


 Sign Out
Sign Out




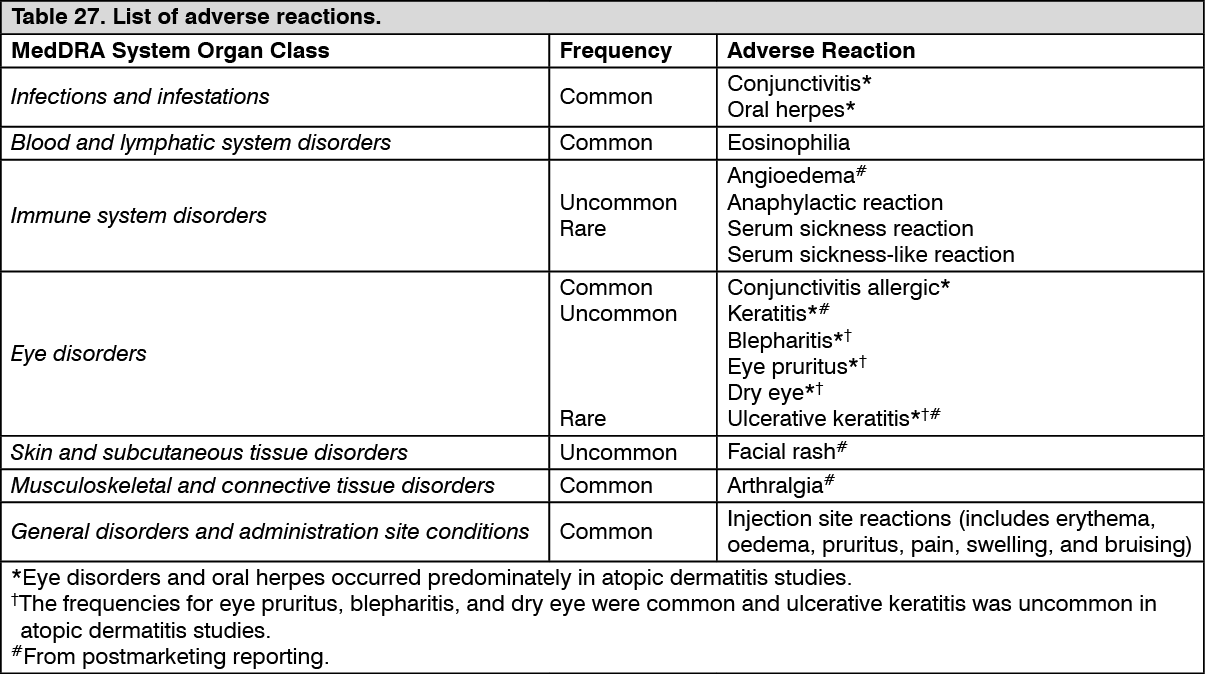
Tabulated list of adverse reactions: The dupilumab safety data presented in Table 27 were predominantly derived from 12 randomised, placebo-controlled trials, including atopic dermatitis, asthma, and CRSwNP patients. These studies involved 4,206 patients receiving dupilumab and 2,326 patients receiving placebo during the controlled period are representative of the overall safety profile for dupilumab.
Listed in Table 27 are adverse reactions observed in clinical trials and/or postmarketing setting presented by system organ class and frequency, using the following categories: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. (See Table 27.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Hypersensitivity: Cases of anaphylactic reaction, angioedema, and serum sickness/serum sickness-like reactions have been reported following administration of dupilumab (see Precautions).
Conjunctivitis and keratitis related events: Conjunctivitis and keratitis occurred more frequently in atopic dermatitis patients who received dupilumab compared to placebo in atopic dermatitis studies. Most patients with conjunctivitis or keratitis recovered or were recovering during the treatment period. In the long-term OLE atopic dermatitis study (AD-1225) at 5 years, the respective rates of conjunctivitis and keratitis remained similar to those in the dupilumab arm in the placebo controlled atopic dermatitis studies. Among asthma patients frequency of conjunctivitis and keratitis was low and similar between dupilumab and placebo. Among CRSwNP and Prurigo Nodularis (PN) patients the frequency of conjunctivitis was higher in dupilumab than placebo, though lower than that observed in atopic dermatitis patients. There were no cases of keratitis reported in the CRSwNP or PN development program. Among patients with EoE, the frequency of conjunctivitis was low and similar between dupilumab and placebo groups. There were no cases of keratitis in the EoE development program (see Precautions).
Eczema herpeticum: Eczema herpeticum was reported in <1% of the dupilumab groups and in <1% of the placebo group in the 16-week atopic dermatitis monotherapy studies. In the 52-week atopic dermatitis dupilumab + TCS study, eczema herpeticum was reported in 0.2% of the dupilumab + TCS group and 1.9% of the placebo + TCS group. These rates remained stable at 5 years in the long-term OLE study (AD-1225).
