


 Sign Out
Sign Out

Following uptake into cancer cells, trifluridine is incorporated into DNA, interferes with DNA synthesis and inhibits cell proliferation. Trifluridine/tipiracil demonstrated anti-tumor activity against KRAS wild-type and mutant human colorectal cancer xenografts in mice.
Pharmacodynamics: Cardiac Electrophysiology: Lonsurf administered to 42 patients with advanced solid tumors at the recommended dosage had no large effect (i.e. >20 ms) in the mean QTc interval when compared to placebo and no exposure-QT relationship was identified. Two of 42 patients (4.8%) had QTc ˃500 msec and 2.4% had a QTc increase from baseline ˃60 msec.
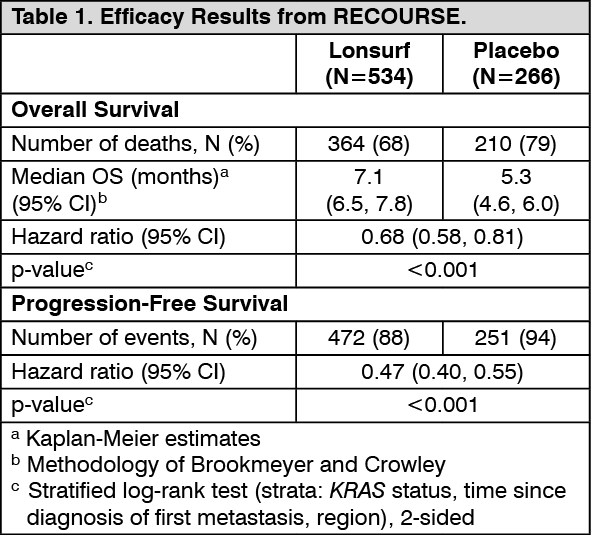
Clinical Studies: Metastatic Colorectal Cancer: The efficacy of Lonsurf was evaluated in the RECOURSE study (NCT01607957), an international, randomized, double-blind, placebo-controlled study conducted in patients with previously treated metastatic colorectal cancer (mCRC). Key eligibility criteria included prior treatment with at least 2 lines of standard chemotherapy for metastatic CRC, ECOG performance status (PS) 0-1, absence of brain metastasis, and absence of ascites requiring drainage in the past four weeks. Patients were randomized 2:1 to receive Lonsurf 35 mg/m2 or matching placebo orally twice daily after meals on Days 1-5 and 8-12 of each 28-day cycle until disease progression or unacceptable toxicity. Randomization was stratified by KRAS status (wild-type vs. mutant), time since diagnosis of first metastasis (<18 months vs. ≥18 months), and region (Japan vs. US, Europe and Australia). The major efficacy outcome measure was overall survival (OS) and an additional efficacy outcome measure was progression-free survival (PFS).
A total of 800 patients were randomized to Lonsurf (N=534) with best supportive care (BSC) or matching placebo (N=266) plus BSC. The median age was 63 years, 61% were male, 58% and 35% were White and Asian respectively, and all patients had baseline ECOG PS of 0 or 1. The primary site of disease was colon (62%) or rectum (38%). KRAS status was wild-type (49%) or mutant (51%) at study entry. All patients received prior treatment with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy. All but one patient received bevacizumab, and all but two patients with KRAS wild-type tumors received panitumumab or cetuximab.
Efficacy results are summarized in Table 1 and Figure 1. (See Table 1 and Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image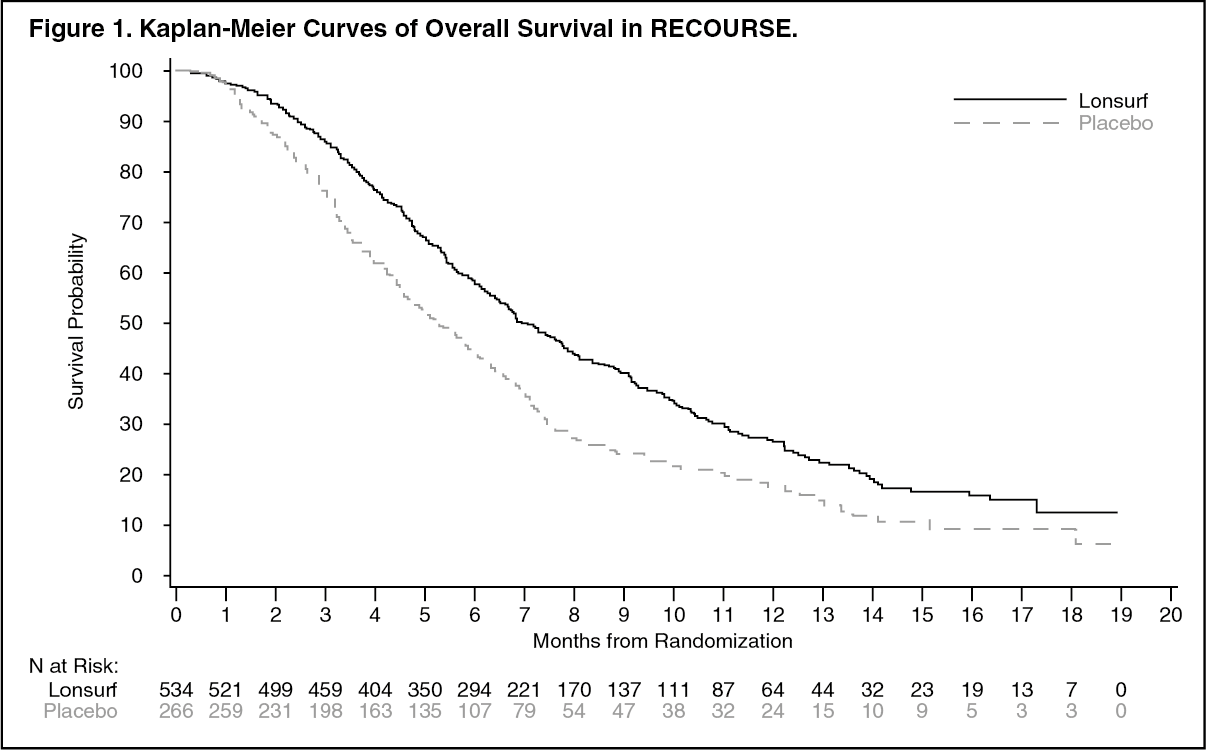 Click on icon to see table/diagram/image
