Each tablet contains: Flupentixol 0.5 mg (as 0.584 mg flupentixol dihydrochloride), Melitracen 10 mg (as 11.25 mg melitracen hydrochloride).
Excipients with known effect: Lactose monohydrate.
Excipients/Inactive Ingredients: Tablet core: Betadex, Lactose monohydrate, Maize starch, Hydroxypropylcellulose, Microcrystalline cellulose, Croscarmellose sodium, Talc, Hydrogenated vegetable oil, Magnesium stearate.
Coating: Polyvinyl alcohol part. hydrolyzed, Macrogol 3350, Talc, Macrogol 6000.
Colours: Titanium dioxide E 171, Erythrosine E 127, Indigotine E 132.
Pharmacotherapeutic group: Antidepressants - Tricyclic antidepressant (melitracen) and neuroleptic of the thioxanthene group (flupentixol). ATC-code: N 06 CA 02.
Pharmacology: Pharmacodynamics: Deanxit consists of two well known and well proven compounds: Flupentixol is a neuroleptic of the thioxanthene group with anxiolytic and antidepressant properties when given in small doses.
Melitracen is a tricyclic antidepressant with activating properties in low doses. It has similar pharmacological properties as amitriptyline but is less sedative.
In combination the compounds render a preparation with antidepressant, anxiolytic and activating properties.
Pharmacokinetics: Flupentixol: Flupentixol is a mixture of two geometric isomers, the active cis(Z)-flupentixol and trans(E)-flupentixol, approximately in the ratio of 1:1.
Absorption: Oral administration results in maximum serum levels in about 12 hours. Oral bioavailability is about 40%.
Distribution: The apparent volume of distribution (Vd)β is about 14.1 l/kg.
The plasma protein binding is about 99%.
Biotransformation: The metabolism of flupentixol proceeds along three main routes - sulphoxidation, side chain N-dealkylation and glucuronic acid conjugation. The metabolites are devoid of psychopharmacological activity. Flupentixol dominates over metabolites in brain and other tissues.
Elimination: The elimination half-life (T1/2 β) is about 61 hours and the mean systemic clearance (Cls) is about 0.29 l/min.
Flupentixol is excreted mainly with faeces, but also to some degree with the urine. When tritium labelled flupentixol was administered to man the excretion pattern shows the excretion via faeces to be about 4 times the urinary excretion.
In nursing mothers flupentixol is excreted in small amounts with the breast milk. The ratio milk conc./serum conc. in women is on average 1.3.
Linearity: The kinetics is linear. Steady state plasma levels are achieved in about 7 days. The mean minimum steady state level corresponding to 5 mg flupentixol orally once-a-day was about 1.7 ng/ml (3.9 nmol/l).
Older people: Pharmacokinetic investigations have not been done in elderly patients. However, for the related thioxanthene drug, zuclopenthixol, the pharmacokinetic parameters are widely independent of the age of the patient.
Reduced hepatic function: No data available.
Reduced renal function: Based on the previously mentioned characteristics for elimination it is reasonable to assume that reduced kidney function is likely not to have much influence on the serum levels of parent drug.
Melitracen: Absorption: Oral administration results in maximum serum levels in about 5 hours. Oral bioavailability is not known.
Distribution: The apparent volume of distribution (Vd)β is not known. The plasma protein binding in rats is about 89%.
Biotransformation: The metabolism of melitracen proceeds mainly by demethylation and hydroxylation. The main active metabolite is the secondary amine, litracen.
Elimination: The elimination half-life (T1/2 β) is about 62 hours in man. The systemic clearance (CLs) is not known.
In rats melitracen is excreted mainly with faeces, but also to some degree with the urine. The excretion pattern showed the excretion via faeces to be about 2½ times the urinary excretion.
It is not known whether melitracen is excreted with breast milk.
Older people: No data available.
Reduced hepatic function: No data available.
Reduced renal function: No data available.
Toxicology: Preclinical safety data: Acute toxicity: Flupentixol has low acute toxicity, but the acute toxicity of tricyclic antidepressants including melitracen is high.
Chronic toxicity: In chronic toxicity studies there were no findings of concern for the therapeutic use of flupentixol or melitracen.
Reproduction toxicity: In preclinical fertility studies in rats, where flupentixol and melitracen were administered separately slight effects on fertility were noted. Flupentixol slightly affected the pregnancy rate of female rats, whereas melitracen slightly repressed fertility and fecundity of male rats. Effects were seen at doses well in excess of those applied during clinical use.
