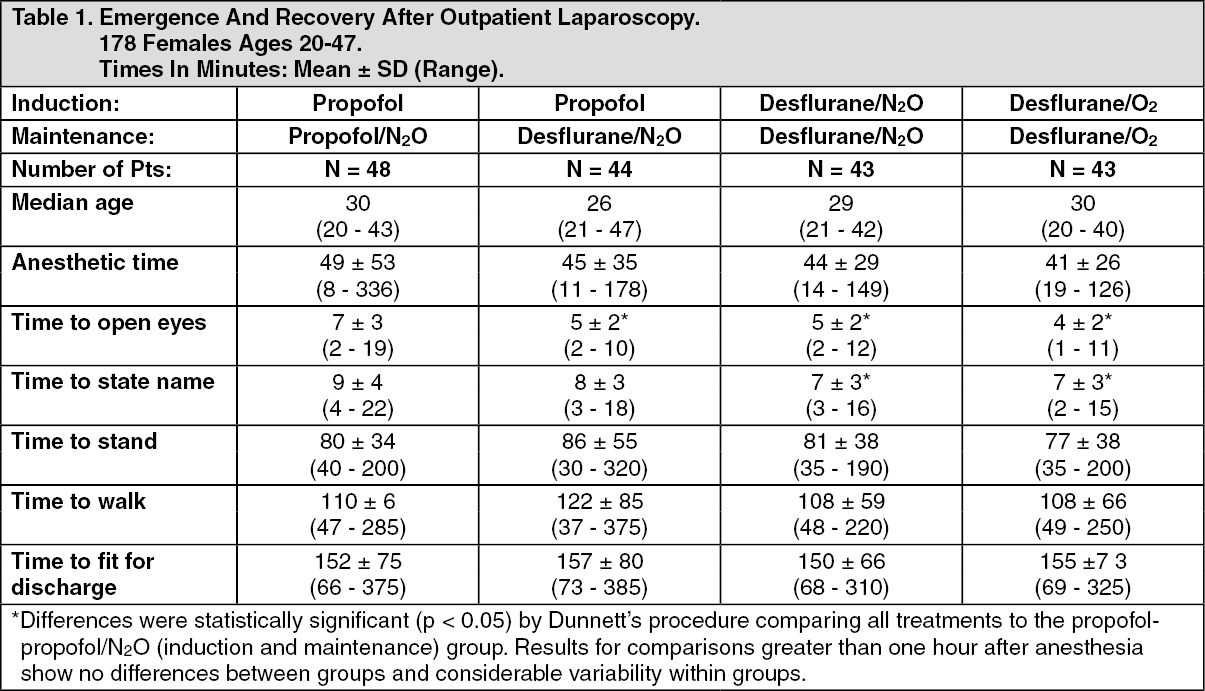
Pharmacology: Pharmacodynamics: Changes in the clinical effects of SUPRANE rapidly follow changes in the inspired concentration. The duration of anesthesia and selected recovery measures for SUPRANE are given in the following tables: In 178 female outpatients undergoing laparoscopy, premedicated with fentanyl (1.5-2.0 μg/kg), anesthesia was initiated with propofol 2.5 mg/kg, desflurane/N
2O 60% in O
2 or desflurane/O
2 alone. Anesthesia was maintained with either propofol 1.5-9.0 mg/kg/hr, desflurane 2.6-8.4% in N
2O 60% in O
2, or desflurane 3.1-8.9% in O
2. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In 88 unpremedicated outpatients, anesthesia was initiated with thiopental 3-9 mg/kg or desflurane in O
2. Anesthesia was maintained with isoflurane 0.7-1.4% in N
2O 60%, desflurane 1.8-7.7% in N
2O 60%, or desflurane 4.4-11.9% in O
2. (See Table 2.)
Click on icon to see table/diagram/image
Recovery from anesthesia was assessed at 30, 60, and 90 minutes following 0.5 MAC desflurane (3%) or isoflurane (0.6%) in N
2O 60% using subjective and objective tests. At 30 minutes after anesthesia, only 43% of patients in the isoflurane group were able to perform the psychometric tests compared to 76% in the SUPRANE group (p < 0.05). (See Table 3.)
Click on icon to see table/diagram/image
SUPRANE was studied in twelve volunteers receiving no other drugs. Hemodynamic effects during controlled ventilation (PaCO
2 38 mm Hg) were: See Table 4.
Click on icon to see table/diagram/image
When the same volunteers breathed spontaneously during desflurane anesthesia, systemic vascular resistance and mean arterial blood pressure decreased; cardiac index, heart rate, stroke volume, and central venous pressure (CVP) increased compared to values when the volunteers were conscious. Cardiac index, stroke volume, and CVP were greater during spontaneous ventilation than during controlled ventilation.
