Pharmacology: Pharmacodynamics: Mechanism of action: Vannair contains budesonide and formoterol, which have different modes of action and show additive effects in terms of reduction of asthma and COPD exacerbations. The specific properties of budesonide and formoterol allow the combination to be used as maintenance treatment for asthma, and for symptomatic treatment of patients with moderate to severe COPD.
Budesonide is a non-halogenated glucocorticosteroid structurally related to 16α hydroxyprednisolone with a high local anti-inflammatory effect. Budesonide has shown anti-anaphylactic and anti-inflammatory effects in provocation studies in animals and humans, manifested as decreased bronchial obstruction in the immediate as well as the late phase of an allergic reaction. Budesonide has also been shown to decrease airway reactivity to both direct (histamine, methacholine) and indirect (exercise) challenge in hyper-reactive patients. Budesonide, when inhaled, has a rapid (within hours) and dose-dependent anti-inflammatory action in the airways, resulting in reduced symptoms and fewer exacerbations. Inhaled budesonide has less severe adverse effects than systemic corticosteroids. The exact mechanism responsible for the anti-inflammatory effect of glucocorticosteroids is unknown.
Formoterol is a potent selective β
2-adrenergic agonist that produces relaxation of bronchial smooth muscle. Therefore, it has a bronchodilating effect in patients with reversible airways obstruction and in patients with bronchospasm induced by direct (methacholine) and indirect (eg, exercise) stimuli. The bronchodilating effect is dose dependent with an onset of effect within 1 to 3 minutes after inhalation. The duration of effect is at least 12 hours after a single dose.
Clinical trials: Asthma: Therapeutic equivalent between Vannair pMDI and Symbicort Turbuhaler was demonstrated in three clinical efficacy and safety studies in adults and adolescents with asthma. They included two randomised, double-blind, active controlled, parallel-group studies, Studies 681 (12 weeks duration) and 003 (6 weeks duration); and one randomised, open-label, parallel group, long term (12 months) study, Study 715.
No clinical studies have been conducted to directly compare the efficacy and safety of Vannair pMDI 80/2.25 with Symbicort Turbuhaler 160/4.5.
In Study 681, Vannair pMDI 160/4.5 mcg (2 inhalations twice daily) was compared with the corresponding dose of budesonide pMDI (160 μg; 2 inhalations twice daily), or Symbicort Turbuhaler (160/4.5; 2 inhalations twice daily) in adults and adolescents (≥12 years) with moderate to severe asthma (eg mean forced expiratory volume during the first second (FEV
1) ≥50% and ≤90% of predicted normal (PN) and FEV
1 reversibility ≥12%). Vannair pMDI was shown to significantly improve morning peak expiratory flow rate (primary efficacy variable), other lung function parameters, symptom scores and use of rescue medication compared to budesonide and was equivalent to Symbicort Turbuhaler (see Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Study 003 was a 6-week study with similar design to Study 681. In this study, Vannair pMDI 40/2.25 (2 inhalations twice daily) was compared primarily (as regular therapy) with the corresponding dose of budesonide Turbuhaler 80 μg (1 inhalation twice daily), or and secondarily with Symbicort Turbuhaler 80/4.5 (1 inhalation twice daily) in adults and adolescents (≥12 years) with asthma (mean FEV
1 74% PN and FEV
1 reversibility 24%). The primary efficacy variable was the change in morning peak expiratory flow (mPEF) from baseline (mean of the 10 last days of the run-in period) to the treatment period (mean of the 6-week treatment period). The primary objective was to demonstrate that Vannair pMDI 40/2.25 was more efficacious than budesonide Turbuhaler 80 μg. The adjusted mean mPEF increased by 12.2 L/min with Vannair pMDI 40/2.25, 4.15 L/min with budesonide Turbuhaler, and 13.1 L/min with Symbicort Turbuhaler 80/4.5. The results showed that the mean change from baseline in mPEF was greater with Vannair pMDI 40/2.25 than with budesonide Turbuhaler, and that the mean difference was statistically significant (mean difference of 8.07 L/min [95% Cl: 3.26 to 12.9], p=0.001). The secondary objective was to demonstrate therapeutic equivalence of Vannair pMDI 40/2.25 and Symbicort Turbuhaler 80/4.5. The results supported equivalence of the two Vannair pMDI and Symbicort Turbuhaler formulations as regular treatment in both the ITT and per-protocol analyses. There was no statistically significant difference between the Vannair pMDI and Symbicort Turbuhaler formulations for any outcome variable in this study.