Combination of flupentixol and melitracen did not induce major malformations or affect pregnancy and embryofoetal development in rats or rabbits. In mice melitracen was associated with lower foetal body weight, but no major malformations were noted.
No effect on parturition or postnatal development of melitracen was noted in mice or rats.
Anxiety - Depression - Asthenia.
Neurasthenia. Psychogenic depression. Depressive neuroses. Masked depression. Psychosomatic affections accompanied by anxiety and apathy. Menopausal depressions. Dysphoria and depression in alcoholics and drug-addicts.
Posology: Adults: Usually 2 tablets daily: morning and noon.
In severe cases the morning dose may be increased to 2 tablets.
The maximum dose is 4 tablets daily.
Older people (> 65 years): 1 tablet in the morning.
In severe cases 1 tablet in the morning and 1 at noon.
Maintenance dose: Usually 1 tablet in the morning.
In case of insomnia or severe restlessness additional treatment with a sedative in the acute phase is recommended.
Paediatric population: Children and adolescents (<18 years): Deanxit is not recommended for use in children and adolescents due to lack of data on safety and efficacy.
Reduced renal function: Deanxit can be given in the recommended doses.
Reduced liver function: Deanxit can be given in the recommended doses.
Method of administration: The tablets are swallowed with water.
In cases of overdosage the symptoms of intoxication by melitracen, especially of anticholinergic nature, dominate. More rarely extrapyramidal disorder due to flupentixol occur.
Symptoms: Somnolence, irritability, agitation, hallucinations. anticholinergic effects (mydriasis, tachycardia, urinary retention, mucosal dryness, intestinal hypomotility), convulsions, pyrexia, depressed level of consciousness, coma, respiratory depression, cardiac symptoms (arrhythmias (ventricular arrhythmia, torsade de pointes, ventricular fibrillation), cardiac failure, hypotension, cardiogenic shock), metabolic acidosis, hypokalaemia.
Treatment: Admission to hospital (intensive care unit). Treatment is symptomatic and supportive. Gastric aspiration and lavage even in a late stage after oral ingestion and treatment with activated charcoal. Measures to support the respiratory and cardiovascular systems should be instituted. Continuous ECG-monitoring of cardiac function for 3-5 days. Epinephrine (adrenaline) should not be used as further lowering of blood pressure may result. Convulsions may be treated with diazepam and extrapyramidal disorder with biperiden.
Adults have survived consumption of up to 100 tablets (1000 mg melitracen and 50 mg flupentixol) and an almost 3-year old child 27 tablets (270 mg melitracen and 13.5 mg flupentixol).
Hypersensitivity to flupentixol and melitracen or to any of the excipients listed in Description.
Circulatory collapse, depressed level of consciousness due to any cause (e.g. intoxication with alcohol, barbiturates or opiates), coma, blood disorders, phaeochromocytoma.
Recent myocardial infarction. Any degree of atrioventricular block or disorders of cardiac rhythm and coronary artery insufficiency.
Concomitant treatment with MAOIs (monoamine oxidase inhibitors) is contraindicated (see Interactions).
Simultaneous administration of melitracen and MAO inhibitors may cause serotonin syndrome (a combination of symptoms, possibly including agitation, confusion, tremor, myoclonus and hyperthermia).
As with other tricyclic antidepressants, melitracen should not be given to patients receiving monoamine oxidase inhibitors (MAOIs). Treatment with Deanxit may be instituted 14 days after discontinuation of non-selective MAOIs and minimum one day after discontinuation of moclobemide and selegiline. Treatment with MAOIs may be introduced 14 days after discontinuation of Deanxit.
Deanxit should not be administered together with MAOIs (see Contraindications and Interactions).
Deanxit should be used with caution in patients with organic brain syndrome, convulsion, urinary retention, hyperthyroidism and advanced hepatic or cardiovascular disease.
Not recommended for excitable or overactive patients since its activating effect may lead to exaggeration of these characteristics. If the patient has previously been treated with tranquillizers or neuroleptics with sedative effect, these should be withdrawn gradually.
The possibility of development of neuroleptic malignant syndrome (hyperthermia, muscle rigidity, fluctuating consciousness, instability of the autonomous nervous system) exists with any neuroleptic.
As with other drugs belonging to the therapeutic class of antipsychotics, Deanxit may cause QT prolongation. Persistently prolonged QT intervals may increase the risk of malignant arrhythmias. Therefore, Deanxit should be used with caution in susceptible individuals (with hypokalaemia, hypomagnesia or genetic predisposition) and in patients with a history of cardiovascular disorders, e.g. QT prolongation, significant bradycardia (<50 beats per minute), a recent acute myocardial infarction, uncompensated heart failure, or cardiac arrhythmia. Concomitant treatment with other drugs which may cause QT prolongation is contraindicated (see Interactions).
