Tablet: The most serious adverse reaction reported in clinical trials with deferiprone is agranulocytosis (neutrophils <0.5 x 10
9/L), with an incidence of 0.8% (0.5 cases per 100 patient-years of treatment), 5.9% (2.5 cases per 100 patient-years). This rate should be considered in the context of the underlying elevated incidence of neutropenia in thalassemia patients, particularly in those with hypersplenism.
Episodes of diarrhea, mostly mild and transient, have been reported in patients treated with deferiprone. Gastrointestinal effects are more frequent at the beginning of therapy and in most patients resolve within a few weeks without discontinuation of treatment. In some patients, it may be beneficial to reduce the dose of deferiprone and then scale it back up to the former dose. Arthropathy events, which ranged from mild pain in 1 or more joints to severe arthritis with effusion and significant disability, have also been reported in patients treated with deferiprone. Mild arthropathies are generally transient.
Increased levels of serum liver enzymes have been reported in patients taking deferiprone. In the majority of these patients, the increase was asymptomatic and transient, and returned to baseline without discontinuation or decreasing the dose of deferiprone (see Precautions: Tablet).
Some patients experienced progression of fibrosis associated with an increase in iron overload or hepatitis C.
In a minority of patients, low plasma zinc levels have been associated with deferiprone. The levels normalized with oral zinc supplementation.
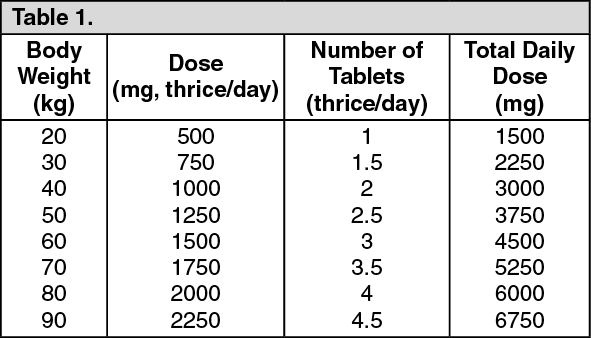
See Table 3.
 Click on icon to see table/diagram/image
Oral Solution: Clinical Trial Experience:
Click on icon to see table/diagram/image
Oral Solution: Clinical Trial Experience: The following adverse reactions are described as follows and as previously mentioned in the labeling: Agranulocytosis/neutropenia; liver enzyme elevations; zinc deficiency (see Precautions: Oral Solution).
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Adverse reaction information for FERRIPROX represents the pooled data collected from 642 patients who participated in single arm or active-controlled clinical trials.
The most serious adverse reaction reported in clinical trials with FERRIPROX was agranulocytosis (see Precautions: Oral Solution).
The most common adverse reactions reported during clinical trials were chromaturia, nausea, vomiting, abdominal pain, alanine aminotransferase increased, arthralgia and neutropenia.
The table as follows lists the adverse drug reactions that occurred in at least 1% of patients treated with FERRIPROX in clinical trials. (See Table 4.)
Click on icon to see table/diagram/image
Gastrointestinal symptoms such as nausea, vomiting, and abdominal pain were the most frequent adverse reactions reported by patients participating in clinical trials and led to the discontinuation of FERRIPROX therapy in 1.6% of patients.
Chromaturia (reddish/brown discoloration of the urine) is a result of the excretion of the iron in the urine.
Postmarketing Experience: The following additional adverse reactions have been reported in patients receiving FERRIPROX. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or to establish a causal relationship to drug exposure.
Blood and lymphatic system disorders: thrombocytosis, pancytopenia.
Cardiac disorders: atrial fibrillation, cardiac failure.
Congenital, familial and genetic disorders: hypospadias.
Eye disorders: diplopia, papilledema, retinal toxicity.
Gastrointestinal disorders: enterocolitis, rectal hemorrhage, gastric ulcer, pancreatitis, parotid gland enlargement.
General disorders and administration site conditions: chills, pyrexia, edema peripheral, multi-organ failure.
Hepatobiliary disorders: jaundice, hepatomegaly.
Immune system disorders: anaphylactic shock, hypersensitivity.
Infections and infestations: cryptococcal cutaneous infection, enteroviral encephalitis, pharyngitis, pneumonia, sepsis, furuncle, infectious hepatitis, rash pustular, subcutaneous abscess.
Investigations: blood bilirubin increased, blood creatinine phosphokinase increased.
Metabolism and nutrition disorders: metabolic acidosis, dehydration.
Musculoskeletal and connective tissue disorders: myositis, chondropathy, trismus.
Nervous system disorders: cerebellar syndrome, cerebral hemorrhage, convulsion, gait disturbance, intracranial pressure increased, psychomotor skills impaired, pyramidal tract syndrome, somnolence.
Psychiatric disorders: bruxism, depression, obsessive-compulsive disorder.
Renal disorders: glycosuria, hemoglobinuria.
Respiratory, thoracic and mediastinal disorders: acute respiratory distress syndrome, epistaxis, hemoptysis, pulmonary embolism.
Skin, subcutaneous tissue disorders: hyperhidrosis, periorbital edema, photosensitivity reaction, pruritis, urticaria, rash, Henoch-Schönlein purpura.
Vascular disorders: hypotension, hypertension.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image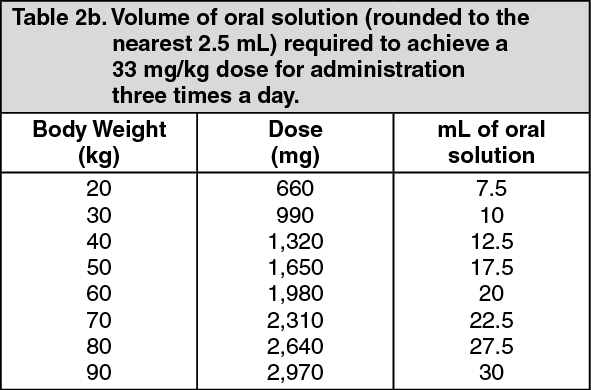 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
