GEFITERO Film coated tablet 250 mg, each film coated tablet contains Gefitinib 250 mg.
Pharmacotherapeutic group: Antineoplastic, protein kinase inhibitors. ATC code: L01XE02.
Pharmacology: Pharmacodynamics: Gefitinib is a selective inhibitor of the epidermal growth factor receptor (EGFR) tyrosine kinase, commonly expressed in solid human tumours of epithelial origin. Inhibition of EGFR tyrosine kinase activity inhibits tumour growth, metastasis and angiogenesis and increases tumour cell apoptosis.
Patients that have never smoked, have adenocarcinoma histology, are female gender or are of Asian ethnicity, are more like to benefit from treatment with GEFITERO. These clinical characteristics are also associated with a higher rate of EGFR mutation positive tumours.
Pharmacokinetics: This study was designed as an open label, balanced, randomized, two-treatment, two-sequence, two-period, single oral dose, crossover bioequivalence study in normal, healthy adult human male subjects under fasting conditions. The study was conducted following an oral administration of one tablet 250 mg of the test drug or one tablet 250 mg of the product drug.
Based on the pharmacokinetic parameters of Gefitinib (N = 53), geometric least squares means for Test drug and Reference drug showed: Cmax values were 188.861 and 174.723, respectively; AUC0-96 values were 5650.393 and 5302.900, respectively.
Relative bioavailability results for Gefitinib (N = 53) were as following : The 90% Confidence Intervals for the ratio of geometric least squares means was found to be 96.57 - 120.98% for Cmax and 100.40 - 113.08% for AUC0-96. Intra subject CV (%) of Cmax and AUC0-96 for Gefitinib were 35.7 and 18.4%, respectively.
Conclusion: These results showed that 250 mg Gefitinib film coated tablet was bioequivalent to the reference product.
Resistance: Most NSCLC tumors with sensitizing EGFR kinase mutations eventually develop resistance to Gefitinib treatment with a median time to disease progression of 1 year. In about 60% of cases, resistance is associated with a secondary T790M mutation for which T790M targeted EGFR TKIs may be considered as a next line treatment option. Other potential mechanism of resistance have been reported following treatment with EGFR signal blocking agents including bypass signaling such as HER2 and MET gen amplification and PIK3CA mutations. Phenotypic switch to small cell lung cancer has also been reported.
GEFITERO is indicated for the naïve treatment of patients with locally advanced or metastatic Non Small Cell Lung Cancer (NSCLC) who have activating mutations of the EGFR TK (see PRECAUTIONS).
GEFITERO is indicated for the treatment of patients with locally advanced or metastatic Non-Small Cell Lung Cancer (NSCLC) who have activating mutations of the EGFR TK, who have previously received chemotherapy or who are not suitable for chemotherapy.
Treatment with GEFITERO should be initiated and supervised by a physician experienced in the use of anticancer therapies.
The recommended dose of GEFITERO is one 250 mg tablet once a day, taken with or without food. If a dose of GEFITERO is missed, it should be taken as soon as the patient remembers. If it is less than 12 hours to the next dose, the patient should not take the missed dose. Patients should not take a double dose (two doses at the same time) to make up for a forgotten dose.
Where dosing a whole tablet is not possible, such as patients who are only able to swallow liquids, tablets may be administered as a dispersion in water. The tablet should be dropped into half a glass of drinking water (non-carbonated), without crushing, and the glass stirred until the tablet has dispersed (approximately 15 minutes) and the contents subsequently drunk immediately. The glass should be rinsed with a further half glass of water and the contents drunk. The liquid can also be administered via a nasogastric tube.
GEFITERO is not recommended for use in children or adolescents as safety and effectiveness in these patient populations has not been studied.
No dosage adjustment is required on the basis of patient age, body weight, gender, ethnicity or renal function or in patients with moderate to severe hepatic impairment due to liver metastases.
Dosage adjustment: Patients with poorly tolerated diarrhea or skin adverse drug reactions may be successfully managed by providing a brief (up to 14 days) therapy interruption followed by reinstatement of the 250 mg dose (see ADVERSE REACTIONS).