Study 715 investigated primarily the safety of Vannair pMDI 160/4.5 (2 inhalations twice daily) during 12 months. The reference treatment was the corresponding dose of Symbicort Turbuhaler 160/4.5 and in a population consisting of adults and adolescents (≥12 years) with moderate to severe asthma (eg mean FEV
1 of ≥50% of PN and FEV
1 reversibility ≥12%). The study was of an open-label design.
There was no statistically significant difference between Vannair pMDI and Symbicort Turbuhaler regarding FEV
1 and FVC (forced vital capacity). The percentage of patients experiencing one or more severe asthma exacerbations did not differ between the Vannair pMDI and Symbicort Turbuhaler groups: 11% in the Vannair pMDI group and 13% in the Symbicort Turbuhaler group. The maximum number of severe exacerbations per patient was 6 in the Vannair pMDI group and 4 in the Symbicort Turbuhaler group. There was no statistical significant difference in time to first severe asthma exacerbation between the two treatment groups.
COPD: The efficacy and safety of Vannair in the treatment of patients with moderate to severe COPD (pre-bronchodilator FEV
1 ≤50% predicted normal) has been evaluated in four randomised, double-blind, placebo and active controlled, parallel-group, multi-centre clinical studies. Two 12-month studies were performed with the dry powder inhaler Symbicort Turbuhaler (studies 629 and 670), and one 12-month and one 6-month study were performed with the pressurised metered dose inhaler (pMDI) Vannair pMDI (studies 001 and 002, respectively).
Studies 629 and 670: In both studies, Symbicort Turbuhaler 160/4.5 was compared with placebo and the corresponding mono-products (budesonide Turbuhaler 160 μg and formoterol Turbuhaler 4.5 μg), all taken as two inhalations twice daily. A total of 812 and 1022 patients with moderate to severe COPD were randomised, of which 208 and 254 were treated with Symbicort Turbuhaler. Patients in both studies had a mean age of 64 years and FEV
1 of 0.99 L or 36% of predicted normal at baseline.
Studies 001 and 002: The study plans were similar. Both studies used Vannair pMDI.
For Study 001, after a screening visit (visit 1), subjects entered a two weeks run-in period after which they were randomly assigned (visit 2) to one of the four following treatments: 1) Vannair pMDI 160/4.5, fixed combination of 160 μg budesonide and 4.5 μg formoterol per actuation, administered as 2 actuations twice daily; 2) Vannair pMDI 80/4.5, fixed combination of 80 μg budesonide and 4.5 μg formoterol per actuation, administered as 2 actuations twice daily; 3) Formoterol Turbuhaler, 4.5 μg per inhalation, administered as 2 actuations twice daily; 4) Placebo.
Study 002 had two additional treatment groups: 5) Budesonide pMDI 160 μg per actuation, administered as 2 actuations twice daily; 6) Free combination of budesonide pMDI 160 μg per actuation plus formoterol Turbuhaler 4.5 μg per actuation, administered as 2 actuations of each twice daily.
A total of 1964 (Study 001) and 1704 (Study 002) patients with moderate to severe COPD were randomised, of which 494 and 277 were treated with Vannair pMDI 160/4.5. The study populations had a mean age of 63 years and mean FEV
1 of 1.04-1.05 L or 34% of predicted normal at baseline.
Study 629: In Study 629, efficacy was evaluated over 12 months using the co-primary endpoints of post-dose FEV
1 and number of severe COPD exacerbations (defined as intake of a course of oral steroids and/or antibiotics and/or hospitalisation due to respiratory symptoms).