Serotonergic psychiatric drugs should not be started in a patient receiving linezolid. Wait until 24 hours after the last dose of linezolid before starting the serotonergic psychiatric drugs.
Suicide / suicidal thoughts or clinical worsening: Depression is associated with an increased risk of suicidal thoughts, self-harm and suicide (suicide-related events). This risk persists until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored until such improvement occurs. It is general clinical experience that the risk of suicide may increase in the early stages of recovery.
Patients with a history of suicide-related events, or those exhibiting a significant degree of suicidal ideation prior to commencement of treatment, are known to be at greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. A meta-analysis of placebo-controlled clinical trials of antidepressant drugs in adult patients with psychiatric disorders showed an increased risk of suicidal behaviour with antidepressants compared to placebo in patients less than 25 years old.
Close supervision of patients and in particular those at high risk should accompany drug therapy especially in early treatment and following dose changes. Patients (and caregivers of patients) should be alerted about the need to monitor for any clinical worsening, suicidal behaviour or thoughts and unusual changes in behaviour and to seek medical advice immediately if these symptoms present.
As described for other psychotropics Deanxit may modify insulin and glucose responses calling for adjustment of the antidiabetic therapy in diabetic patients.
In patients with the rare condition of shallow anterior chamber and narrow chamber angle, attacks of acute glaucoma due to dilation of the pupil may be provoked.
Anaesthetics given during tri/tetracyclic antidepressant therapy may increase the risk of arrhythmias and hypotension. If possible, discontinue Deanxit several days before surgery; if emergency surgery is unavoidable, the anaesthetist should be informed that the patient is being so treated.
Deanxit should be used with caution in patients receiving SSRIs.
Excipients: The tablets contain lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Deanxit is a non-sedating drug in the recommended dosage range.
However, patients who are prescribed psychotropic medication may be expected to have some impairment in general attention and concentration and should be cautioned about their ability to drive or operate machinery.
Use in Children: Use in children and adolescents under the age of 18: Deanxit is not recommended for use in children and adolescents due to lack of data on efficacy and safety.
Venous thromboembolism (VTE): Cases of venous thromboembolism (VTE) have been reported with antipsychotic drugs. Since patients treated with antipsychotics often present with acquired risk factors for VTE, all possible risk factors for VTE should be identified before and during treatment with Deanxit and preventive measures undertaken.
Use in the Elderly: Cerebrovascular: An approximately 3-fold increased risk of cerebrovascular adverse events have been seen in randomized placebo controlled clinical trials in the dementia population with some atypical antipsychotics. The mechanism for this increased risk is not known. An increased risk cannot be excluded for other antipsychotics or other patient populations. Deanxit should be used with caution in patients with risk factors for stroke.
Increased mortality in older people with dementia: Data from two large observational studies showed that elderly people with dementia who are treated with antipsychotics are at a small increased risk of death compared with those who are not treated. There are insufficient data to give a firm estimate of the precise magnitude of the risk and the cause of the increased risk is not known.
Deanxit is not licensed for the treatment of dementia-related behavioural disturbances.
Pregnancy: Deanxit should not be administered during pregnancy unless the expected benefit to the patient outweighs the theoretical risk to the foetus. Due to the risk of neonatal withdrawal symptoms it is recommended that Deanxit treatment is stopped about 14 days before delivery by tapering off the dosage.
Neonates exposed to antipsychotics (including Deanxit) during the third trimester of pregnancy are at risk of adverse reactions including extrapyramidal and/or withdrawal symptoms that may vary in severity and duration following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress, or feeding disorder. Consequently, newborns should be monitored carefully.
Animal studies have shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Breast-feeding: As flupentixol is found in breast milk in low concentrations it is not likely to affect the infant when therapeutic doses are used. The dose ingested by the infant is less than 0.5% of the weight related maternal dose (in mg/kg).
It is not known whether melitracen is excreted in breast milk. However, another tricyclic antidepressant, amitriptyline, is found in breast milk in low concentrations and it is not likely to affect the infant when therapeutic doses are used. The dose ingested by the infant is about 2% of the weight related maternal daily dose (in mg/kg). As melitracen has the same lipophilic properties as amitriptyline, it is assumed that it occurs in breast milk in similar concentrations.
Breast-feeding can be continued during Deanxit therapy if considered of clinical importance but observation of the infant is recommended, particularly in the first 4 weeks after giving birth.
