Pharmacotherapeutic group: Immunosuppressants, Selective immunosuppressants.
ATC code: L04AA51.
Pharmacology: Pharmacodynamics: Mechanism of action: Anifrolumab is a human immunoglobulin G1 kappa monoclonal antibody that binds to subunit 1 of the type I interferon receptor (IFNAR1) with high specificity and affinity. This binding inhibits type I IFN signalling thereby blocking the biologic activity of type I IFNs. Anifrolumab also induces the internalisation of IFNAR1, thereby reducing the levels of cell surface IFNAR1 available for receptor assembly. Blockade of receptor mediated type I IFN signalling inhibits IFN responsive gene expression as well as downstream inflammatory and immunological processes. Inhibition of type I IFN blocks plasma cell differentiation and normalises peripheral T-cell subsets, restoring the balance between adaptive and innate immunity that is dysregulated in SLE.
Pharmacodynamic effects: In adult patients with SLE, administration of anifrolumab at doses ≥300 mg, via intravenous infusion every 4 weeks, demonstrated consistent neutralisation (≥80%) of a 21 gene type I interferon pharmacodynamic (PD) signature in blood. This suppression occurred as early as 4 weeks post-treatment and was either maintained or further suppressed over the 52-week treatment period. Following withdrawal of anifrolumab at the end of the 52-week treatment period in the SLE clinical trials, the type I IFN PD signature in blood samples returned to baseline levels within 8 to 12 weeks. Anifrolumab 150 mg IV showed <20% suppression of the gene signature at early timepoints, that reached a maximum of <60% by the end of the treatment period.
In SLE patients with positive anti-dsDNA antibodies at baseline, treatment with anifrolumab 300 mg led to numerical reductions in anti-dsDNA antibodies over time through Week 52.
In patients with low complement levels (C3 and C4), increases in complement levels were observed in patients receiving anifrolumab through Week 52.
Clinical efficacy: The safety and efficacy of anifrolumab were evaluated in two 52-week treatment period, multicentre, randomised, double-blind, placebo-controlled, Phase III studies (Trial 1 [TULIP 1] and Trial 2 [TULIP 2]). Patients were diagnosed with SLE according to the American College of Rheumatology (1997) classification criteria.
All patients were ≥18 years of age and had moderate to severe disease, with a SLE Disease Activity Index 2000 (SLEDAI-2K) score ≥6 points, organ level involvement based on British Isles Lupus Assessment Group (BILAG) assessment, and a Physician's Global Assessment [PGA] score ≥1, despite receiving standard SLE therapy consisting of either one or any combination of oral corticosteroids (OCS), antimalarials and/or immunosuppressants at baseline. With the exception of OCS (prednisone or equivalent) where tapering was a component of the protocol, patients continued to receive their existing SLE therapy at stable doses during the clinical trials. Patients who had severe active lupus nephritis and patients who had severe active central nervous system lupus were excluded. The use of other biologic agents and cyclophosphamide were not permitted during the clinical trials. Patients receiving other biologic therapies were required to complete a wash-out period of at least 5 half-lives prior to enrolment. Both studies were conducted in North America, Europe, South America and Asia. Patients received anifrolumab or placebo, administered by intravenous infusion, every 4 weeks.
Trial 1 (N=457) and Trial 2 (N=362) were similar in design.
In Trial 1 the primary endpoint was SLE Responder Index (SRI-4) response, defined as meeting each of the following criteria at Week 52 compared with baseline: Reduction from baseline of ≥4 points in the SLEDAI-2K; No new organ system affected as defined by 1 or more BILAG A or 2 or more BILAG B items compared to baseline; No worsening from baseline in the lupus disease activity defined by an increase ≥0.30 points on a 3-point PGA visual analogue scale (VAS); No use of restricted medication beyond the protocol-allowed thresholds; No discontinuation of treatment.
In Trial 2 the primary endpoint was British Isles Lupus Assessment Group based Composite Lupus Assessment (BICLA) response at Week 52, defined as improvement in all organ domains with moderate or severe activity at baseline: Reduction of all baseline BILAG A to B/C/D and baseline BILAG B to C/D, and no BILAG worsening in other organ systems, as defined by ≥1 new BILAG A or ≥2 new BILAG B; No worsening from baseline in SLEDAI-2K, where worsening is defined as an increase from baseline of >0 points; No worsening from baseline in lupus disease activity, where worsening is defined by an increase ≥0.30 points on a 3-point PGA VAS; No use of restricted medication beyond the protocol-allowed thresholds; No discontinuation of treatment.
The secondary efficacy endpoints included in both studies included maintenance of OCS reduction and annual flare rate. Both studies evaluated the efficacy of anifrolumab 300 mg versus placebo.
Patient demographics were generally similar in both trials; the median age was 41.3 and 42.1 years (range 18-69), 4.4% and 1.7% were ≥65 years of age, 92% and 93% were female, 71% and 60% were White, 14% and 12% were Black/African American, and 5% and 17% were Asian, in Trials 1 and 2 respectively. In both trials, 72% of patients had high disease activity (SLEDAI-2K score ≥10). In Trials 1 and 2 respectively, 47% and 49% had severe disease (BILAG A) in at least 1 organ system and 46% and 47% of patients had moderate disease (BILAG B) in at least 2 organ systems. The most commonly affected organ systems (BILAG A or B at baseline) were the mucocutaneous (Trial 1: 87%, Trial 2: 85%) and musculoskeletal (Trial 1: 89%, Trial 2: 88%) systems.
