Each vial contains: Esomeprazole Sodium equivalent to Esomeprazole 40 mg.
Pharmacology: Esomeprazole is the S-isomer of Omeprazole which reduces gastric acid secretion through a specific targeted mechanism of action. It is a specific inhibitor of the acid pump in the parietal cell. Both the R- and S- isomer of Omeprazole have familiar pharmacodynamic activity.
Site and mechanism of action: Esomeprazole is a weak base and concentrated, converted to the active form in the highly acidic environment of the secretory canaliculi of the parietal cell, where it inhibits the enzyme H+K+-ATPase the acid pump and inhibits both basal and stimulated acid secretion.
ESOPUMP for injection and infusion are indicated for: Gastric antisecretory treatment when the oral route is not possible, such as: Gastroesophageal reflux disease in patients with esophagitis and/or severe symptoms of reflux.
Healing of gastric ulcers associated with NSAID therapy.
The short-term maintenance of haemostasis and prevention of rebleeding in patients following therapeutic endoscopy for acute bleeding gastric or duodenal ulcers.
Adults: Gastric antisecretory treatment when the oral route is not possible.
Patients who cannot take oral medication may be treated parenterally with 20-40 mg once daily. Patients with reflux oesophagitis should be treated with 40 mg once daily. Patients treated symptomatically for reflux disease should be treated with 20 mg once daily.
For healing of gastric ulcers associated with NSAID therapy the usual dose is 20 mg once daily.
Usually the i.v. treatment duration is short and transfer to oral treatment should be made as soon as possible.
Maintenance of haemostasis and prevention of rebleeding of gastric and duodenal ulcers.
Following therapeutic endoscopy for acute bleeding gastric or duodenal ulcers, 80 mg should be administered as a bolus infusion over 30 minutes, followed by a continuous intravenous infusion of 8 mg/h given over 3 days (72 hours).
The parenteral treatment period should be followed by acid-suppression therapy with Esomeprazole 40 mg tablets once daily for 4 week.
Administrations: For preparation of reconstituted solution see directions for Reconstitution as follows.
Injection: 40 mg dose: 5 mL of the reconstituted solution (8 mg/mL) should be given as an intravenous injection over a period of at least 3 minutes.
20 mg dose: 2.5 mL or half of the reconstituted solution (8 mg/mL) should be given as an intravenous injection over a period of approximately 3 minutes. Any unused solution should be discarded.
Infusion: 40 mg dose: The reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes.
20 mg dose: Half of the reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes. Any unused solution should be discarded.
80 mg bolus dose: The reconstituted solution should be given as a continuous intravenous infusion over 30 minutes.
8 mg/h dose: The reconstituted solution should be given as a continuous intravenous infusion over a period of 71.5 hours (calculated rate of infusion of 8 mg/h).
Children and adolescents: ESOPUMP i.v. should not be used in children and adolescent since no data is available.
Impaired renal function: Dose adjustment is not required in patients with impaired renal function. Due to limited experience in patient with severe renal insufficiency, such patients should be treated with caution.
Impaired hepatic function: GERD: Dose adjustment is not required in patients with mild to moderate liver impairment.
For patients with severe liver impairment, a maximum daily dose of 20 mg ESOPUMP should not be exceeded.
Bleeding ulcers: Dose adjustment is not required in patients with severe liver impairment. For patients with mild to moderate liver impairment. For patients with severe liver impairment, following an initial bolus dose of 80 mg ESOPUMP infusion, a continuous intravenous infusion dose 4 mg/h for 71.5 hours may be sufficient.
Elderly: Dose adjustment is not required in the elderly.
The symptoms described in connection with deliberate Esomeprazole overdose (limited experience of doses in excess of 240 mg/day) are transient. Single oral doses of 80 mg Esomeprazole and intravenous doses of 308 mg Esomeprazole over 24 hours were uneventful. No specific antidote is known. Esomeprazole is extensively bounded plasma protein therefore not readily dialyzable. As in any case of overdose, treatment should be symptomatic and general supportive measures should be utilized.
Known hypersensitivity to Esomeprazole, substituted Benzimidazole or any other constituents of the formulation.
Concomitant administration with Esomeprazole and drugs such as Atazanavir and Nelvinavir is not recommended.
In the presence of any alarm symptom (e.g. significant unintentional weight loss, recurrent vomiting, dysphagia, haematemesis or melaena) and when gastric ulcer is suspected or present, malignancy should be excluded, as treatment with Esomeprazole may alleviate symptoms and delay diagnosis.
Concomitant use of Esomeprazole and Clopidogrel should be avoided.
Some published observational studies suggest that proton pump inhibitor (PPI) therapy may be associated with a small increased risk for osteoporosis related fractures. However, in other similar observational studies no such increased risk was found.
Although a causal relationship between Omeprazole/Esomeprazole and osteoporotic fractures has not been established, patients at risk for developing osteoporosis or osteoporotic fractures are advised to have appropriate clinical monitoring in accordance with current clinical guidelines for these conditions.
