
Efficacy and safety in children and adolescents have not been established.
No dosage adjustment is required in patients with any degree of renal impairment (including creatinine clearance ≤ 30 mL/minute/1.73m2).
For treatment of complicated intra-abdominal infections and complicated skin and skin structure infections requiring initial intravenous therapy followed by oral administration of 400 mg moxifloxacin tablet.
Administration: The infusion solution should be infused intravenously over 1 hour. Rapid intravenous infusion of moxifloxacin should be avoided.
It can be administered directly or via a T-tube together with compatible infusion solutions.
If moxifloxacin infusion solution is to be given with another drug, each drug should be given separately.
Moxifloxacin intravenous solution should be in inspected visually for particulate matter prior to administration and should be discarded if visible particulates are evident. Only clear solutions are to be used.
Duration of treatment: The duration of treatment should be determined by the severity of the indication of clinical response. The following are general recommendations: Acute exacerbation of chronic bronchitis: 5-10 days.
Community acquired pneumonia: 10 days.
Acute sinusitis: 7 days.
Complicated skin and skin structure infections: 7-21 days (sequential intravenous/oral therapy).
Complicated intra-abdominal infections: 5-14 days (sequential intravenous/oral therapy).
In patients with complicated skin and skin structure infections, the mean duration of intravenous therapy was approximately 6 days with overall mean treatment duration of approximately 13 days.
Moxifloxacin can be administered intravenously as initial intravenous administration, followed by oral tablet administration when allowed by the patient's condition. The recommended dose (400 mg once daily) and duration of therapy for indication being treated should not be exceeded. Intravenous therapy may be limited for up to 2-5 days in therapy in the very ill patients and should be changed to oral therapy whenever possible as determined by the physician.
There is no experience with moxifloxacin in overdose. No specific countermeasures after accidental overdosage are recommended. General symptomatic therapy should be initiated.
Patients with known hypersensitivity to any component of the infusions or other quinolones.
Pregnancy and lactation.
Patients below 18 years of age.
Patients with a history of tendon disease/disorder related to quinolones treatment.
Patients with congenital or documented acquired QT prolongation.
Patients with electrolyte disturbances, particularly in hypokalemia.
Patients with clinically relevant bradycardia.
Patients with clinically relevant heart failure with reduced left-ventricular ejection fraction.
Patients with previous history of symptomatic arrhythmias.
Fluoroquinolone is associated with an increased risk of tendinitis and tendon rupture in all ages. This risk is further increased in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with renal,heart or lung transplants.
Tendon inflammation and rupture may occur with quinolone therapy, particularly in elderly patients and in those treated concurrently with corticosteroids. At the first sign of pain or inflammation, patients should discontinue treatment with moxifloxacin and rest the effected limb(s).
Moxifloxacin, as with some other quinolones and macrolides, has been shown to prolong the QT interval. Since there is only limited information available on patients who may be predisposed to develop cardiac arrhythmias associated with QT prolongation, moxifloxacin should be used with caution in patients using concomitant medication that can reduce potassium and magnesium level. QT prolongation may lead to an increased risk for ventricular arrhythmias including torsades de pointes.
If signs of cardiac arrhythmia occur during treatment with moxifloxacin, treatment should be stopped and an ECG should be performed.
In women and elderly patients who, both may be more susceptible to QT-prolonging drugs. As women tend to have a longer baseline QT interval compared with men, they may be more sensitive to QT prolonging medications. Elderly patients may also be more susceptible to drug-associated effects on the QT interval. -
Quinolones are known to trigger seizures. Moxifloxacin should be used with caution in patients with central nervous system disorders which may predispose to seizures or lower the seizure threshold.
In some instances, the hypersensitivity and allergic reactions already occur after the first time administration and the doctor should be informed immediately. Anaphylactic reactions in very rare case instances can progress to a life-threatening shock, in some instances after the first administration. In these cases the treatment with moxifloxacin has to be discontinued and medical treatment (e.g., treatment for shock) is required.