There is no specific treatment in the event of overdose of Gefitinib. Adverse reactions associated with overdose should be treated symptomatically; in particular severe diarrhea should be managed as clinically indicated. In phase I clinical trials, a limited number of patients were treated with daily doses of up to 1000 mg. An increase of frequency and severity of some adverse reactions was observed, mainly diarrhea and skin rash. In one study a limited number of patients were treated weekly with doses from 1500 mg to 3500 mg. In this study Gefitinib exposure did not increase with increasing dose, adverse events were mostly mild to moderate in severity, and were consistent with the known safety profile of Gefitinib.
Known severe hypersensitivity to the active substance or to any of the excipients of this product.
When considering the use of GEFITERO for the naïve treatment of patients with locally advanced or metastatic NSCLC, it is recommended that EGFR mutation assessment of the tumour tissue is attempted for all patients. When assessing the mutation status of a patient it is important that a well-validated and robust methodology is chosen to minimize the possibility of false negative or false positive determinations. Tumour sample which are used for the diagnosis of advanced NSCLC are preferred sample type for EGFR mutation testing. A tumour sample should be collected and tested where possible. If a tumour sample is not available or evaluable, then circulating tumour DNA (ctDNA) obtained from a blood (plasma) sample may be used. Only robust, reliable, sensitive test(s) with demonstrated utility on ctDNA should be used for the determination of EGFR mutation status of ctDNA. EGFR mutations identified in ctDNA are highly predictive of EGFR mutation positive tumours). However it is not always possible to detect EGFR mutations using this sample type.
Interstitial Lung Disease (ILD), which may be acute in onset, has been observed in 1,3% of patients receiving Gefitinib, and some cases have been fatal (see ADVERSE REACTIONS).
Patients with concurrent idiopathic pulmonary fibrosis/interstitial pneumonia/pneumoconiosis/ radiation pneumonia/drug-induced pneumonia have been observed to have an increased rate of mortality from this condition. If patients present with worsening of respiratory symptoms such as dyspnea, cough and fever, GEFITERO should be interrupted and prompt investigation initiated. If ILD is confirmed, GEFITERO should be discontinued and the patient treated appropriately.
Patients with NSCLC receiving Gefitinib or chemotherapy who were followed up for 12 weeks, the following risk factors for developing ILD (irrespective of whether the patient received Gefitinib or chemotherapy) were identified: Smoking, poor performance status (PS ≥ 2), CT scan evidence of reduced normal lung (≤ 50%), recent diagnosis of NSCLC (< 6 months), pre-existing ILD, older age (≥ 55 years old) and concurrent cardiac disease. An increase risk of ILD on Gefitinib relative to chemotherapy was seen predominantly during the first 4 weeks of treatment; thereafter the relative risk was lower. Risk of mortality among patients who developed ILD on Gefitinib or chemotherapy was higher in patients with the following risk factors: Smoking, CT scan evidence of reduced normal lung (≤ 50%), pre-existing ILD, older age (≥ 65 years old), and extensive areas adherent to pleura (≥ 50%).
Liver function abnormalities (including increases in alanine aminotransferase, aspartate aminotransferase, bilirubin) have been observed (see ADVERSE REACTIONS), uncommonly presenting as hepatitis. There have been isolated reports of hepatic failure which in some cases led to fatal outcomes. Therefore, periodic liver function testing is recommended. GEFITERO should be used cautiously in the presence of mild to moderate changes in liver function. Discontinuation should be considered if changes are severe. Impaired liver function due to cirrhosis has been shown to lead to increased plasma concentrations of Gefitinib.
Cerebrovascular events have been reported. A relationship with GEFITERO has not been established.
Substances that are inducers of CYP3A4 activity may increase metabolism and decrease Gefitinib plasma concentrations. Therefore, co-medication with CYP3A4 inducers (e.g. Phenytoin, Carbamazepine, Rifampicin, Barbiturates or St. John's Wort) may reduce efficacy.