Symbicort Turbuhaler significantly improved mean FEV
1 compared with placebo and budesonide by 15% (p<0.001) and 9% (p<0.001), respectively.
Symbicort Turbuhaler significantly reduced the number of severe exacerbations compared with placebo and formoterol by 24% (p=0.035) and 23% (p=0.043), respectively. The number needed to treat (NNT) to prevent one severe COPD exacerbation in a year for Symbicort Turbuhaler compared with formoterol was 2.4.
Study 670: In Study 670, efficacy was evaluated over 12 months using the co-primary endpoints of post dose-FEV
1 and time to first severe COPD exacerbation (defined as intake of a course of oral steroids and/or antibiotics and/or hospitalisation due to respiratory symptoms).
Symbicort Turbuhaler significantly improved mean FEV
1 compared with placebo, budesonide, and formoterol by 14% (p<0.001), 11% (p<0.001), and 5% (p=0.002), respectively.
Symbicort Turbuhaler significantly prolonged the time to first severe COPD exacerbation compared to all comparator treatments. The instantaneous risk of experiencing a severe COPD exacerbation compared to placebo, budesonide, and formoterol was reduced by 29% (p=0.006), 23% (p=0.033), and 30% (p=0.003), respectively.
Symbicort Turbuhaler also significantly reduced the number of severe COPD exacerbations compared to placebo and formoterol by 24% (p=0.029) and 26% (p=0.015), respectively. The NNT to prevent one COPD exacerbation in a year compared to formoterol was 2.1.
Study 001: In Study 001, efficacy was evaluated over 12 months using the co-primary efficacy variables of change from baseline in average pre-dose and 1-hour post-dose FEV
1 over the treatment period.
Primary endpoints: Vannair pMDI 80/4.5 produced a significantly greater change in post-dose FEV
1 compared to placebo (LS mean = 0.16 L; p<0.001); however the change in pre-dose FEV
1 was not significantly different to formoterol 6 μg (LS mean = 0.02 L; p=0.161).
Vannair pMDI 160/4.5 significantly improved 1-hour pre-dose FEV
1 compared with formoterol and placebo by 0.04 L (p=0.008) and 0.09 L (p<0.001) respectively.
Vannair pMDI 160/4.5 significantly improved post-dose FEV
1 over the treatment period compared with formoterol and placebo by 0.03 L (p=0.023) and 0.18 L (p<0.001), respectively.
Serial FEV
1 measures over 12 hours were obtained in a subset of patients (N=491). The median time to onset of bronchodilation (>15% improvement in FEV
1) was seen within 5 minutes at the end of treatment time point in patients receiving Vannair pMDI 160/4.5 (N=121). Maximum improvement in FEV
1 occurred at approximately 2 hours post-dose and post-dose bronchodilator effect was maintained over 12 hours.
Exacerbations (secondary variable): Vannair pMDI reduced the number of severe COPD exacerbations (defined as a worsening of COPD requiring oral steroid use and/or hospitalisation) to a statistically significant degree. Overall 34.1% of subjects experienced 1159 exacerbations: Vannair pMDI 160/4.5, 30.8%; Vannair pMDI 80/4.5, 32.6%; placebo 37.2%. The majority of exacerbations were treated with oral glucocorticosteroids: Vannair pMDI 160/4.5, 96.5% of exacerbations; Vannair pMDI 80/4.5, 94.1%; placebo 97.4%. Treatment comparisons were by means of rate ratios (RR) estimates, CIs and p-values derived from a Poisson regression adjusted for treatment, country and differential treatment exposure. Vannair pMDI 160/4.5 demonstrated a statistically significant reduction of 37% (p<0.001) and 25% (p=0.004) in the rate of exacerbations per subject-treatment year compared with placebo and formoterol respectively. Vannair pMDI 80/4.5 reduced the exacerbation rate by 41% compared with placebo (p<0.001).
Vannair pMDI 160/4.5 significantly prolonged the time to first severe COPD exacerbation compared to placebo, reducing the instantaneous risk of experiencing a severe COPD exacerbation by 26% (p=0.009). The NNT to prevent one severe COPD exacerbation in a year for Vannair pMDI compared with formoterol was 5.4.
