


 Sign Out
Sign Out

After proper training in injection technique, patients may self-inject with Humira if their physician determines that it is appropriate and with medical follow-up as necessary.
During treatment with Humira, other concomitant therapies (e.g., corticosteroids and/or immunomodulatory agents) should be optimised.
Posology: Rheumatoid arthritis (for 40 mg only): The recommended dose of Humira for adult patients with rheumatoid arthritis is 40 mg adalimumab administered every other week (eow) as a single dose via subcutaneous injection. Methotrexate should be continued during treatment with Humira.
Glucocorticoids, salicylates, nonsteroidal anti-inflammatory drugs, or analgesics can be continued during treatment with Humira. Regarding combination with disease modifying anti-rheumatic drugs other than methotrexate see Precautions and Pharmacology: Pharmacodynamics under Actions.
In monotherapy, some patients who experience a decrease in their response to Humira 40 mg every other week may benefit from an increase in dosage to 40 mg adalimumab every week or 80 mg every other week.
Available data suggest that the clinical response is usually achieved within 12 weeks of treatment. Continued therapy should be reconsidered in a patient not responding within this time period.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Dose interruption: There may be a need for dose interruption, for instance before surgery or if a serious infection occurs.
Available data suggest that re-introduction of Humira after discontinuation for 70 days or longer resulted in the same magnitudes of clinical response and similar safety profile as before dose interruption.
Ankylosing spondylitis, axial spondyloarthritis without radiographic evidence of AS and psoriatic arthritis (for 40 mg only): The recommended dose of Humira for patients with ankylosing spondylitis, axial spondyloarthritis without radiographic evidence of AS and for patients with psoriatic arthritis is 40 mg adalimumab administered every other week as a single dose via subcutaneous injection.
Available data suggest that the clinical response is usually achieved within 12 weeks of treatment. Continued therapy should be reconsidered in a patient not responding within this time period.
Psoriasis (for 40 mg only): The recommended dose of Humira for adult patients is an initial dose of 80 mg administered subcutaneously, followed by 40 mg subcutaneously given every other week starting one week after the initial dose.
Continued therapy beyond 16 weeks should be carefully reconsidered in a patient not responding within this time period.
Beyond 16 weeks, patients with inadequate response to Humira 40 mg every other week may benefit from an increase in dosage to 40 mg every week or 80 mg every other week. The benefits and risks of continued 40 mg weekly or 80 mg every other week therapy should be carefully reconsidered in a patient with an inadequate response after the increase in dosage (see Pharmacology: Pharmacodynamics under Actions). If adequate response is achieved with 40 mg every week or 80 mg every other week, the dosage may subsequently be reduced to 40 mg every other week.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Pre-filled pen: Beyond 16 weeks, patients with inadequate response may benefit from an increase in dosing frequency to 40 mg every week. The benefits and risks of continued weekly Humira therapy should be carefully reconsidered in a patient with an inadequate response after the increase in dosing frequency (see Pharmacology: Pharmacodynamics under Actions). If adequate response is achieved with an increased dosing frequency, the dose may subsequently be reduced to 40 mg every other week.
Hidradenitis suppurativa (for 40 mg only): The recommended Humira dose regimen for adult patients with hidradenitis suppurativa (HS) is 160 mg initially at Day 1 (given as four 40 mg injections in one day or as two 40 mg injections per day for two consecutive days), followed by 80 mg two weeks later at Day 15 (given as two 40 mg injections in one day). Two weeks later (Day 29) continue with a dose of 40 mg every week or 80 mg every other week (given as two 40 mg injections in one day). Antibiotics may be continued during treatment with Humira if necessary. It is recommended that the patient should use a topical antiseptic wash on their HS lesions on a daily basis during treatment with Humira.
Continued therapy beyond 12 weeks should be carefully reconsidered in a patient with no improvement within this time period.
Should treatment be interrupted, Humira 40 mg every week or 80 mg every other week may be re-introduced (see Pharmacology: Pharmacodynamics under Actions).
The benefit and risk of continued long-term treatment should be periodically evaluated (see Pharmacology: Pharmacodynamics under Actions).