International Normalized Ratio (INR) elevations and/or bleeding events have been reported in some patients taking Warfarin (see INTERACTIONS). Patients taking Warfarin should be monitored regularly for changes in Prothrombin Time (PT) or INR.
Drugs that cause significant sustained elevation in gastric pH may reduce plasma concentrations of Gefitinib and therefore may reduce efficacy (see INTERACTIONS).
Patients should be advised to seek medical advice promptly in the event of developing: Severe or persistent diarrhea, nausea, vomiting or anorexia. These symptoms should be managed as clinically indicated (see ADVERSE REACTIONS).
Patients presenting with signs and symptoms suggestive of keratitis such as acute or worsening: Eye inflammation, lacrimation, light sensitivity, blurred vision, eye pain and/or red eye should be referred promptly to an ophthalmology specialist. If a diagnosis of ulcerative keratitis is confirmed, treatment with GEFITERO should be interrupted, and if symptoms do not resolve, or recur on reintroduction of GEFITERO, permanent discontinuation should be considered.
Radiation in pediatric patients, newly diagnosed with brain stem glioma or incompletely resected supratentorial malignant glioma of Central Nervous System hemorrhages were reported. A further case of Central Nervous System hemorrhage has been reported in a child with an ependymoma with GEFITERO alone. An increased risk of cerebral hemorrhage in adult patients with NSCLC receiving GEFITERO has not been established.
Where GEFITERO and Vinorelbine have been used concomitantly, indicate that GEFITERO may exacerbate the neutropenic effect of Vinorelbine.
Gastrointestinal perforation has been reported in patients taking GEFITERO. In most cases this is associated with other known risk factors, including increasing age, concomitant medications such as steroids or NSAIDs, underlying history of GI ulceration, age, smoking or bowel metastases at sites of perforation.
Effects on ability to drive and use machines: During treatment with GEFITERO, asthenia has been reported and those patients who experience this symptom should observe caution when driving or using machines.
Use in Pregnancy and Lactation: There is no data from the use of Gefitinib in pregnant or breast-feeding women. Studies in animals have shown reproductive toxicity. Animal studies also indicate that Gefitinib and certain metabolites pass into rats breast-milk. Women of childbearing potential must be advised to avoid becoming pregnant, and breast-feeding mothers must be recommended to discontinue nursing while receiving GEFITERO therapy.
Pregnancy and Lactation: There is no data from the use of Gefitinib in pregnant or breast-feeding women. Studies in animals have shown reproductive toxicity. Animal studies also indicate that Gefitinib and certain metabolites pass into rats breast-milk. Women of childbearing potential must be advised to avoid becoming pregnant, and breast-feeding mothers must be recommended to discontinue nursing while receiving GEFITERO therapy.