Eosinophilia: Dupilumab-treated patients had a greater mean initial increase from baseline in eosinophil count compared to patients treated with placebo in the atopic dermatitis, asthma, and CRSwNP indications. Eosinophil counts declined to near baseline levels during study treatment and returned to baseline during the asthma open-label extension safety study (TRAVERSE). The mean blood eosinophil levels decreased to below baseline by week 20 and was maintained up to 5 years in the long-term OLE study (AD-1225). Compared to placebo, no increase in mean blood eosinophil counts was observed in PN (PRIME and PRIME2). Mean and median blood eosinophil counts declined to near baseline or remained below baseline levels in EoE (TREET Parts A and B) during study treatment.
Treatment-emergent eosinophilia (≥5,000 cells/mcL) was reported in <3% of dupilumab-treated patients and <0.5% in placebo-treated patients (SOLO1, SOLO2, AD-1021, DRI12544, QUEST, and VOYAGE; SINUS-24 and SINUS-52, PRIME, and PRIME2 studies; TREET Parts A and B).
Treatment-emergent eosinophilia (≥ 5,000 cells/mcL) was reported in 8.4 % of dupilumab-treated patients and 0 % in placebo-treated patients in study AD-1539, with median eosinophil counts declining below baseline at end of treatment period.
Infections: In the 16-week atopic dermatitis monotherapy clinical studies, serious infections were reported in 1.0% of patients treated with placebo and 0.5% of patients treated with dupilumab. In the 52-week atopic dermatitis CHRONOS study, serious infections were reported in 0.6% of patients treated with placebo and 0.2% of patients treated with dupilumab. The rates of serious infections remained stable at 5 years in the long-term OLE study (AD-1225).
No increase was observed in the overall incidence of infections with dupilumab compared to placebo in the safety pool for asthma clinical studies. In the 24-week safety pool, serious infections were reported in 1.0% of patients treated with dupilumab and 1.1% of patients treated with placebo. In the 52-week QUEST study, serious infections were reported in 1.3% of patients treated with dupilumab and 1.4% of patients treated with placebo.
No increase was observed in the overall incidence of infections with dupilumab compared to placebo in the safety pool for CRSwNP clinical studies. In the 52-week SINUS-52 study, serious infections were reported in 1.3% of patients treated with dupilumab and 1.3% of patients treated with placebo.
No increase was observed in the overall incidence of infections with dupilumab compared to placebo in the safety pool for PN clinical studies. In the safety pool, serious infections were reported in 1.3 % of patients treated with dupilumab and 1.3 % of patients treated with placebo.
The overall incidence of infections was numerically higher with dupilumab (32.0 %) compared to placebo (24.8 %) in the safety pool for EoE TREET (Parts A and B) studies. In the 24-week safety pool, serious infections were reported in 0.5 % of patients treated with dupilumab and 0 % of patients treated with placebo.
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity with dupilumab.
Anti-Drug-Antibodies (ADA) responses were not generally associated with impact on dupilumab exposure, safety, or efficacy.
Approximately 5% of patients with atopic dermatitis, asthma, or CRSwNP who received dupilumab 300 mg Q2W for 52 weeks developed ADA to dupilumab; approximately 2% exhibited persistent ADA responses and approximately 2% had neutralizing antibodies. Similar results were observed in adult patients with PN who received dupilumab 300 mg Q2W for 24 weeks, paediatric patients (6 months to 11 years of age) with atopic dermatitis who received dupilumab 200 mg Q2W or 300 mg Q4W for 16 weeks and patients (6 to 11 years of age) with asthma who received dupilumab 100 mg Q2W or 200 mg Q2W for 52 weeks. Similar ADA responses were observed in adult patients with atopic dermatitis treated with dupilumab for up to 5 years in the long-term OLE study (AD-1225).
Approximately 16% of adolescent patients with atopic dermatitis who received dupilumab 300 mg or 200 mg Q2W for 16 weeks developed antibodies to dupilumab; approximately 3% exhibited persistent ADA responses, and approximately 5% had neutralizing antibodies.
Approximately 9% of patients with asthma who received dupilumab 200 mg Q2W for 52 weeks developed antibodies to dupilumab; approximately 4% exhibited persistent ADA responses and approximately 4% had neutralizing antibodies.
Approximately 1 % of patients with EoE who received dupilumab 300 mg QW or 300 mg Q2W for 24 weeks developed antibodies to dupilumab; 0 % exhibited persistent ADA responses and approximately 0.5 % had neutralizing antibodies.
Regardless of age or population, up to 4% of patients in the placebo groups were positive for antibodies to dupilumab; approximately 2% exhibited persistent ADA response and approximately 1% had neutralizing antibodies.
Less than 1% of patients who received dupilumab at approved dosing regimens exhibited high titer ADA responses associated with reduced exposure and efficacy. In addition, there was one patient with serum sickness and one with serum sickness-like reaction (<0.1%) associated with high ADA titers (see Precautions).