During spontaneous ventilation in the same volunteers, increasing the concentration of SUPRANE from 3% to 12% decreased tidal volume and increased arterial carbon dioxide tension and respiratory rate. The combination of N
2O 60% with a given concentration of desflurane gave results similar to those with desflurane alone. Respiratory depression produced by desflurane is similar to that produced by other potent inhalation agents.
The use of desflurane concentrations higher than 1.5 MAC may produce apnea. (See Figure 1.)
Click on icon to see table/diagram/image
Clinical Studies: The efficacy of SUPRANE was evaluated in 1,843 patients including ambulatory (N=1,061), cardiovascular (N=277), geriatric (N=103), neurosurgical (N=40), and pediatric (N=235) patients. Clinical experience with these patients and with 1,087 control patients in these studies not receiving SUPRANE is described as follows. Although SUPRANE can be used in adults for the inhalation induction of anesthesia via mask, it produces a high incidence of respiratory irritation (coughing, breathholding, apnea, increased secretions, laryngospasm). Oxyhemoglobin saturation below 90% occurred in 6% of patients (from pooled data, N = 370 adults).
Ambulatory Surgery: SUPRANE plus N
2O was compared to isoflurane plus N
2O in multicenter studies (21 sites) of 792 ASA physical status I, II, or III patients aged 18-76 years (median 32).
Induction: Anesthetic induction begun with thiopental and continued with SUPRANE was associated with a 7% incidence of oxyhemoglobin saturation of 90% or less (from pooled data, N = 307) compared with 5% in patients in whom anesthesia was induced with thiopental and isoflurane (from pooled data, N = 152).
Maintenance & Recovery: SUPRANE with or without N
2O or other anesthetics was generally well tolerated. There were no differences between SUPRANE and the other anesthetics studied in the times that patients were judged fit for discharge.
In one outpatient study, patients received a standardized anesthetic consisting of thiopental 4.2-4.4 mg/kg, fentanyl 3.5-4.0 μg/kg, vecuronium 0.05-0.07 mg/kg, and N
2O 60% in oxygen with either desflurane 3% or isoflurane 0.6%. Emergence times were significantly different; but times to sit up and discharge were not different (see Table 5).
Click on icon to see table/diagram/image
Cardiovascular Surgery: SUPRANE was compared to isoflurane, sufentanil or fentanyl for the anesthetic management of coronary artery bypass graft (CABG), abdominal aortic aneurysm, peripheral vascular and carotid endarterectomy surgery in 7 studies at 15 centers involving a total of 558 patients. In all patients except the desflurane vs. sufentanil study, the volatile anesthetics were supplemented with intravenous opioids, usually fentanyl. Blood pressure and heart rate were controlled by changes in concentration of the volatile anesthetics or opioids and cardiovascular drugs if necessary. Oxygen (100%) was the carrier gas in 253 of 277 desflurane cases (24 of 277 received N
2O/O
2). (See Table 6.)
Click on icon to see table/diagram/image
No differences were found in cardiovascular outcome (death, myocardial infarction, ventricular tachycardia or fibrillation, heart failure) among desflurane and the other anesthetics.
Induction: SUPRANE should not be used as the sole agent for anesthetic induction in patients with coronary artery disease or any patients where increases in heart rate or blood pressure are undesirable. In the desflurane vs. sufentanil study, anesthetic induction with desflurane without opioids was associated with new transient ischemia in 14 patients vs. 0 in the sufentanil group. In the desflurane group, mean heart rate, arterial pressure, and pulmonary blood pressure increased and stroke volume decreased in contrast to no change in the sufentanil group. Cardiovascular drugs were used frequently in both groups: especially esmolol in the desflurane group (56% vs. 0%) and phenylephrine in the sufentanil group (43% vs. 27%). When 10 μg/kg of fentanyl was used to supplement induction of anesthesia at one other center, continuous 2-lead ECG analysis showed a low incidence of myocardial ischemia and no difference between desflurane and isoflurane. If desflurane is to be used in patients with coronary artery disease, it should be used in combination with other medications for induction of anesthesia, preferably intravenous opioids and hypnotics.
Maintenance & Recovery: In studies where SUPRANE or isoflurane anesthesia was supplemented with fentanyl, there were no differences in hemodynamic variables or the incidence of myocardial ischemia in the patients anesthetized with desflurane compared to those anesthetized with isoflurane.