In Trials 1 and 2, 90% of patients (both trials) were seropositive for anti-nuclear antibodies (ANA), and 45% and 44% for anti-double-stranded DNA (anti-dsDNA) antibodies; 34% and 40% of patients had low C3, and 21% and 26% had low C4.
Baseline concomitant standard therapy medications included oral corticosteroids (Trial 1: 83%, Trial 2: 81%), antimalarials (Trial 1: 73%, Trial 2: 70%) and immunosuppressants (Trial 1: 47%, Trial 2: 48%; including azathioprine, methotrexate, mycophenolate and mizoribine). For those patients taking OCS (prednisone or equivalent) at baseline, the mean daily dose was 12.3 mg in Trial 1 and 10.7 mg in Trial 2. During Weeks 8-40, patients with a baseline OCS ≥10 mg/day were required to taper their OCS dose to ≤7.5 mg/day, unless there was worsening of disease activity.
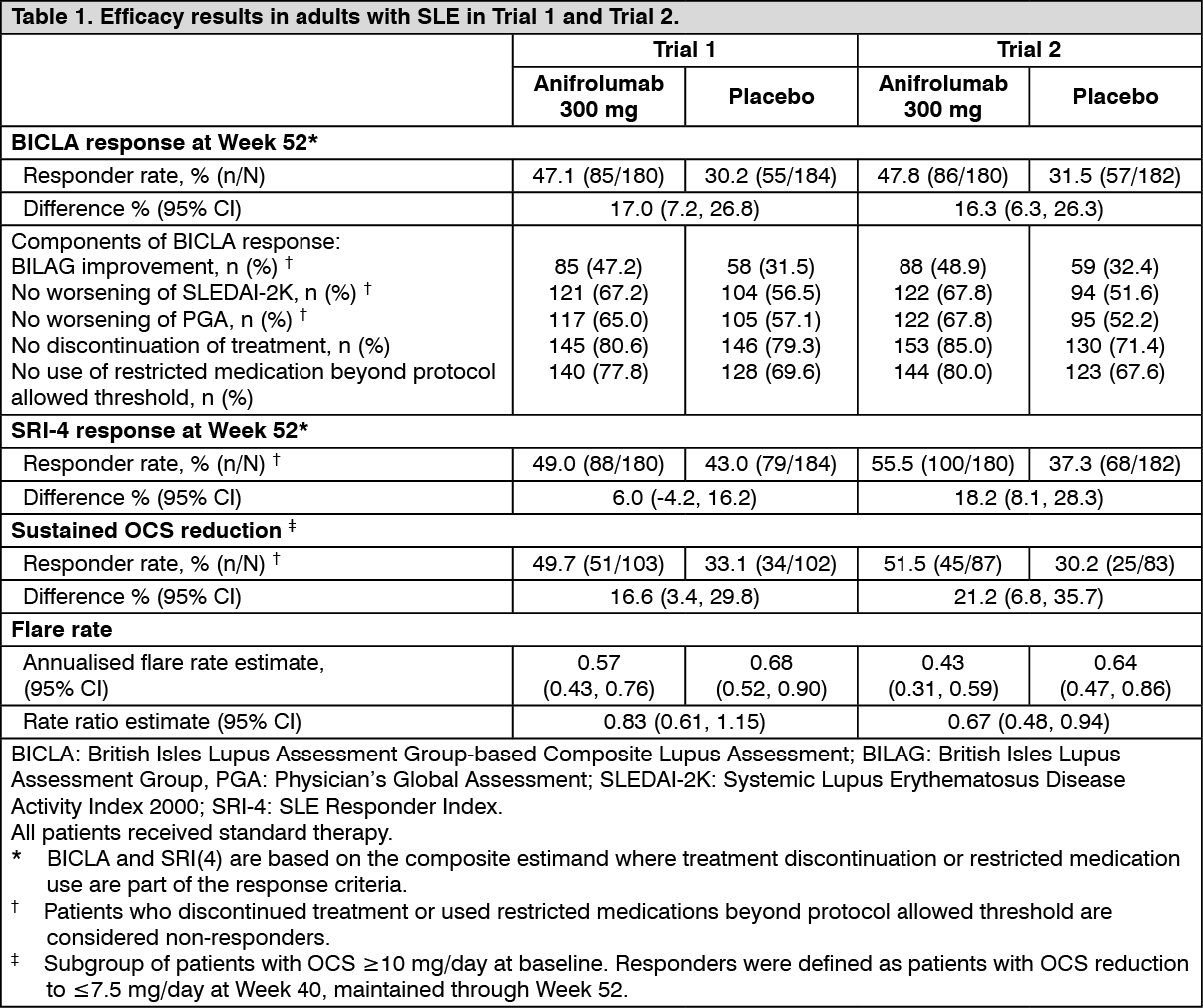
For BICLA and SRI(4) response, patients who withdrew from treatment prior to Week 52 were considered non-responders. In Trial 1 and 2 respectively, 35 (19%) and 27 (15%) patients receiving anifrolumab, and 38 (21%) and 52 (29%) patients receiving placebo withdrew from treatment prior to Week 52. The results are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Pharmacokinetics: The pharmacokinetics (PK) of anifrolumab was studied in adult patients with SLE following intravenous doses ranging from 100 to 1 000 mg, once every 4 weeks, and healthy volunteers following a single dose.