Study 002: In Study 002, efficacy was evaluated over 6 months using the co-primary efficacy variables of change from baseline in average pre-dose and 1-hour post-dose FEV
1 over the treatment period.
Vannair pMDI 80/4.5: Post-dose FEV
1 increased significantly from baseline to the average of the treatment period (LS mean [95%CI] = 0.19 [0.17, 0.22]). Vannair pMDI 80/4.5 caused a significantly greater change from baseline compared to budesonide (LS mean = 0.16; p<0.001). Pre-dose FEV
1 increased significantly from baseline to the average of the treatment period, LS mean = 0.06 [0.03, 0.08]. However, the change from baseline, compared to formoterol, for pre-dose FEV
1 was not statistically significant, LS mean = 0.02 [-0.02, 0.05; p=0.335].
Vannair pMDI 160/4.5 significantly improved pre-dose FEV
1 compared with formoterol by 0.04 L (p=0.026) and compared with placebo and budesonide by 0.08 L (p<0.001) for both comparators.
Vannair pMDI 160/4.5 significantly improved 1-hour post-dose FEV
1 compared with formoterol by 0.04 L (p=0.039) and compared with placebo and budesonide by 0.17 L (p<0.001) for both comparators.
Study 002 was not powered for showing effect on severe COPD exacerbations.
Serial FEV
1 measures over 12 hours were obtained in subsets of patients (n=618). The median time to onset of bronchodilation (>15% improvement in FEV
1) was seen within 5 minutes at the end of treatment in patients receiving Vannair pMDI 160/4.5 (N=101). Maximal improvement in FEV
1 occurred at approximately 2 hours post-dose and post-dose bronchodilator effect was generally maintained over 12 hours.
Pharmacokinetics: The budesonide and formoterol bioavailability of Vannair pMDI and Symbicort Turbuhaler were similar after single doses containing 1280 μg budesonide and 36 μg formoterol (8 inhalations) in healthy adult volunteers. The budesonide and formoterol bioavailability from Vannair pMDI was also comparable with that from similar doses of the component products, Pulmicort (budesonide) Turbuhaler, Oxis (formoterol) Turbuhaler and a specially prepared budesonide HFA pressurised inhalation suspension.
There was no evidence of pharmacokinetic interactions between budesonide and formoterol.
Absorption: Inhaled budesonide is rapidly absorbed and the maximum plasma concentration is reached within 30 minutes after inhalation.
Inhaled formoterol is rapidly absorbed and the maximum plasma concentration is reached within 10 minutes after inhalation.
Distribution: Plasma protein binding is approximately 90% for budesonide and volume of distribution is 3 L/kg.
Plasma protein binding is approximately 50% for formoterol and volume of distribution is about 4 L/kg.
Metabolism: Budesonide undergoes an extensive degree (approximately 90%) of biotransformation on first passage through the liver to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6β-hydroxy-budesonide and 16α-hydroxy-prednisolone is less than 1% of that of budesonide.
Formoterol is inactivated via conjugation reactions (active-0-demethylated and deformylated metabolites are formed, but they are seen mainly as inactivated conjugates).
Excretion: Budesonide is eliminated via metabolism mainly catalysed by the enzyme CYP3A4. The metabolites of budesonide are excreted in urine as such or in conjugated form. Only negligible amounts of unchanged budesonide have been detected in the urine. Budesonide has a high systemic clearance (approximately 1.2 L/min) and the plasma elimination half-life after i.v. dosing averages 4 hours.
The major part of a dose of formoterol is eliminated by metabolism in the liver followed by renal excretion. After inhalation of formoterol via a Turbuhaler, 8% to 13% of the delivered dose of formoterol is excreted unmetabolised in the urine. Formoterol has a high systemic clearance (approximately 1.4 L/min) and terminal elimination half-life averages 17 hours.