During the precardiopulmonary bypass period, in the desflurane vs. sufentanil study where the desflurane patients received no intravenous opioid, more desflurane patients required cardiovascular adjuvants to control hemodynamics than the sufentanil patients. During this period, the incidence of ischemia detected by ECG or echocardiography was not statistically different between desflurane (18 of 99) and sufentanil (9 of 98) groups. However, the duration and severity of ECG-detected myocardial ischemia was significantly less in the desflurane group. The incidence of myocardial ischemia after cardiopulmonary bypass and in the ICU did not differ between groups.
Geriatric Surgery: SUPRANE plus N
2O was compared to isoflurane plus N
2O in a multicenter study (6 sites) of 203 ASA physical status II or III elderly patients, aged 57-91 years (median 71).
Induction: Most patients were premedicated with fentanyl (mean 2 μg/kg), preoxygenated, and received thiopental (mean 4.3 mg/kg IV) or thiamylal (mean 4 mg/kg IV) followed by succinylcholine (mean 1.4 mg/kg IV) for intubation.
Maintenance & Recovery: Heart rate and arterial blood pressure remained within 20% of preinduction baseline values during administration of SUPRANE 0.5-7.7% (average 3.6%) with 50-60% N
2O. Induction, maintenance, and recovery cardiovascular measurements did not differ from those during isoflurane/N
2O administration nor did the postoperative incidence of nausea and vomiting differ. The most common cardiovascular adverse event was hypotension occurring in 8% of the desflurane patients and 6% of the isoflurane patients.
Neurosurgery: SUPRANE was studied in 38 patients aged 26-76 years (median 48 years), ASA physical status II or III undergoing neurosurgical procedures for intracranial lesions.
Induction: Induction consisted of standard neuroanesthetic techniques including hyperventilation and thiopental.
Maintenance: No change in cerebrospinal fluid pressure (CSFP) was observed in 8 patients who had intracranial tumors when the dose of SUPRANE was 0.5 MAC in N
2O 50%. In another study of 9 patients with intracranial tumors, 0.8 MAC desflurane/air/O
2 did not increase CSFP above post induction baseline values. In a different study of 10 patients receiving 1.1 MAC desflurane/air/O
2, CSFP increased 7 mm Hg (range 3-13 mm Hg increase, with final values of 11-26 mm Hg) above the pre-drug values.
All volatile anesthetics may increase intracranial pressure in patients with intracranial space occupying lesions. In such patients, SUPRANE should be administered at 0.8 MAC or less, and in conjunction with a barbiturate induction and hyperventilation (hypocapnia) in the period before cranial decompression. Appropriate attention must be paid to maintain cerebral perfusion pressure. The use of a lower dose of SUPRANE and the administration of a barbiturate and mannitol would be predicted to lessen the effect of desflurane on CSFP.
Under hypocapnic conditions (PaCO
2 27 mm Hg) SUPRANE 1 and 1.5 MAC did not increase cerebral blood flow (CBF) in 9 patients undergoing craniotomies. CBF reactivity to increasing PaCO
2 from 27 to 35 mm Hg was also maintained at 1.25 MAC desflurane/air/O
2.
Pediatric Surgery: In a clinical safety trial conducted in children aged 2 to 16 years (mean 7.4 years), following induction with another agent, SUPRANE and isoflurane (in N
2O/O
2) were compared when delivered via face mask or laryngeal mask airway (LMA mask) for maintenance of anesthesia, after induction with intravenous propofol or inhaled sevoflurane, in order to assess the relative incidence of respiratory adverse events. (See Table 7.)
Click on icon to see table/diagram/image
SUPRANE was associated with higher rates (compared with isoflurane) of coughing, laryngospasm and secretions with an overall rate of respiratory events of 39%. Of the pediatric patients exposed to desflurane, 5% experienced severe laryngospasm (associated with significant desaturation; i.e. SpO
2 of <90% for >15 seconds, or requiring succinylcholine), across all ages, 2-16 years old. Individual age group incidences of severe laryngospasm were 9% for 2-6 years old, 1% for 7-11 years old, and 1% for 12-16 years old. Removal of LMA mask under deep anesthesia (MAC range 0.6 - 2.3 with a mean of 1.12 MAC) was associated with a further increase in frequency of respiratory adverse events as compared to awake LMA mask removal or LMA mask removal under deep anesthesia with the comparator. The frequency and severity of non-respiratory adverse events were comparable between the two groups.
The incidence of respiratory events under these conditions was highest in children aged 2-6 years. Therefore, similar studies in children under the age of 2 years were not initiated.