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Crohn's disease (for 40 mg only): The recommended Humira induction dose regimen for adult patients with moderately to severely active Crohn's disease is 80 mg at Week 0 followed by 40 mg at Week 2. In case there is a need for a more rapid response to therapy, the regimen 160 mg at Week 0 (given as four 40 mg injections in one day or as two 40 mg injections per day for two consecutive days), 80 mg at Week 2 (given as two 40 mg injections in one day), can be used with the awareness that the risk for adverse events is higher during induction.
After induction treatment, the recommended dose is 40 mg every other week via subcutaneous injection. Alternatively, if a patient has stopped Humira and signs and symptoms of disease recur, Humira may be re‑administered. There is little experience from re‑administration after more than 8 weeks since the previous dose.
During maintenance treatment, corticosteroids may be tapered in accordance with clinical practice guidelines.
Some patients who experience decrease in their response to Humira 40 mg every other week may benefit from an increase in dosage to 40 mg Humira every week or 80 mg every other week.
Some patients who have not responded by Week 4 may benefit from continued maintenance therapy through Week 12. Continued therapy should be carefully reconsidered in a patient not responding within this time period.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Ulcerative colitis (for 40 mg only): The recommended Humira induction dose regimen for adult patients with moderate to severe ulcerative colitis is 160 mg at Week 0 (given as four 40 mg injections in one day or as two 40 mg injections per day for two consecutive days) and 80 mg at Week 2 (given as two 40 mg injections in one day). After induction treatment, the recommended dose is 40 mg every other week via subcutaneous injection.
During maintenance treatment, corticosteroids may be tapered in accordance with clinical practice guidelines.
Some patients who experience decrease in their response to 40 mg every other week may benefit from an increase in dosage to 40 mg Humira every week or 80 mg every other week.
Available data suggest that clinical response is usually achieved within 2-8 weeks of treatment. Humira therapy should not be continued in patients failing to respond within this time period.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Uveitis (for 40 mg only): The recommended dose of Humira for adult patients with uveitis is an initial dose of 80 mg, followed by 40 mg given every other week starting one week after the initial dose. There is limited experience in the initiation of treatment with Humira alone. Treatment with Humira can be initiated in combination with corticosteroids and/or with other non-biologic immunomodulatory agents. Concomitant corticosteroids may be tapered in accordance with clinical practice starting two weeks after initiating treatment with Humira.
It is recommended that the benefit and risk of continued long-term treatment should be evaluated on a yearly basis (see Pharmacology: Pharmacodynamics under Actions).
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Special populations: Elderly (for 40 mg only): No dose adjustment is required.
Renal and/or hepatic impairment (for 20 mg & 40 mg): Humira has not been studied in these patient populations. No dose recommendations can be made.
Paediatric population: Juvenile idiopathic arthritis (for 20 mg & 40 mg): Polyarticular juvenile idiopathic arthritis from 2 years of age: The recommended dose of Humira for patients with polyarticular juvenile idiopathic arthritis from 2 years of age is based on body weight (Table 24). Humira is administered every other week via subcutaneous injection. (See Table 24.)
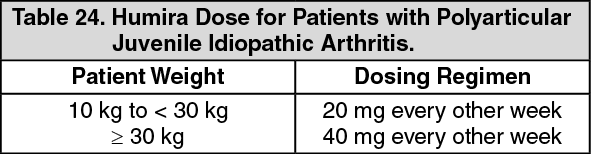 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAvailable data suggest that clinical response is usually achieved within 12 weeks of treatment. Continued therapy should be carefully reconsidered in a patient not responding within this time period.
There is no relevant use of Humira in patients aged less than 2 years for this indication.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Enthesitis-related arthritis: The recommended dose of Humira for patients with enthesitis-related arthritis from 6 years of age is based on body weight (Table 25). Humira is administered every other week via subcutaneous injection. (See Table 25.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHumira has not been studied in patients with enthesitis-related arthritis aged less than 6 years.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Paediatric plaque psoriasis (for 20 mg & 40 mg): The recommended Humira dose for patients with plaque psoriasis from 4 to 17 years of age is based on body weight (Table 26). Humira is administered via subcutaneous injection. (See Table 26.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageContinued therapy beyond 16 weeks should be carefully considered in a patient not responding within this time period.