Cases of bullous skin reactions like Steven-Johnson syndrome or toxic epidermal necrolysis have been reported with moxifloxacin. Patients should be advised to contact their doctor immediately prior to continuing treatment if skin and/or mucosa I reactions occur.
Cases of fulminant hepatitis potentially leading to liver failure (including fatal cases) have been reported with moxifloxacin. Patients should be to contact their doctor immediately prior continuing treatment if symptoms related to liver failure occur.
Due to limited clinical data, the use of moxifloxacin is also not recommended in patients with severe hepatic impairment (Child Pugh C).
Liver function tests/investigations should be performed in cases where indications of liver dysfunction occur.
Pseudomembranous colitis has been reported with the use of board-spectrum antibiotics; therefore, it is important to consider this diagnosis in patients who develop serious diarrhea during or after the use of moxifloxacin. Drugs inhibiting peristalsis are contraindicated in patients who develop serious diarrhea.
Moxifloxacin should be used with caution in patients with myasthenia gravis because the symptoms can be exacerbated.
Patients with a family history of or actual defects in glucose-6-phospate dehydrogenase (G6PD) deficiency are prone to hemolytic reactions when treated with quinolones. Therefore, moxifloxacin should be used with caution in these patients.
In patients for whom sodium intake is of medical concerns (patients with congestive heart failure, renal failure, nephrotic syndrome, etc.) the additional sodium load of the solution for infusion should be taken into account.
Quinolones have been shown to cause photosensitivity reactions. However, studies have been shown that moxifloxacin has no substantive potential to induce photosensitivity. Nevertheless, patients should be advised to avoid exposure to either UV irradiation or extensive sunlight during treatment with moxifloxacin.
If vision becomes impaired or any effects on the eyes are experienced, an eye specialist should be consulted immediately.
For patients with complicated pelvic inflammatory disease (E.G., associated with a tuba-ovarian or pelvic abscess), for whom an intravenous treatment is considered necessary, treatment with moxifloxacin 400 mg film-coated tablet is not recommended.