Pharmacokinetics: Due to the volatile nature of desflurane in plasma samples, the washin-washout profile of desflurane was used as a surrogate of plasma pharmacokinetics. SUPRANE is a volatile liquid inhalation anesthetic minimally biotransformed in the liver in humans. Less than 0.02% of the desflurane absorbed can be recovered as urinary metabolites (compared to 0.2% for isoflurane). Eight healthy male volunteers first breathed 70% N
2O/30% O
2 for 30 minutes and then a mixture of desflurane 2.0%, isoflurane 0.4%, and halothane 0.2% for another 30 minutes. During this time, inspired and end-tidal concentrations (F
I and F
A) were measured. The F
A/F
I (washin) value at 30 minutes for desflurane was 0.91, compared to 1.00 for N
2O, 0.74 for isoflurane, and 0.58 for halothane (see Figure 2). The washin rates for halothane and isoflurane were similar to literature values. The washin was faster for desflurane than for isoflurane and halothane at all time points. The F
A/F
AO (washout) value at 5 minutes was 0.12 for desflurane, 0.22 for isoflurane, and 0.25 for halothane (see Figure 3). The washout for desflurane was more rapid than that for isoflurane and halothane at all elimination time points. By 5 days, the F
A/F
AO for desflurane is 1/20th of that for halothane or isoflurane. (See Figures 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenesis: Long-term studies in animals to evaluate the carcinogenic potential of desflurane have not been conducted.
Mutagenesis:
In vitro and
in vivo genotoxicity studies did not demonstrate mutagenicity or chromosomal damage by desflurane. Tests for genotoxicity included the Ames mutation assay, the metaphase analysis of human lymphocytes, and the mouse micronucleus assay.