Paediatric population: Atopic Dermatitis: Adolescents 12 to 17 years of age: The safety of dupilumab was assessed in a study of 250 patients 12 to 17 years of age with moderate-to-severe atopic dermatitis (AD-1526). The safety profile of dupilumab in these patients followed through week 16 was similar to the safety profile from studies in adults with atopic dermatitis.
Children 6 to 11 years of age: The safety of dupilumab was assessed in a study of 367 patients 6 to 11 years of age with severe atopic dermatitis (AD-1652). The safety profile of dupilumab with concomitant TCS in these patients through week 16 was similar to the safety profile from studies in adults and adolescents with atopic dermatitis.
Children 6 months to 5 years of age: The safety of dupilumab with concomitant TCS was assessed in a study of 161 patients 6 months to 5 years of age with moderate-to-severe atopic dermatitis, which included a subgroup of 124 patients with severe atopic dermatitis (AD-1539). The safety profile of dupilumab with concomitant TCS in these patients through week 16 was similar to the safety profile from studies in adults and paediatric patients 6 to 17 years of age with atopic dermatitis.
Atopic Hand and Foot Dermatitis: The safety of dupilumab was assessed in 27 paediatric patients 12 to 17 years of age with moderate-to-severe atopic hand and foot dermatitis (AD-1924). The safety profile of dupilumab in these patients through Week 16 was consistent with the safety profile from studies in adult and paediatric patients 6 months of age and older with moderate-to-severe AD.
Asthma: Adolescents (12 to 17 years of age): A total of 107 adolescents aged 12 to 17 years with asthma were enrolled in the 52 week QUEST study. The safety profile observed was similar to that seen in adults.
The long-term safety of dupilumab was assessed in 89 adolescent patients who were enrolled in an open-label extension study in moderate-to-severe asthma (TRAVERSE). In this study, patients were followed for up to 96 weeks. The safety profile of dupilumab in TRAVERSE was consistent with the safety profile observed in pivotal asthma studies for up to 52 weeks of treatment.
Children 6 to 11 years of age: In children 6 to 11 years of age with moderate-to-severe asthma (VOYAGE), the additional adverse reaction of enterobiasis was reported in 1.8 % (5 patients) in the dupilumab groups and none in the placebo group. All enterobiasis cases were mild to moderate and patients recovered with anti-helminth treatment without dupilumab treatment discontinuation.
In children 6 to 11 years of age with moderate-to-severe asthma, eosinophilia (blood eosinophils ≥ 3,000 cells/mcL or deemed by the investigator to be an adverse event) was reported in 6.6 % of the dupilumab groups and 0.7% in the placebo group. Most eosinophilia cases were mild to moderate and not associated with clinical symptoms. These cases were transient, decreased over time, and did not lead to dupilumab treatment discontinuation.
The long-term safety of dupilumab was assessed in an open-label extension study (EXCURSION) in children 6 to 11 years of age with moderate-to-severe asthma who previously participated in VOYAGE. Among 365 patients who entered EXCURSION, 350 completed 52 weeks of treatment and 228 patients completed a cumulative treatment duration of 104 weeks (VOYAGE and EXCURSION). The long-term safety profile of dupilumab in EXCURSION was consistent with the safety profile observed in the pivotal asthma study (VOYAGE) for 52 weeks of treatment.
EoE: A total of 99 adolescents aged 12 to 17 years with EoE were enrolled in the TREET (Parts A and B) studies. The safety profile observed was similar to that seen in adults.
Long-term safety: Atopic Dermatitis: The safety profile of dupilumab + TCS (CHRONOS) in adult atopic dermatitis patients through week 52 was consistent with the safety profile observed at week 16. The long-term safety of dupilumab was assessed in an open-label extension study in patients 6 months to 17 years of age with moderate-to-severe atopic dermatitis (AD-1434). The safety profile of dupilumab in patients followed through week 52 was similar to the safety profile observed at week 16 in the AD-1526, AD-1652 studies, and AD-1539 studies. The long-term safety profile of dupilumab observed in children and adolescents was consistent with that seen in adults with atopic dermatitis.
In a phase 3, multicentre, open-label extension (OLE) study (AD-1225), the long-term safety of repeat doses of dupilumab was assessed in 2,677 adults with moderate-to-severe AD exposed to 300 mg weekly dosing (99.7%), including 179 who completed at least 260 weeks of the study. The long-term safety profile observed in this study up to 5 years was generally consistent with the safety profile of dupilumab observed in controlled studies.
Asthma: The safety profile of dupilumab in the 96 weeks long-term safety study (TRAVERSE) was consistent with the safety profile observed in pivotal asthma studies for up to 52 weeks of treatment.
The safety profile of dupilumab in children with asthma 6 to 11 years of age who participated in the 52 weeks long-term safety study (EXCURSION) was consistent with the safety profile observed in the pivotal asthma study (VOYAGE) for 52 weeks of treatment.
CRSwNP: The safety profile of dupilumab in adults with CRSwNP through week 52 was consistent with the safety profile observed at week 24.
Eosinophilic esophagitis: The safety profile of dupilumab through week 52 was generally consistent with the safety profile observed at week 24.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form