Anifrolumab exhibits nonlinear PK in the dose range of 100 mg to 1 000 mg. PK exposure decreased more rapidly at doses lower than 300 mg every 4 weeks (the recommended dose).
Absorption: Anifrolumab is administered by intravenous infusion.
Distribution: Based on population pharmacokinetic analysis, the estimated central and peripheral volumes of distribution for anifrolumab were 2.93 L (with 26.9% CV inter-individual variability) and 3.3 L, respectively for a 69.1 kg patient.
Biotransformation: Anifrolumab is a protein, therefore specific metabolism studies have not been conducted.
Anifrolumab is eliminated by target IFNAR-mediated elimination pathway and reticuloendothelial system where anifrolumab is expected to be degraded, into small peptides and individual amino acids, by proteolytic enzymes that are widely distributed in the body.
Elimination: Due to saturation of IFNAR1-mediated clearance at higher doses, exposure increases are greater-than-dose-proportional.
From population PK modelling the estimated typical systemic clearance (CL) was 0.193 L/day with a 33.0% CV inter-individual variability. The median CL decreases slowly over time, with an 8.4% reduction after 1 year of treatment.
Based on population PK analysis, serum concentrations were below detection in the majority (95%) of patients approximately 16 weeks after the last dose of anifrolumab, when anifrolumab has been dosed for one year.
Special populations: There was no clinically meaningful difference in systemic clearance based on age, race, ethnicity, region, gender, IFN status or body weight that requires dose adjustment.
Elderly patients (≥ 65 years old): Based on the population PK analysis, age (range 18 to 69 years) did not impact the clearance of anifrolumab; the population PK dataset included 20 (3%) patients ≥65 years of age.
Renal impairment: No specific clinical studies have been conducted to investigate the effect of renal impairment on anifrolumab. Based on population PK analyses, anifrolumab clearance was comparable in SLE patients with mild (60-89 mL/min/1.73 m
2) and moderate decrease in eGFR (30-59 mL/min/1.73 m
2) values and patients with normal renal function (≥90 mL/min/1.73 m
2). SLE patients with a severe decrease in eGFR or end stage renal disease (<30 mL/min/1.73 m
2) were excluded from the clinical trials; anifrolumab is not cleared renally.
Patients with UPCR >2 mg/mg were excluded from the clinical trials. Based on population PK analyses, increased urine protein/creatinine ratio (UPCR) did not significantly affect anifrolumab clearance.
Hepatic impairment: No specific clinical studies have been conducted to investigate the effect of hepatic impairment on anifrolumab.
As an IgG1 monoclonal antibody, anifrolumab is principally eliminated via catabolism and is not expected to undergo metabolism via hepatic enzymes, as such changes in hepatic function are unlikely to have any effect on the elimination of anifrolumab. Based on population pharmacokinetic analyses, baseline hepatic function biomarkers (ALT and AST ≤2.0 × ULN, and total bilirubin) had no clinically relevant effect on anifrolumab clearance.
Interactions: Based on population PK analyses, concomitant use of oral corticosteroids, antimalarials, immunosuppressants (including azathioprine, methotrexate, mycophenolate and mizoribine), NSAIDS, ACE inhibitors, HMG-CoA reductase inhibitors did not significantly influence the PK of anifrolumab.
Toxicology: Preclinical safety data: Non-clinical: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology or repeated dose toxicity studies in cynomolgus monkeys.
Mutagenicity and carcinogenicity: Anifrolumab is a monoclonal antibody, as such genotoxicity and carcinogenicity studies have not been conducted.
In rodent models of IFNAR1 blockade, increased carcinogenic potential has been observed. The clinical relevance of these findings is unknown.
Reproductive toxicity: Developmental toxicity: In a pre- and postnatal development study, conducted in cynomolgus monkeys, there was an increased incidence of embryo-foetal loss; the incidence of these findings were within historical control values and were not statistically significant. The relevance of these findings to humans is not known. No maternal, or postnatal developmental effects were observed for exposures up to approximately 28-times the maximum recommended human dose (MRHD) on an AUC basis. Based on the available data, a potential effect of anifrolumab on conception and implantation cannot be excluded.
Fertility: Effects on male and female fertility have not been directly evaluated in animal studies. In the 9-month repeat dose study, there were no anifrolumab-related adverse effects on indirect measures of male or female fertility, based on semen analysis, spermatogenesis staging, menses cycle, organ weights and histopathological findings in the reproductive organs, in cynomolgus monkeys at approximately 58-times the MRHD on an AUC basis.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