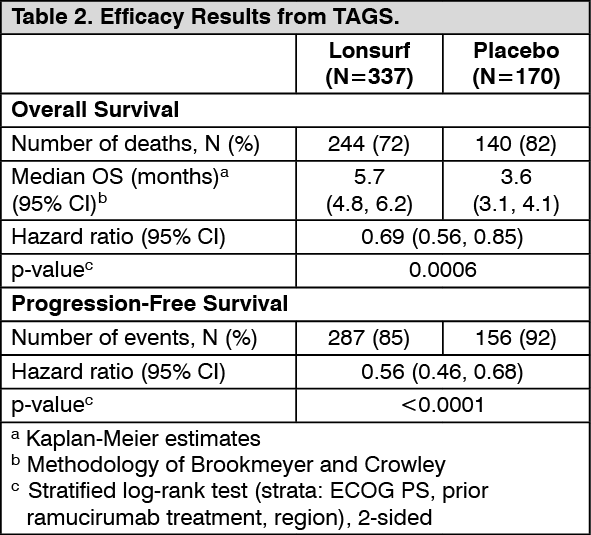
Click on icon to see table/diagram/imageMetastatic Gastric Cancer: The efficacy of Lonsurf was evaluated in the TAGS study (NCT02500043) an international, randomized, double-blind, placebo-controlled study in patients with metastatic gastric or gastroesophageal junction (GEJ) adenocarcinoma previously treated with at least 2 prior regimens for advanced disease. Previous treatments must have included a fluoropyrimidine, a platinum, and either a taxane or irinotecan. Patients with HER2/neu-positive tumors must have received prior HER2/neu-targeted therapy, if available. Adjuvant chemotherapy could be counted as one prior regimen in patients who had recurrence during or within 6 months of completion of the adjuvant chemotherapy. Other key eligibility criteria included ECOG performance status (PS) 0 or 1. Patients were randomized 2:1 to receive Lonsurf 35 mg/m2 orally twice daily on Days 1-5 and 8-12 of each 28-day cycle with best supportive care (BSC) or matching placebo with BSC until disease progression or unacceptable toxicity. Randomization was stratified by ECOG PS at baseline (0 vs. 1), prior ramucirumab (yes vs. no), and geographic region (Japan vs. rest of world). The major efficacy outcome measure was OS and an additional outcome measure was PFS.
A total of 507 patients were randomized to Lonsurf (N=337) or placebo (N=170). The median age was 63 years, 73% were male, 70% and 16% were White and Asian respectively, and 38% had a baseline ECOG PS of 0. Seventy-one percent of patients had gastric tumors, 29% had GEJ tumors, and two patients had gastric/GEJ tumors. All patients received platinum-based chemotherapy, 99% received fluoropyrimidine-based therapy, 91% received a taxane, 55% received irinotecan, and 33% received ramucirumab. The HER2 status was negative in 62%, positive in 19% and unknown in 20% of patients. Among the 94 patients with HER2 positive tumors, 89% received prior anti-HER2 therapy.
Efficacy results are summarized in Table 2 and Figure 2. (See Table 2 and Figure 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: After twice daily dosing of Lonsurf, systemic exposure (AUC) of trifluridine increased more than dose-proportionally over the dose range of 15 mg/m2 (0.43 times the recommended dose) to 35 mg/m2.
The accumulation of trifluridine was 3-fold for AUC0-12hr and 2-fold for Cmax at steady state while no accumulation was observed for tipiracil.