Effect on ability to drive and use machines: Esomeprazole is not likely to affect the ability to drive or use machine.
Use in Pregnancy & Lactation: For Esomepazole limited data on exposed pregnancies are available. Caution should be exercised when prescribing Esomeprazole to pregnant women.
It is not known whether Esomeprazole is excreted in human breast milk. No studies in lactating women have been performed.
Therefore Esomeprazole should not be used during breast-feeding.
For Esomepazole limited data on exposed pregnancies are available. Caution should be exercised when prescribing Esomeprazole to pregnant women.
It is not known whether Esomeprazole is excreted in human breast milk. No studies in lactating women have been performed.
Therefore Esomeprazole should not be used during breast-feeding.
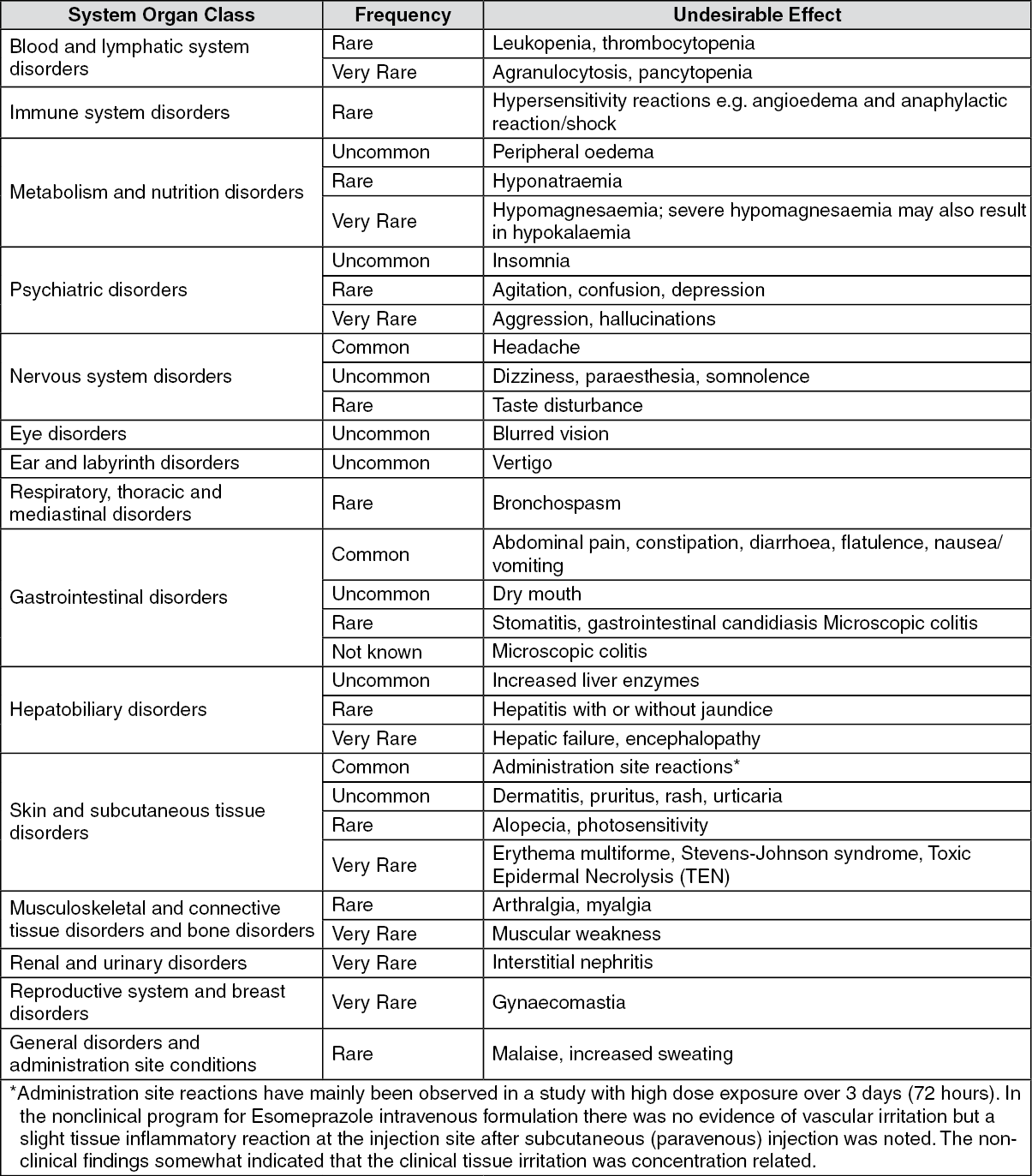
The following definitions of frequencies are used: Common (≥ 1/100), Uncommon (≥ 1/1000, < 1/100), Rare (≥ 1/10,000, < 1/1,000), Very rare (≤1/10,000).
