Succinylated gelatin (modified fluid gelatin).
1000 ml of solution for infusion contain: Active substances: Succinylated Gelatine 40.0 g (modified fluid gelatine; average molecular weight: Mw (weight average) 30 000 daltons, Mn (number average) 23 200 daltons); Sodium chloride 7.01 g; Sodium hydroxide 1.36 g.
Electrolyte concentrations: Sodium 154 mmol/l, Chloride 120 mmol/l.
pH: 7.4 ± 0.3.
Theoretical osmolarity: 274 mOsm/l.
Gelation point: ≤ 3 °C.
The gelatine is prepared from the bones of cattle.
Excipients/Inactive Ingredients: Water for injections to 1000 ml.
Pharmacology: Gelofusine is a 4 % w/v solution of succinylated gelatine (also known as modified gelatine in solution) with an average molecular weight of 30 000 daltons (weight average). It has a relative viscosity of 1.9 at 37 °C and a colloid-osmotic pressure of 34 mmHg. The iso-electric point is at pH 4.5. The negative charges introduced into the molecule by succinylation lead to an expansion of the molecule, thus rendering it markedly more voluminous than unsuccinylated protein chains of the same molecular weight.
The characteristics of Gelofusine result in a sufficient volume effect over about 3 - 4 hours.
Therapeutic Effect: Gelofusine substitutes intravascular volume deficits caused by losses of blood or plasma. Thus the mean arterial pressure, the left-ventricular end-diastolic pressure, the cardiac stroke volume, the cardiac index, the oxygen supply and the diuresis are increased.
Mechanism of Action: The colloid-osmotic pressure of the solution determines the extent of its initial volume effect. The duration of the effect depends on the clearance of the colloid by re-distribution and excretion. The volume effect of Gelofusine is equivalent to the administered amount of solution. So Gelofusine is a plasma substitute, it does not have a plasma expanding effect. Lost plasma protein is not substituted by Gelofusine.
Pharmacokinetics: Absorption/Distribution: After infusion, Gelofusine is rapidly distributed in the intravascular but in part - regarding the low molecular weight fraction - also in the interstitial compartment. There is no evidence that Gelofusine is stored in the reticulo-endothelial system or elsewhere in the organism.
Metabolism/elimination: Most of the infused Gelofusine is excreted in urine. Only a minor amount is excreted in faeces and not more than about 1 % is metabolised. The smaller molecules are excreted directly by glomerular filtration while the larger molecules first are degraded proteolytically in the liver and then are also excreted in urine. The proteolytic metabolism is so adaptable that even under the condition of renal insufficiency no accumulation of gelatine is observed. After infusion for plasma volume substitution the half-life time of the intravascular effect of Gelofusine is 4 - 5 hours.
Pharmacokinetics in special clinical situations: The plasma half-life time of Gelofusine may be prolonged in patients on haemodialysis (GFR < 0.5 ml/min).
Toxicology: The toxicological studies on Gelofusine showed that the product is well tolerated. So, the maximum dose of the product is limited by its volume and dilution effects, not by any intrinsic toxicological properties.
Colloidal plasma volume substitute for prophylaxis and treatment of relative or absolute hypovolaemia.
Further, Gelofusine may be used as plasma volume substitute for: prophylaxis of hypotension, e.g. during induction of epidural or spinal anaesthesia; haemodilution; extra-corporal circulation (heart-lung machine, haemodialysis); vehicle solution for various medicaments, e.g. insulin.
Dosage and infusion rate are adjusted according to individual needs and are controlled by monitoring the usual circulatory parameters, e.g. blood pressure.
In order to avoid the occurrence of anaphylactoid/anaphylactic reactions described under Adverse Reactions, the first 20 - 30 ml should be infused slowly and under careful observation of the patient.
Recommended doses: For compensation of minor losses of blood or plasma as well as for pre- and intraoperative routine prophylaxis, as a rule, 500 - 1000 ml of Gelofusine will be required, being infused over 1 - 3 hours.
For compensation of major losses of blood or plasma, the average dose is between 1000 and 2000 ml.
In emergency situations or shock conditions, an initial dose of 500 ml may be administered by forced infusion over 5 - 10 min, using a pressure cuff or an infusion pump. Before starting infusion, the solution should be warmed to max. 37 °C. After stabilisation of the cardiovascular situation, the infusion can be continued with doses corresponding to the actual losses of blood or plasma. In this case, the amount of solution infused may be as much as 10 - 15 l/24 h. (Monitor haematocrit)
In isovolaemic haemodilution, the amount of infused solution corresponds to the withdrawn plasma volume. As a rule, a dose of 20 ml/kg BW should not be exceeded.