Impairment of Fertility: In a study in which male animals were administered 8.2% desflurane (60% oxygen) for either 0.5, 1.0, or 4.0 hours per day beginning 63 days prior to mating and female animals were administered the same doses of desflurane for 14 days prior to mating through Lactation Day 21, there were no adverse effects on fertility in the 1.0 hour per day treatment group. However, reduced male and female fertility was noted in the 4 hour a day group. A dose dependent increase in mortality and decreased body weight gain was note in all treatment groups.
Animal Toxicology and/or Pharmacology: Published studies in animals demonstrate that the use of anesthetic agents during the period of rapid brain growth or synaptogenesis results in widespread neuronal and oligodendrocyte cell loss in the developing brain and alterations in synaptic morphology and neurogenesis. Based on comparisons across species, the window of vulnerability to these changes is believed to correlate with exposures in the third trimester through the first several months of life, but may extend out to approximately 3 years of age in humans.
In primates, exposure to 3 hours of an anesthetic regimen that produced a light surgical plane of anesthesia did not increase neuronal cell loss, however, treatment regimens of 5 hours or longer increased neuronal cell loss. Data in rodents and in primates suggest that the neuronal and oligodendrocyte cell losses are associated with subtle but prolonged cognitive deficits in learning and memory. The clinical significance of these nonclinical findings is not known, and healthcare providers should balance the benefits of appropriate anesthesia in neonates and young children who require procedures against the potential risks suggested by the nonclinical data [see Pediatric Neurotoxicity and Use in Children under Precautions; Pregnancy under Use in Pregnancy & Lactation].