The following adverse drug reactions have been identified or suspected in the clinical trials programme for esomeprazole and/or from post-marketing use. None was found to be dose-related. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Effect of Esomeprazole on pharmacokinetics of the other drugs: The gastric acid suppression during treatment with Esomeprazole i.v. and other PPIs, may decrease or increase the absorption of drugs with a gastric pH dependent absorption. Like with other drugs that decrease the intragastric acidity, the absorption of drugs such as Ketoconazole, Itraconazole and Erlotinib can decrease while the absorption of Digoxin can increase during treatment with Esomeprazole. Concomitant treatment with Omeprazole (20 mg daily) and Digoxin in healthy subjects increased the bioavailability of Digoxin.
Esomeprazole inhibits CYP2C19, the major Esomeprazole enzyme metabolism. Concomitant oral administration of 30 mg Esomeprazole resulted in decreasing clearance of the CYP2C19 substrate Diazepam. This interaction is unlikely to be of clinical relevance. Concomitant oral administration of 40 mg Esomeprazole resulted in increasing trough plasma levels of Phenytoin in epileptic patients. Concomitant oral administration of 40 mg Esomeprazole to Warfarin-treated patients showed that, despite a slight elevation in the trough plasma concentration of the less potent than R-isomer of Warfarin, the coagulation times were within the accepted range.
Pharmacokinetic/pharmacodynamic interaction between Clopidogrel (300 mg loading dose/75 mg daily maintenance dose) and Esomeprazole (40 mg p.o. daily) resulting in decreased exposure to the active metabolite of Clopidogrel and resulting in decreased maximum inhibition of (ADP induced) platelet aggregation.
When given together with proton pump inhibitors, Methotrexate levels have been reported to increase in some patients. In high-dose Methotrexate administration a temporary withdrawal of Esomeprazole may need to be considered.
Omeprazole has been reported to interact with some antiretroviral drugs. Increased gastric pH during Omeprazole treatment may change the absorption of the antiretroviral drug. Other possible interaction mechanisms are via CYP2C19. For some antiretroviral drugs, such as Atazanavir and Nelfinavir, decreased serum levels have been reported when given together with Omeprazole and concomitant administration are not recommended. For other antiretroviral drugs, such as Saquinavir, increased serum levels have been reported. There are also some antiretroviral drugs for which unchanged serum levels have been reported when given with Omeprazole. Due to the similar pharmacodynamic effects and pharmacokinetic properties of Omeprazole and Esomeprazole, concomitant administration with Esomeprazole and antiretroviral drugs such as Atazanavir and Nelfinavir is not recommended (see Contraindications).
Esomeprazole has been shown to have no clinically relevant effects on the pharmacokinetics of Amoxicillin or Quinidine.
Effect of other drugs on pharmacokinetics of Esomeprazole: Esomeprazole is metabolised by CYP2C19 and CYP3A4. Concomitant oral administration of Esomeprazole and a CYP3A4 inhibitor, Clarithromycin (500 mg b.i.d.), resulted in a doubling of the exposure (AUC) to Esomeprazole. Concomitant administration of Esomeprazole and a combined inhibitor of CYP2C19 and CYP3A41, such as Voriconazole, may result in more than doubling of the Esomeprazole exposure. The CYP2C19 and CYP3A4 inhibitor Voriconazole increased Omeprazole AUCT. A dose adjustment of Esomeprazole is not regularly required in either of these situation. However, dose adjustment should be considered in patients with severe hepatic impairment and if long-term treatment is indicated.
Drugs known to induce CYP2C19 or CYP3A4 or both (such as Rifampicin and St. John's wort) may lead to descrease Esomeprazole serum levels by increasing the Esomeprazole metabolism.
Directions for Reconstitution: The reconstituted solution should be inspected visually for particulate matter and discoloration prior to administration. Only clear solution should be used. For single use only. If the entire reconstituted content of the vial is not required, any unused solution should be discarded in accordance with local requirements.
Injection 40 mg: A solution for injection (8 mg/mL) is prepared by adding 5 mL of 0.9% Sodium Chloride for intravenous use to the vial with Esomeprazole. The reconstituted solution for injection is clear and colourless to very slightly yellow.
Half of the volume should be given if 20 mg should be administered. Any unused solution should be discarded.
Infusion 40 mg: A solution for infusion is prepared by dissolving the content of one vial with Esomeprazole 40 mg in up to100 mL 0.9% Sodium Chloride for intravenous use.
Infusion 80 mg: A solution for infusion is prepared by dissolving the content of two vials of Esomeprazole 40 mg in up to 100 mL of 0.9% Sodium Chloride for intravenous use. The reconstituted solution for infusion is clear and colourless to very slightly yellow.
Store below 30°C.
Reconstituted solution must be used within 12 hours at temperature below 30°C.
A02BC05 - esomeprazole ; Belongs to the class of proton pump inhibitors. Used in the treatment of peptic ulcer and gastro-oesophageal reflux disease (GERD).
Esopump powd for inj 40 mg
1's (Rp137,500/boks)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