The amount of Gelofusine required during extracorporal circulation depends on the system used. Normally, volumes between 500 and 1000 ml are required.
Maximum daily dose: The therapeutic limit is dependent on the dilution effect. If the haematocrit falls below 25 % (in patients at cardiovascular or pulmonary risk, below 30 %), substitution of erythrocytes or full blood should be considered.
Maximum infusion rate: The maximum infusion rate depends on the actual cardio-circulatory situation.
Method of administration: Gelofusine is administered intravenously. Only solutions that are clear and free of precipitate should be infused.
Units once prepared ready for infusion must be used within the following 4 hours. Unused portions of the solution must not be stored for later use.
Overdose of Gelofusine may lead to unintended hypervolaemia associated with consecutive impairment of heart and lung function. As soon as symptoms of circulatory overload (headache, dyspnoea, jugular vein congestion) appear, the infusion must be stopped immediately.
Gelofusine must not be administered in the case of: hypersensitivity towards gelatine, hypervolaemia, hyperhydration, severe cardiac insufficiency, recent event of cardiac infarction, severe disturbances of blood coagulation, severe renal insufficiency.
Gelofusine should only be administered with caution in the cases of: known allergic diseases, e.g. asthma, hypernatraemia, haemorrhagic diathesis, states of dehydration, left or right ventricular insufficiency.
Special caution should be exercised and doses should be adjusted carefully in patients with: blood coagulation disorders, renal insufficiency, chronic liver diseases.
The following precautions should be observed: Electrolytes are to be substituted according to specific requirements.
Necessary monitoring: During compensation of severe blood losses by massive infusions of Gelofusine, the haematocrit must be monitored under any circumstances.
Likewise in those situations, the dilution effect on coagulation factors should be observed. (Critical values: platelet count below 50 000/μl, Quick's test and aPTT below 35 % of normal). Especially in patients with existing disorders of haemostasis, e.g. afibrinogenaemia, checks of the serum electrolyte concentrations are required. Special attention should be paid to the appearance of symptoms of hypocalcaemia (e.g. signs of tetany, paraesthesia); then corrective measures should be taken. This applies in particular to patients on medication with digitalis.
Because Gelofusine has no buffering capacity, it has no effect on acidosis.
Because the product does not substitute lost plasma protein, it is advisable to check the plasma protein concentrations 6 - 12 hours after an operation. If required, deficiencies should be corrected to a target level of 5 g/100 ml by infusion of human albumin. (It is necessary to observe the previously mentioned time of waiting because the biuret protein assay does not distinguish between gelatine and plasma proteins.)
Attention should be paid to the insufficiency of plasma protein stocks in infants, children, and the elderly.
Use in Children: Sufficient experience with application in children under 1 year is not available.
Pregnancy category C: Controlled studies have been carried out neither in animals nor in pregnant women.