Special patient populations - children, elderly patients, renal and/or hepatic impairment: The pharmacokinetics of budesonide or formoterol in children, elderly patients, and patients with renal failure is unknown. The systemic availability of budesonide and formoterol may be increased in patients with liver disease.
Toxicology: Preclinical safety data: Genotoxicity: Individually, budesonide and formoterol were not genotoxic in a series of assays for gene mutations (except for a slight increase in reverse mutation frequency in
Salmonella typhimurium at high concentrations of formoterol), chromosomal damage, and DNA repair. The combination of budesonide and formoterol has not been tested in genotoxicity assays.
Carcinogenicity: The carcinogenic potential of the budesonide/formoterol combination has not been investigated in animal studies.
In formoterol carcinogenicity studies performed by AstraZeneca, there was a dose dependent increase in the incidence of uterine leiomyomas in mice dosed orally at 0.1, 0.5, and 2.5 mg/kg/day for 2 years, and a mesovarian leiomyoma was observed in a female rat dosed by inhalation at 0.13 mg/kg/day for 2 years. The effects observed are expected findings with high-dose exposure to β
2-agonists.
Formoterol carcinogenicity studies performed by other companies used systemic exposure levels 800 to 4800-fold higher than those expected upon clinical use of formoterol (based on an 18 μg daily dose).
Some carcinogenicity activity was observed in rats and mice. However, in view of the dose levels at which these effects were observed and the fact that formoterol is not mutagenic (except for very weak activity at high concentrations in one test system), it is concluded that the cancer risk in patients treated with formoterol fumarate is no greater than for other β
2-adrenoceptor agonists.
The carcinogenic potential of budesonide has been evaluated in the mouse and rat at oral doses up to 200 and 50 μg/kg/day respectively. In male rats dosed with 10, 25, and 50 μg budesonide/kg/day, those receiving 25 and 50 μg/kg/day showed an increased incidence of primary hepatocellular tumours. In a repeat study, this effect was observed in a number of steroid groups (budesonide, prednisolone, triamcinolone acetonide), thus indicating a class effect of corticosteroids.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image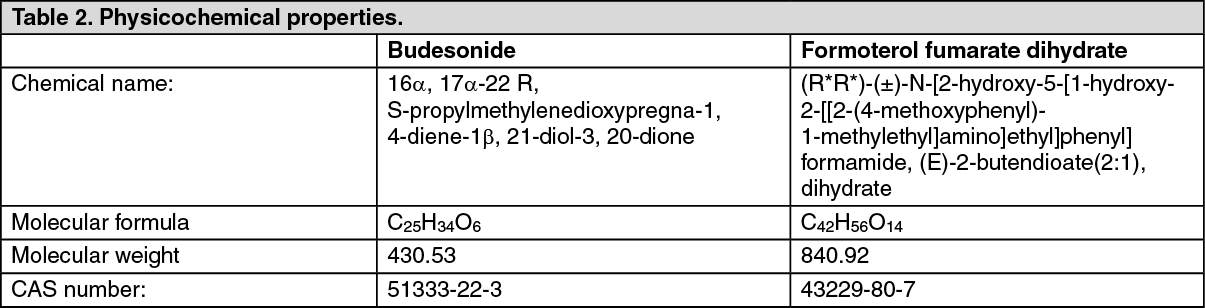 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image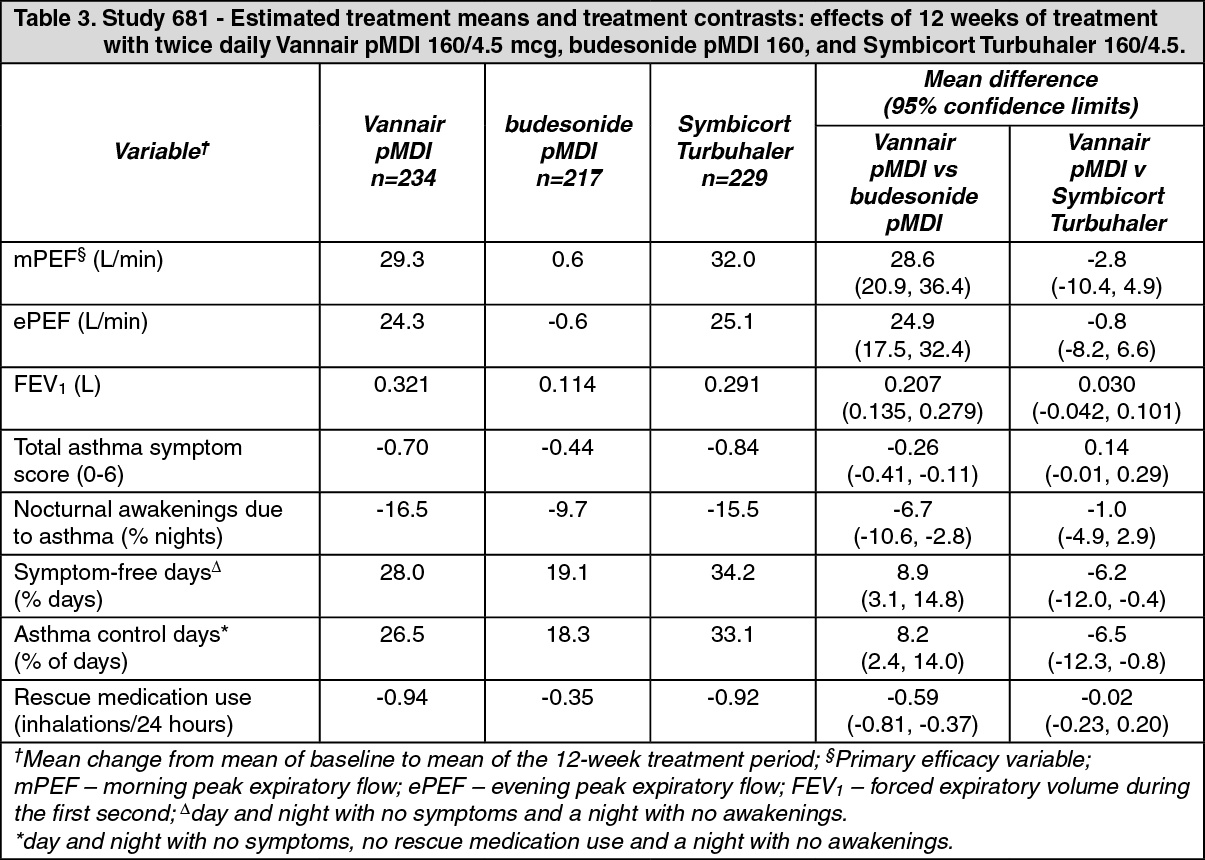 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image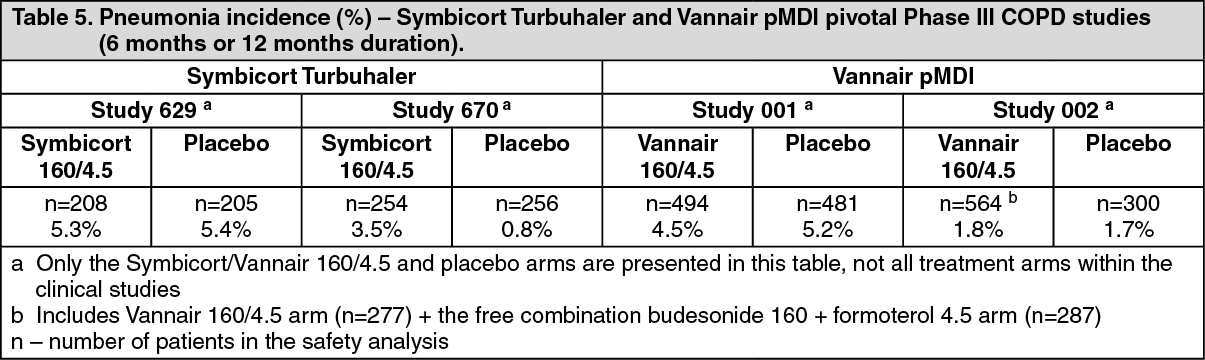 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
