Pharmacotherapeutic group: Other dermatological preparations, Other dermatologicals.
ATC code: D11AX21.
Pharmacology: Pharmacodynamics: Mechanism of action: Brimonidine is a highly selective alpha
2-adrenergic receptor agonist that is 1000-fold more selective for the alpha
2-adrenergic receptor than the alpha
1-adrenergic receptor.
Pharmacodynamic effects: Cutaneous facial application of a highly selective alpha
2-adrenergic receptor agonist reduces erythema through direct cutaneous vasoconstriction.
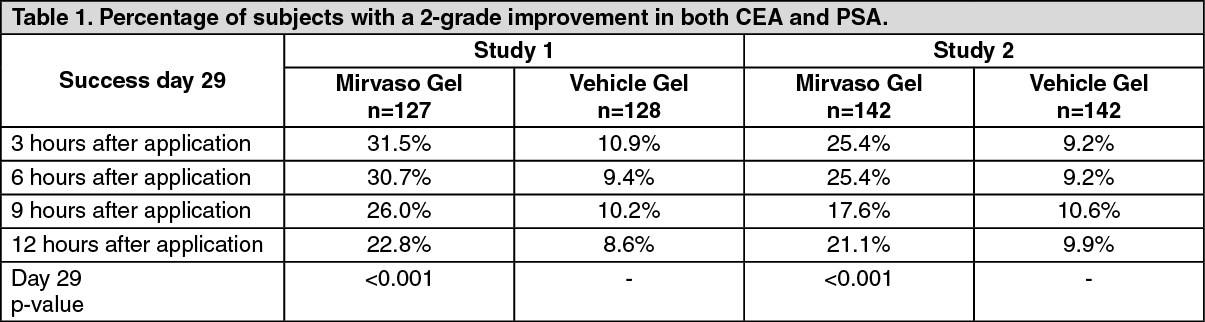
Clinical efficacy and safety: The efficacy of Mirvaso in the treatment of moderate to severe facial erythema of rosacea has been demonstrated in two randomised, vehicle controlled blinded clinical trials, which were identical in design. Moderate to severe erythema was defined as a grade 3 or greater on both the Clinician Erythema Assessment (CEA) scale and Patient Self-Assessment (PSA) scale. The studies were conducted in 553 randomised subjects aged 18 years and older who were treated once daily for 4 weeks with either Mirvaso or vehicle. Of these, 539 completed 29 days of treatment and had data available to be included in the efficacy analysis at Day 29, with the majority being Caucasians between 18 and 65 years of age.
The primary endpoint was expressed in terms of composite success i.e. subjects responding with a 2-grade reduction on both baseline CEA score and baseline PSA score on Day 29. The results from both clinical studies demonstrated that Mirvaso was significantly more effective (p<0.001) in the reduction of facial erythema of rosacea than vehicle gel when applied once daily for 29 days (primary endpoint, see Table 1). For the population subset of patients with severe erythema at baseline Day 1 (i.e. subjects with CEA or PSA grade of 4) which represented 26% of the randomised subjects, the results on the primary endpoint on Day 29 were similar to those results observed in the overall population (see Table 2) and were statistically significant for both studies combined (p=0.003). In addition, for the overall population, Mirvaso demonstrated statistical superiority (p<0.001) over vehicle gel with respect to rapid initial onset of a clinically meaningful effect (1-Grade Composite Success for CEA and PSA) after the first application at 30 minutes on Day 1 (secondary endpoint 27.9% vs. 6.9% for Study 1, 28.4% vs. 4.8% for Study 2), and to achievement of a clinically meaningful effect (1-Grade Composite Success for CEA and PSA) on Day 29 (tertiary endpoint, see Table 3).
CEA and PSA were defined as follows: CEA: Clinician Erythema Assessment: 0=Clear skin with no signs of erythema, 1=Almost clear; slight redness, 2=Mild erythema; definite redness, 3=Moderate erythema + marked redness and 4=Severe erythema + fiery redness.
PSA: Patient Self-Assessment: 0=No redness, 1=Very mild redness, 2=Mild redness, 3=Moderate redness and 4=Severe redness. (See Tables 1, 2 and 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
No clinically meaningful trends with respect to tachyphylaxis or rebound effects (worsening of baseline erythema after cessation of treatment) were observed with use of Mirvaso for 29 days.
The results from a long term open label study in 449 patients, with continuous treatment for up to one year, confirmed that chronic use of Mirvaso is safe and effective. Daily reductions in erythema for the first month of use (as measured with the CEA and PSA scales) were similar to those observed in the controlled trials, and those reductions were achievable for up to 12 months with no apparent loss of effect over time. The overall frequencies of adverse reactions in this study are reflected in Table 4 (see Adverse Reactions), with the highest rates occurring in the first 29 days of use. No adverse reactions had an increase in frequency over time, and there was no evidence that long-term use of Mirvaso conveyed an increased risk of occurrence of any specific type of adverse reaction.
Concomitant use of Mirvaso with other medicinal products for the treatment of inflammatory lesions of rosacea has not been systematically investigated. However, in the long term open label study, the efficacy and safety of Mirvaso, as described previously, was not affected by the concomitant use of cosmetics or other medicinal products (e.g. topical metronidazole, topical azelaic acid, and oral tetracyclines including low dose doxycycline) for the treatment of inflammatory lesions of rosacea in the concerned subpopulation (131/449 patients in the study used concomitant rosacea medicinal product).
Pharmacokinetics: Absorption: The absorption of brimonidine from Mirvaso was evaluated in a clinical study in 24 adult subjects with facial erythema of rosacea. All enrolled subjects received a single-day ocular administration of a 0.2% eye drops solution of brimonidine followed by a once daily cutaneous application of Mirvaso for 29 days (intra-individual comparison of systemic exposure). On Day 1 of the study, all subjects received 1 drop of the 0.2% eye drops solution in each eye, every 8 hours over a 24-hour period (3 doses in total).
After repeated cutaneous application of Mirvaso on facial skin, no drug accumulation in plasma was observed throughout the treatment duration: the highest mean (± standard deviation) plasma maximum concentration (C
max) and area under the concentration-time curve from 0 to 24 hours (AUC
0-24hr) were 46 ± 62 pg/mL and 417 ± 264 pg·hr/mL respectively. These levels are significantly lower (2-fold) than those observed following single-day ocular administration of a 0.2% eye drops solution of brimonidine.
Distribution: The protein binding of brimonidine has not been studied.
Biotransformation: Brimonidine is extensively metabolised by the liver.
Elimination: Urinary excretion is the major route of elimination of brimonidine and its metabolites.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