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image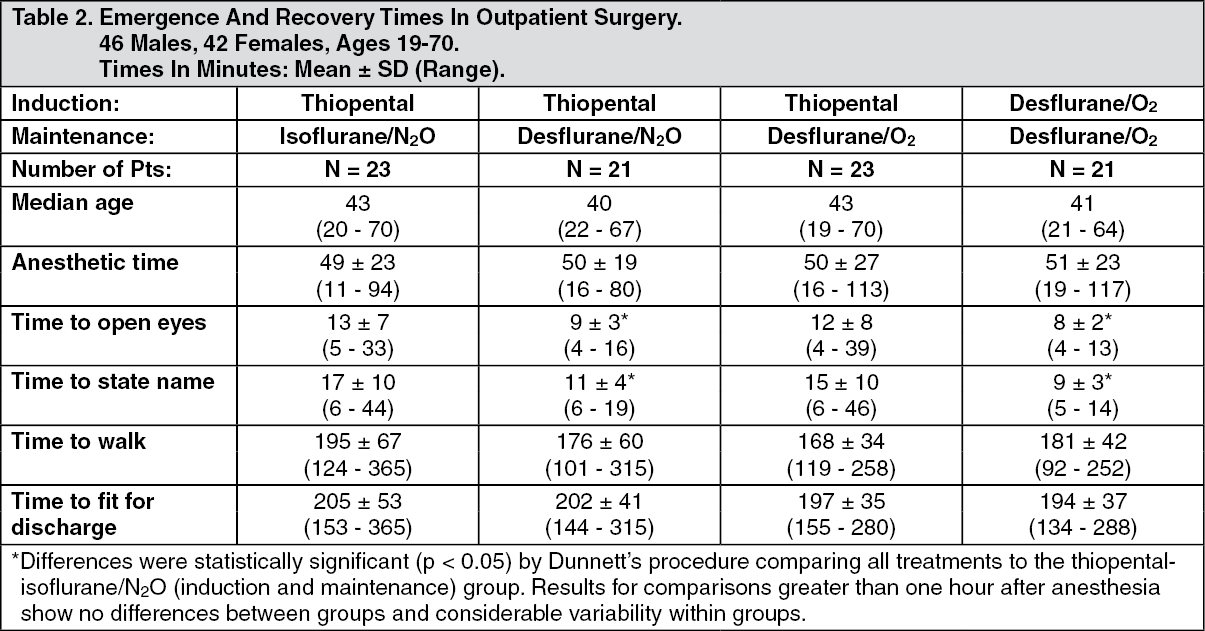 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image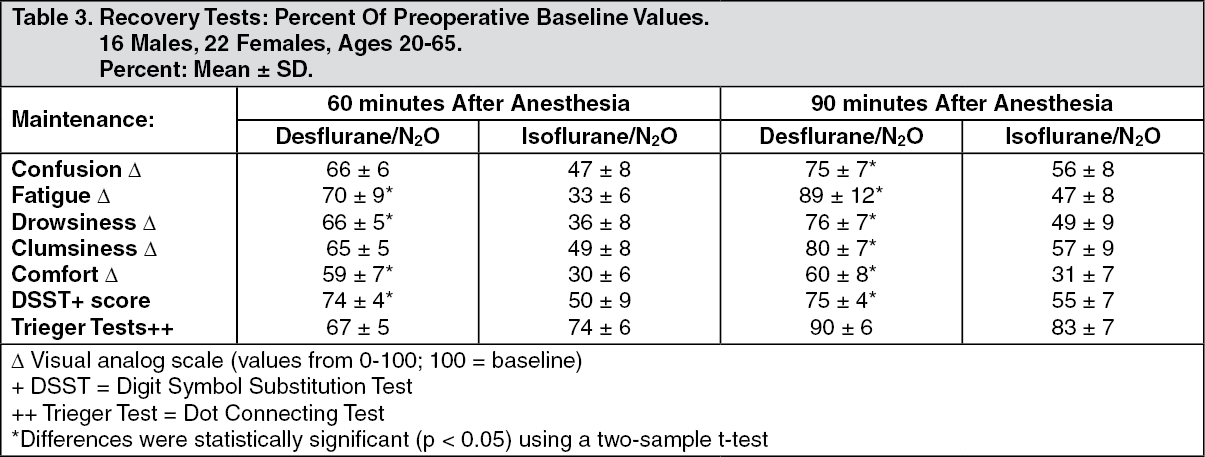 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image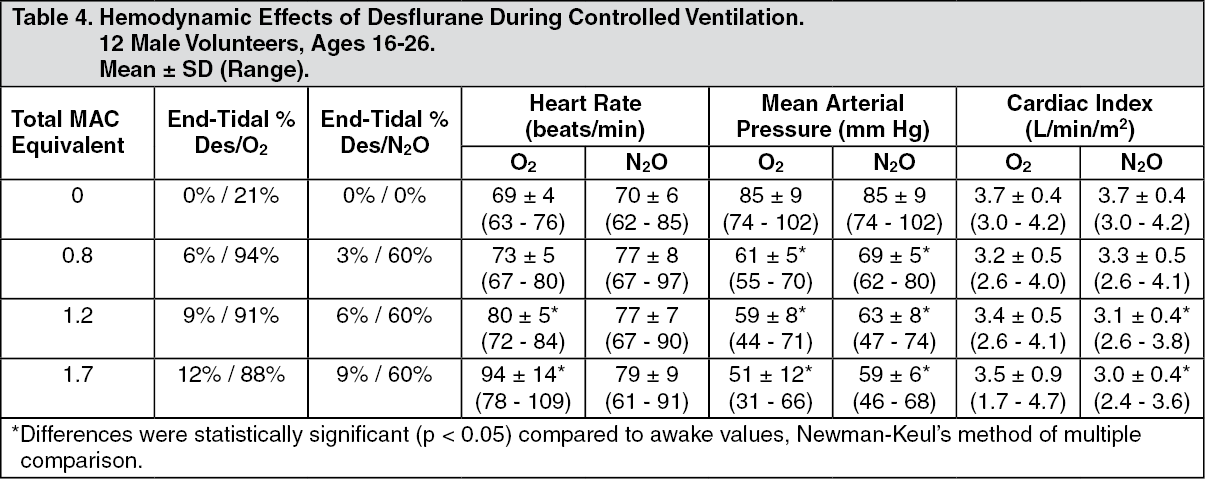 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image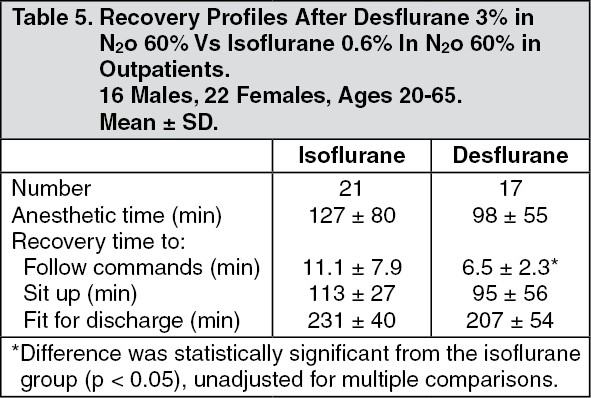 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image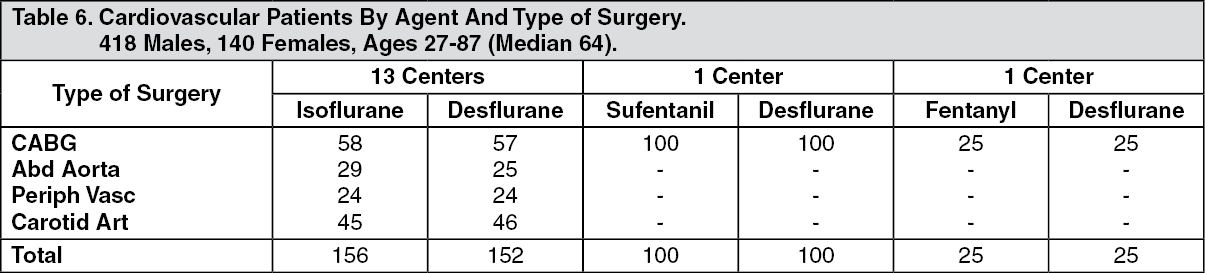 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image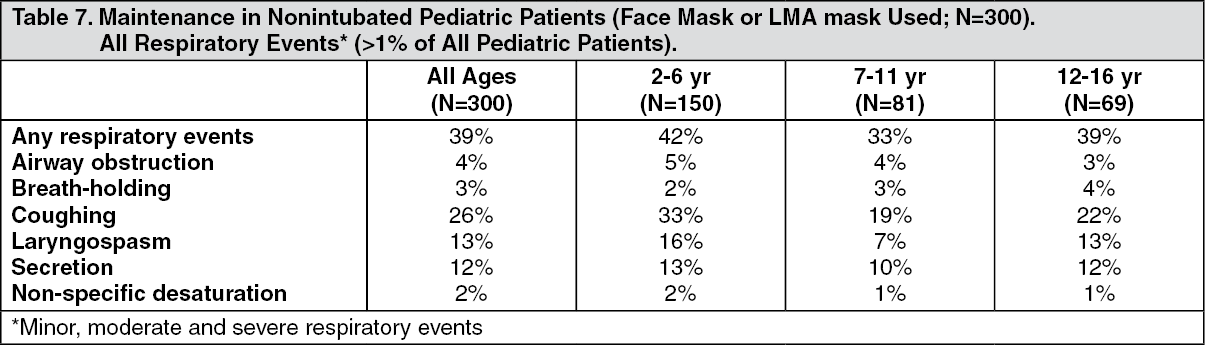 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image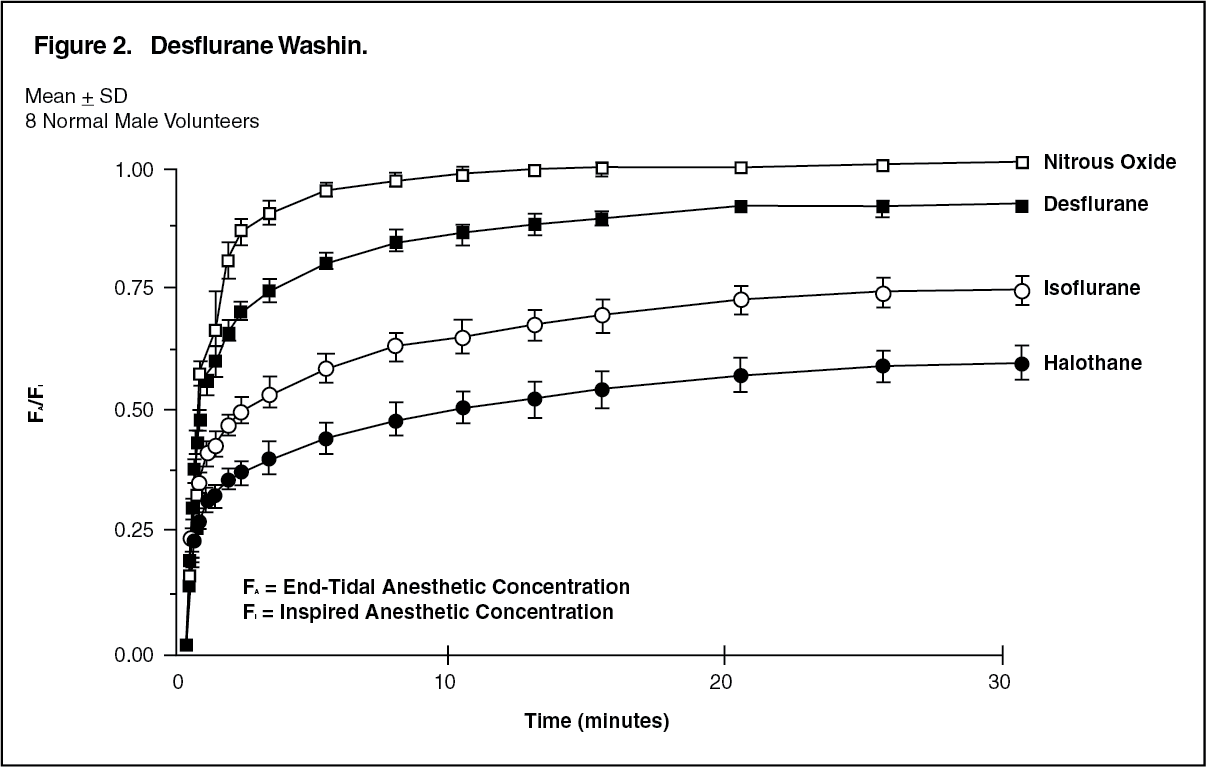 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image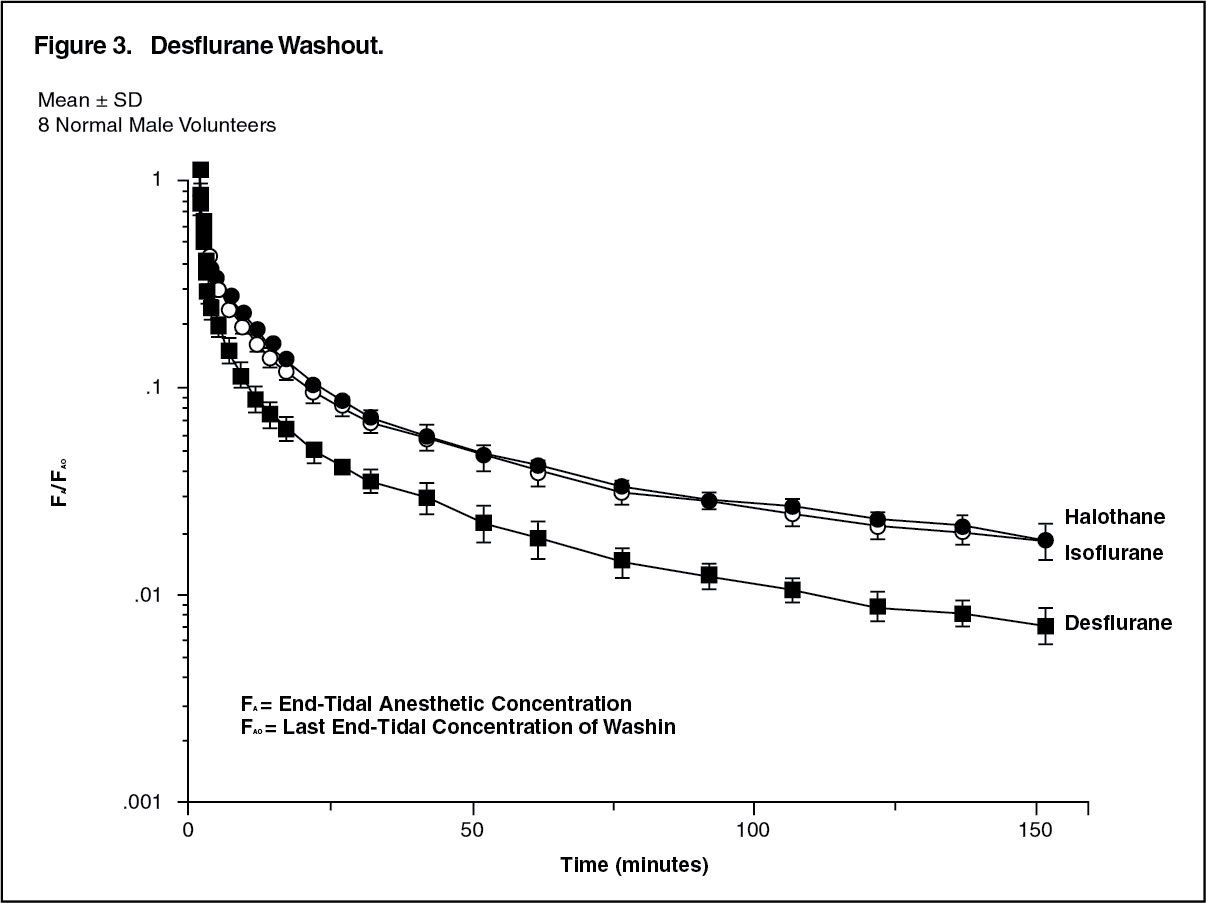 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image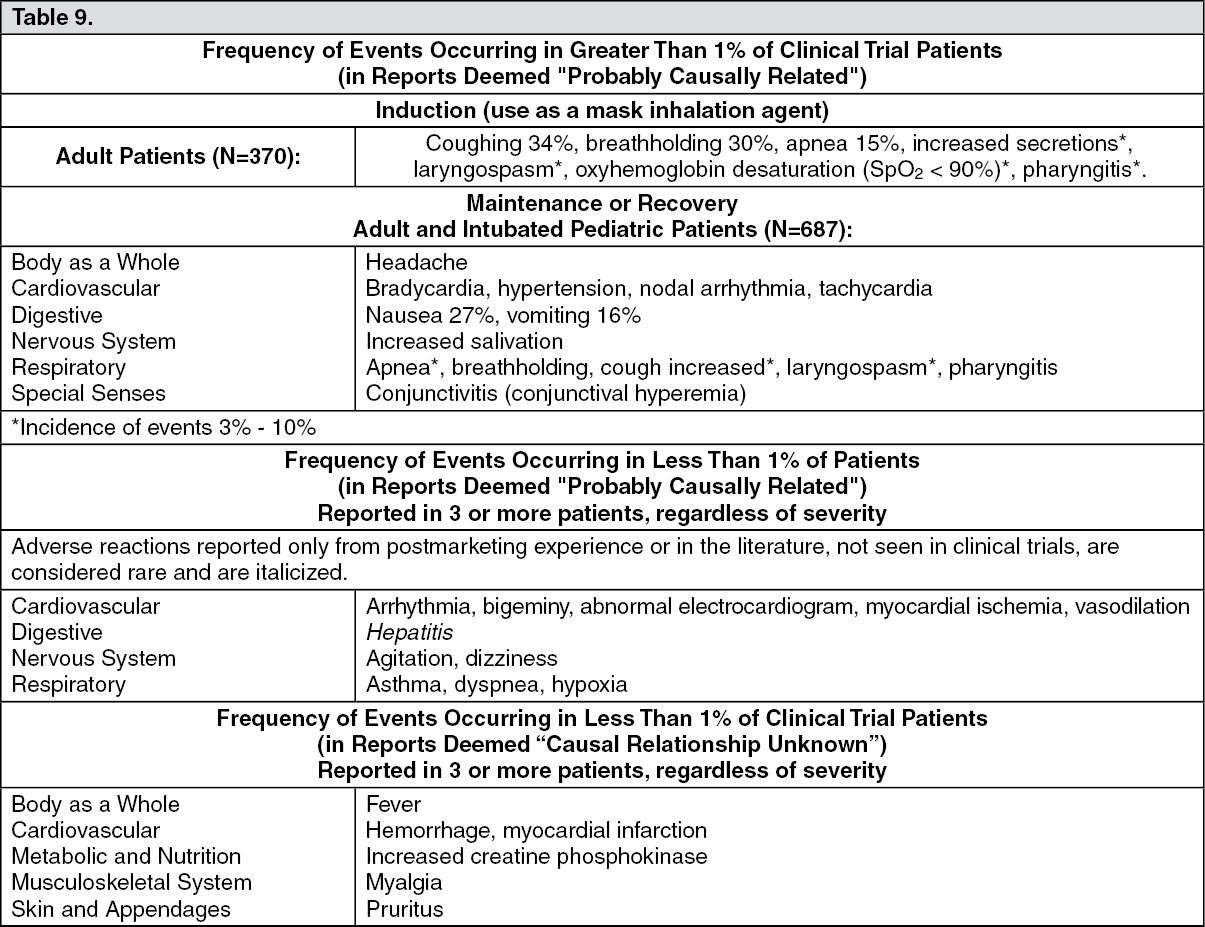 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