Administration of a single dose of Lonsurf 35 mg/m2 increased the mean AUC0-last of trifluridine by 37-fold and Cmax by 22-fold with reduced variability compared to administration of a single dose of trifluridine 35 mg/m2 alone.
Absorption: Following a single oral administration of Lonsurf at 35 mg/m2 in patients with cancer, the mean time to peak plasma concentration (Tmax) of trifluridine was around 2 hours.
Food Effect: A standardized high-fat, high-calorie meal decreased trifluridine Cmax, tipiracil Cmax and AUC by approximately 40%, but did not change trifluridine AUC compared to those in a fasting state in patients with cancer following administration of a single dose of Lonsurf 35 mg/m2. It is recommended to take Lonsurf within 1 hour after completion of the morning and evening meals based on the observed correlation between the increase in the Cmax of trifluridine and the decrease in neutrophil counts.
Distribution: Trifluridine mainly binds to human serum albumin. The in vitro protein binding of trifluridine in human plasma is ˃96%, independent of drug concentration and presence of tipiracil. Plasma protein binding of tipiracil is below 8%.
Elimination: After administration of Lonsurf 35 mg/m2, the mean elimination half-life (t1/2) of trifluridine was 1.4 hours and of tipiracil was 2.1 hours after a single dose. The mean elimination half-life at steady state of trifluridine was 2.1 hours and of tipiracil was 2.4 hours.
Metabolism: Trifluridine and tipiracil are not metabolized by cytochrome P450 (CYP) enzymes. Trifluridine is mainly eliminated by metabolism via thymidine phosphorylase to form an inactive metabolite, 5-(trifluoromethyl) uracil (FTY). No other major metabolites were detected in plasma or urine.
Excretion: After single oral administration of Lonsurf (60 mg) with [14C]-trifluridine, the total cumulative excretion of radioactivity was 60% of the administered dose. The majority of recovered radioactivity was eliminated into urine (55% of the dose) as FTY and trifluridine glucuronide isomers within 24 hours, and the excretion into feces and expired air was <3% for both. The unchanged trifluridine was <3% of administered dose recovered in the urine and feces.
After single oral administration of Lonsurf (60 mg) with [14C]-tipiracil hydrochloride, recovered radioactivity was 77% of the dose, which consisted of 27% urinary excretion and 50% fecal excretion. Tipiracil was the major component and 6-HMU was the major metabolite in urine, and feces.
Specific Populations: Based on the population pharmacokinetic analysis, there is no clinically relevant effect of age, sex, or race (White or Asian) on the pharmacokinetics of trifluridine or tipiracil.
Patients with Renal Impairment: In a dedicated renal impairment study, all patients received Lonsurf 35 mg/m2 twice daily except for patients with severe renal impairment who received 20 mg/m2 twice daily. Mild renal impairment (CLcr of 60 to 89 mL/min as determined by the Cockcroft-Gault formula) had no clinically important effect on steady-state AUC0-last of trifluridine and tipiracil. Moderate renal impairment (CLcr of 30 to 59 mL/min) increased steady-state AUC0-last of trifluridine by 56% and tipiracil by 139% compared to normal renal function (CLcr ≥90 mL/min). Severe renal impairment (CLcr of 15 to 29 mL/min) increased the dose-normalized steady-state AUC0-last of trifluridine by 140% and tipiracil by 614% compared to normal renal function. The pharmacokinetics of trifluridine and tipiracil have not been studied in patients with end-stage renal disease.
Patients with Hepatic Impairment: No clinically important differences in the mean exposures of trifluridine and tipiracil were observed between patients with mild hepatic impairment (total bilirubin ≤ ULN and AST ˃ ULN or total bilirubin ˃1 to 1.5 times ULN and any AST) to moderate hepatic impairment (total bilirubin ˃1.5 to 3 times ULN and any AST) and patients with normal hepatic function (total bilirubin and AST ≤ ULN); however, 5 of 6 patients with moderate hepatic impairment experienced Grade 3 or 4 increased bilirubin levels. The pharmacokinetics of trifluridine and tipiracil have not been studied in patients with severe hepatic impairment. [See Hepatic Impairment under Precautions.]
Drug Interaction Studies: In vitro studies indicated that trifluridine, tipiracil, and FTY did not inhibit the CYP enzymes and had no inductive effect on CYP1A2, CYP2B6, or CYP3A4/5.
In vitro studies indicated that trifluridine was not an inhibitor of or substrate for human uptake and efflux transporters.
Toxicology: Nonclinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: No long-term studies evaluating the carcinogenic potential of trifluridine/tipiracil in animals have been performed. Trifluridine/tipiracil was genotoxic in a reverse mutation test in bacteria, a chromosomal aberration test in mammalian-cultured cells, and a micronucleus test in mice.
Animal studies did not indicate an effect of trifluridine/tipiracil on male fertility in rats. Dose-related increases in the corpus luteum count and implanted embryo count were observed, but female fertility was not affected.