If retreatment with Humira is indicated, the previously mentioned guidance on dose and treatment duration should be followed.
The safety of Humira in paediatric patients with plaque psoriasis has been assessed for a mean of 13 months.
There is no relevant use of Humira in children aged less than 4 years for this indication.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Adolescent hidradenitis suppurativa (from 12 years of age, weighing at least 30 kg) (for 40 mg only): There are no clinical trials with Humira in adolescent patients with HS. The posology of Humira in these patients has been determined from pharmacokinetic modelling and simulation (see Pharmacology: Pharmacokinetics under Actions).
The recommended Humira dose is 80 mg at Week 0 followed by 40 mg every other week starting at Week 1 via subcutaneous injection.
In adolescent patients with inadequate response to Humira 40 mg every other week, an increase in dosage to 40 mg every week or 80 mg every other week may be considered.
Antibiotics may be continued during treatment with Humira if necessary. It is recommended that the patient should use a topical antiseptic wash on their HS lesions on a daily basis during treatment with Humira.
Continued therapy beyond 12 weeks should be carefully reconsidered in a patient with no improvement within this time period.
Should treatment be interrupted, Humira may be re-introduced as appropriate.
The benefit and risk of continued long-term treatment should be periodically evaluated (see adult data in Pharmacology: Pharmacodynamics under Actions).
There is no relevant use of Humira in children aged less than 12 years in this indication.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Paediatric Crohn's disease (for 20 mg & 40 mg): The recommended dose of Humira for patients with Crohn's disease from 6 to 17 years of age is based on body weight (Table 27). Humira is administered via subcutaneous injection. (See Table 27.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients who experience insufficient response may benefit from an increase in dosage: < 40 kg: 20 mg every week; ≥ 40 kg: 40 mg every week or 80 mg every other week.
Continued therapy should be carefully considered in a subject not responding by week 12.
There is no relevant use of Humira in children aged less than 6 years for this indication.
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Paediatric Uveitis (for 20 mg & 40 mg): The recommended dose of Humira for paediatric patients with uveitis from 2 years of age is based on body weight (Table 28). Humira is administered via subcutaneous injection.
In paediatric uveitis, there is no experience in the treatment with Humira without concomitant treatment with methotrexate. (See Table 28.)
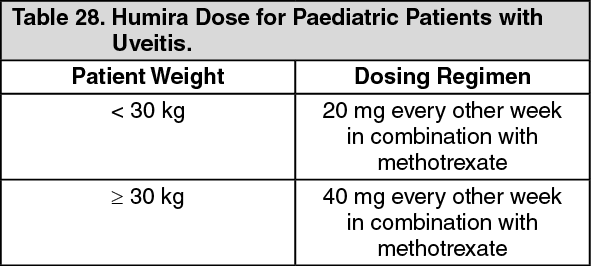 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen Humira therapy is initiated, a loading dose of 40 mg for patients < 30 kg or 80 mg for patients ≥ 30 kg may be administered one week prior to the start of maintenance therapy. No clinical data are available on the use of a Humira loading dose in children < 6 years of age (see Pharmacology: Pharmacokinetics under Actions).
There is no relevant use of Humira in children aged less than 2 years in this indication.
It is recommended that the benefit and risk of continued long-term treatment should be evaluated on a yearly basis (see Pharmacology: Pharmacodynamics under Actions).
Humira may be available in other strengths and/or presentations depending on the individual treatment needs.
Paediatric ulcerative colitis (for 40 mg only): The safety and efficacy of Humira in children aged 4-17 years have not yet been established. No data are available. There is no relevant use of Humira in children aged less than 4 years for this indication.
Psoriatic arthritis and axial spondyloarthritis including ankylosing spondylitis (for 40 mg only): There is no relevant use of Humira in the paediatric population for the indications of ankylosing spondylitis and psoriatic arthritis.
Method of administration: Humira is administered by subcutaneous injection. Full instructions for use are provided in the package leaflet.
Humira is available in other strengths and presentations.