Use in Pregnancy and Lactation: The safety of use of moxifloxacin in human pregnancy has not been evaluated. Preclinical data indicates that moxifloxacin passes into milk. Therefore, the use of moxifloxacin in pragnancy and lactation is contraindicated.
The safety of use of moxifloxacin in human pregnancy has not been evaluated. Preclinical data indicates that moxifloxacin passes into milk. Therefore, the use of moxifloxacin in pregnancy and lactation is contraindicated.
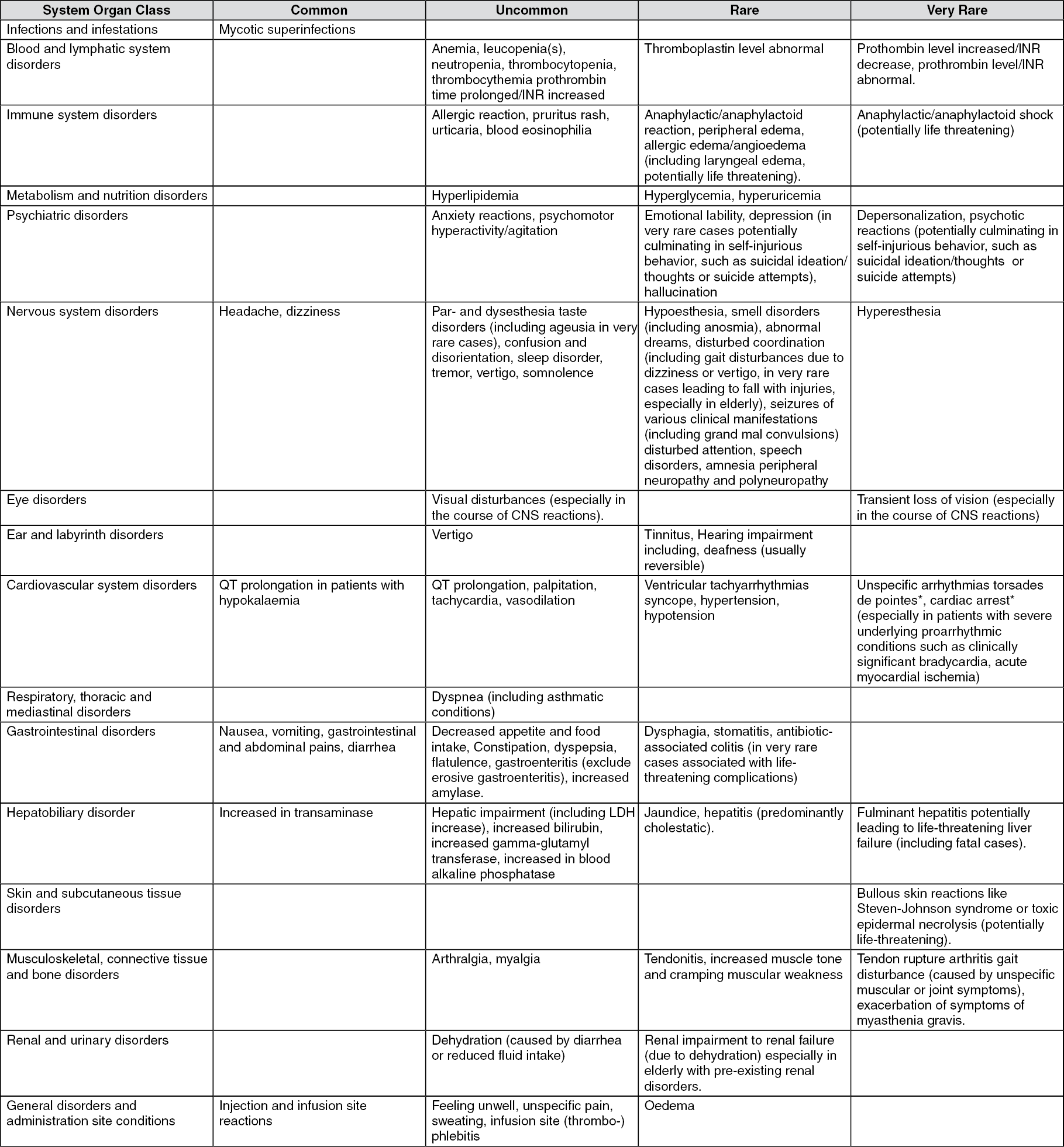
The adverse reactions as follows are sorted by frequency grouping (common, uncommon, rare, and very rare). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Moxifloxacin should be administered at least 4 hours before or 8 hours after antacids that contain aluminum or magnesium, didanosine tablets, sucralfate and agents containing iron or zinc. Transient increase in digoxin concentrations may occur; this is not considered clinically important. Dosage adjustment of moxifloxacin or digoxin is not necessary.
No clinically relevant interaction was seen between glibenclamide and moxifloxacin.
Concomitant use of drugs that induce bradycardia or hypokalemia or drugs which induce QT prolongation (neuroleptic, certain anti-infective agents [some antimalarials, azole antimycotics, macrolides], certain antihistaminic [terfenadine, astemizole], cisapride) should be considered carefully. Antiarrhythmic drugs class IA (such as quinidine and procainamide) and III (such as amiodarone and sotalol) are contraindicated. No interactions have occurred following concomitant administration of moxifloxacin with: warfarin, ranitidine, probenecid, oral contraceptives or theophylline. Cases of increased anticoagulant activity have been reported in patients receiving anticoagulants concurrently with antibiotics, including moxifloxacin. After intravenous drug administration, charcoal only slightly reduces systemic exposure to moxifloxacin in cases of overdosage.
Store at temperature below 30°C. Protect from light.
Do not store the infusion solution in a refrigerator.
J01MA14 - moxifloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Moxivar infusion 400 mg/250 mL
1's (Rp187,000/boks)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