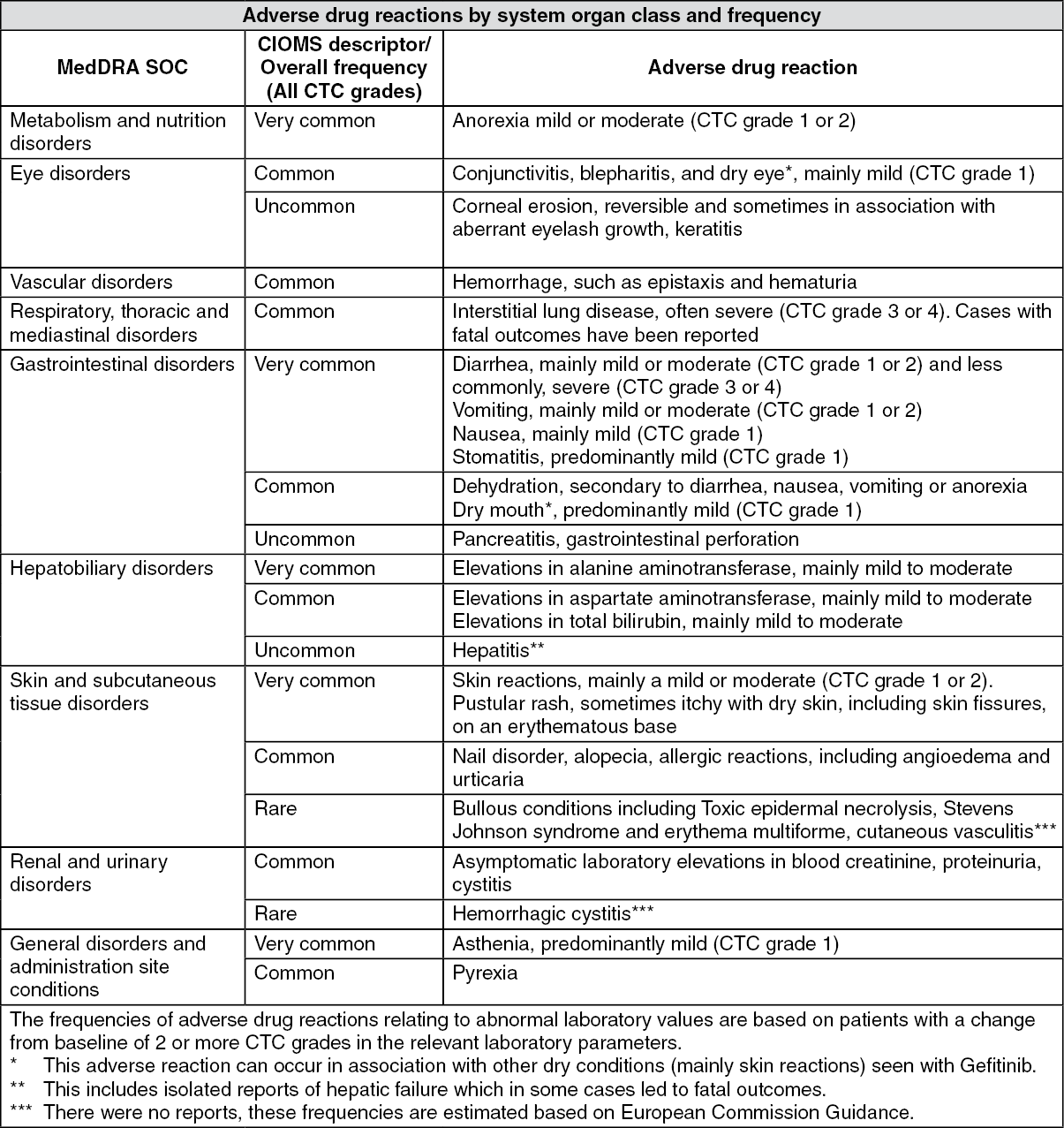
The most commonly reported adverse drug reactions (ADRs), occurring in patients are diarrhea and skin reactions (including rash, acne, dry skin and pruritus). ADRs usually occur within the first month of therapy and are generally reversible. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The metabolism of Gefitinib is predominantly via CYP3A4. Co-administration with Rifampicin (a known potent CYP3A4 inducer) reduced mean Gefitinib AUC (see PRECAUTIONS).
Co-administration with Itraconazole (a CYP3A4 inhibitor) resulted in an increase in the mean AUC of Gefitinib. This increase may be clinically relevant since adverse experiences are related to dose and exposure.
Co-administration of Ranitidine at a dose that caused sustained elevations in gastric pH (≥ 5), resulted in a reduced mean Gefitinib AUC. As consequence, drug that cause significant sustained elevation in gastric pH may reduce plasma concentrations of GEFITERO and therefore may reduce plasma concentrations of GEFITERO and therefore may reduce efficacy (see PRECAUTIONS).
INR elevations and/or bleeding events have been reported in some patients taking Warfarin (see PRECAUTIONS).
Store below 30°C and protect from moisture.
L01EB01 - gefitinib ; Belongs to the class of epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors. Used in the treatment of cancer.
Gefitero FC tab 250 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