Because of possible anaphylactoid or anaphylactic reactions, the preparation should only be administered during pregnancy, if its expected benefits definitely outweigh possible risks.
It is not known whether Gelofusine passes into breast milk. Sufficient experience with application during breast-feeding period is not available.
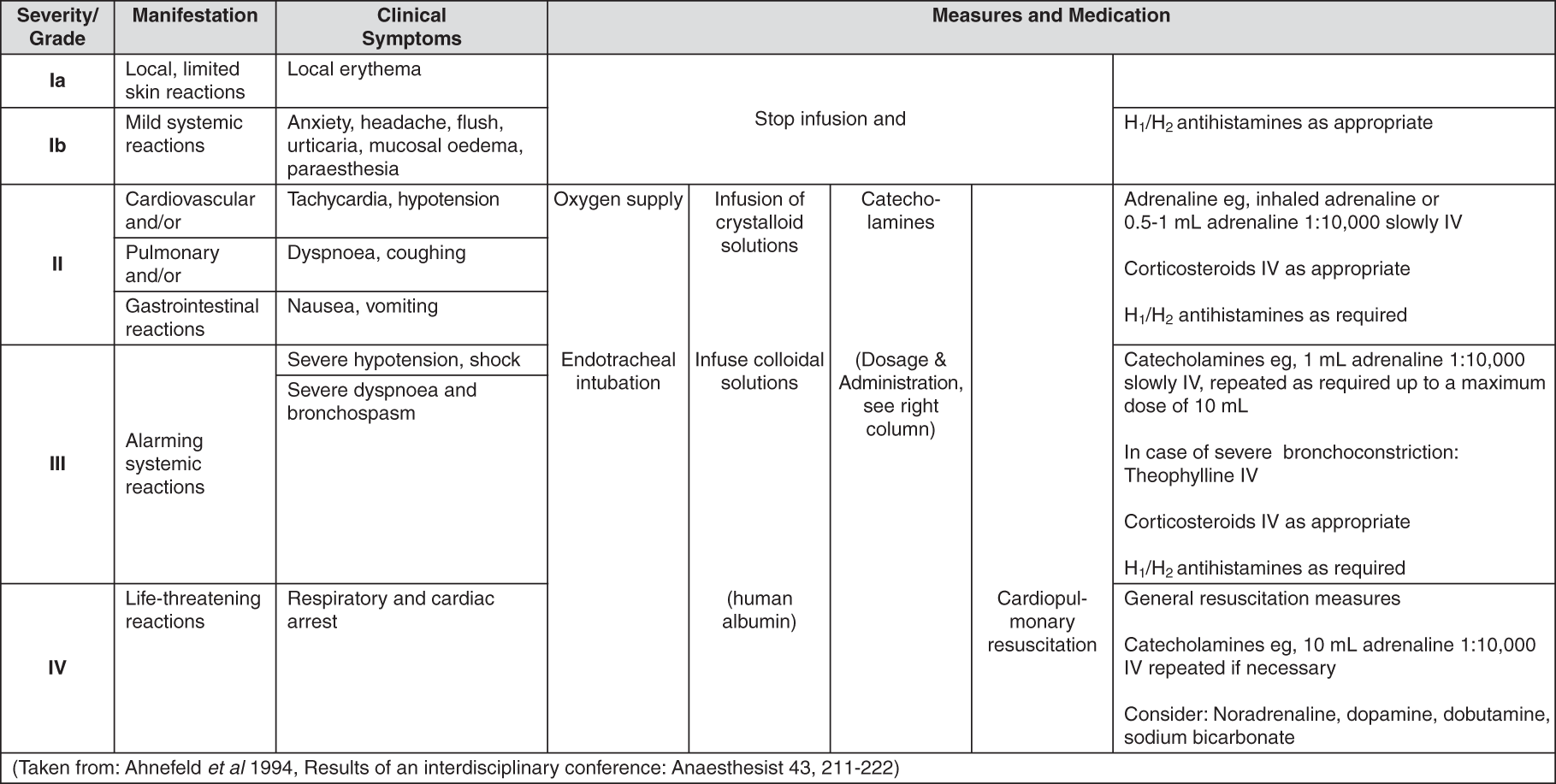
After the administration of Gelofusine infusions, just as of any colloidal volume substitutes, anaphylactoid or anaphylactic reactions of varying degrees of severity may occur. These reactions manifest as fever or cutaneous eruptions (urticaria) or sudden flushing of the face and neck. In rare cases, they may proceed over sudden flushing of the face and neck to drop in blood pressure, shock, cardiac and respiratory arrest.
Severe anaphylactoid reactions (grade III or IV) are rare with an incidence of about 1 : 13 000. Patients receiving Gelofusine must be continuously observed for the occurrence of anaphylactoid or anaphylactic reactions.
General guidelines for the prophylaxis of adverse reactions: Adequate information of physicians and nursing staff about the type and severity of possible adverse reactions that may be encountered after the administration of a colloidal volume substitute.
Close observation of the patient during infusion, especially while the first 20 - 30 ml of the solution are being infused.
Availability of all apparatus and medication required for resuscitation.
Stop of infusion immediately, as soon as there are any indications of adverse reactions.
It cannot be predicted by any test procedure which patients are likely to experience anaphylactic or anaphylactoid reactions, nor is it possible to foresee the course and severity of any such reaction. Anaphylactic or anaphylactoid reactions caused by gelatine solutions may either be histamine-mediated or histamine independent. Histamine release can be prevented by the use of a combination of H
1- and H
2-receptor blockers. Prophylactic administration of corticosteroids has not proved effective.
Adverse reactions may occur in conscious and anaesthetized patients. In the acute phase of volume deficiency shocks, so far no anaphylactic or anaphylactoid reaction has ever been reported. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Incompatibilities may occur when the solution is mixed with other medicaments.
Results of compatibility tests will be provided on request.
Admixture of fat emulsions must be avoided.
Influence on diagnostic methods: Gelofusine may have an influence on the following clinical-chemical tests, leading to falsely high values: Erythrocyte sedimentation rate, specific gravity of urine, unspecific plasma protein assays, e.g. by the biuret method.
Instructions for use: If the solution is administered by forced infusion, using a pressure cuff or on infusion pump, it should be warmed to body temperature before starting the infusion.
Incompatibilities: Incompatibilities may occur when the solution is mixed with other medicaments.
Gelofusine should not be stored above 25 °C.
B05AA06 - gelatin agents ; Belongs to the class of blood substitutes and plasma protein fractions. Used as blood substitutes.
Gelofusine infusion
500 mL x 10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