Fertility: In humans, adverse events have been reported that may have a negative impact on female and/or male sexual function and fertility. If clinically significant hyperprolactinaemia, galactorrhoea, amenorrhoea or sexual dysfunctions occur, a dose reduction (if possible) or discontinuation should be considered.
The effect is reversible on discontinuation.
In preclinical fertility studies in rats, where flupentixol and melitracen were administered separately slight effects on fertility were noted. Flupentixol slightly affected the pregnancy rate of female rats, whereas melitracen slightly repressed fertility and fecundity of male rats. Effects were seen at doses well in access of these applied during clinical use.
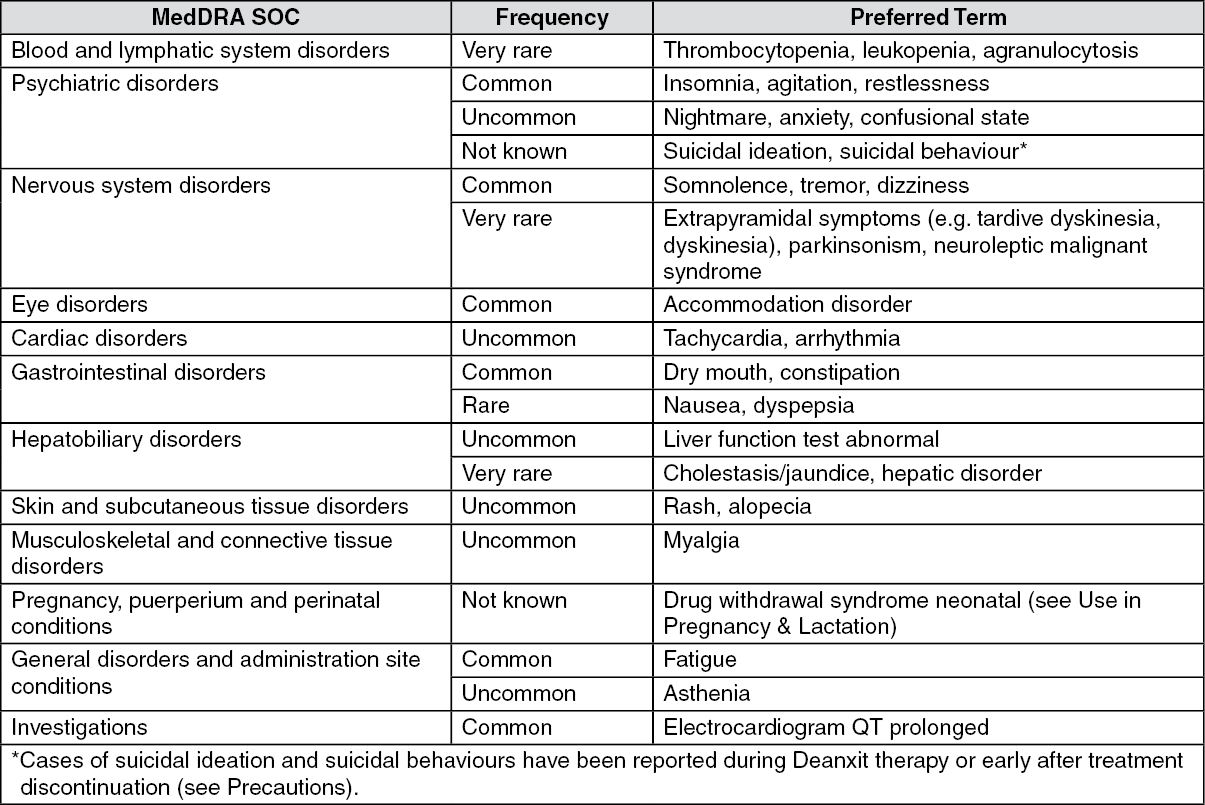
Dryness of the mouth, dizziness, tremor, nervousness, blurred vision, and insomnia are the most frequent undesirable effects and occur commonly.
In the listing as follows, the following convention is used: MedDRA system organ class / preferred term.
Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000) or not known (cannot be estimated from available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Cases of withdrawal syndrome have occurred.
Cases of venous thromboembolism, including cases of pulmonary embolism and cases of deep vein thrombosis have been reported with antipsychotic drugs with unknown frequency.
Post marketing: Isolated cases of cholestatic hepatitis have been reported.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions to:
Pharmacovigilance Unit
Drug Office, Department of Health
Room 1856, Wu Chung House,
213 Queen's Road East, Wanchai
Hong Kong
Phone: 2319 2920
Fax: 2186 9845
Email: adr@dh.gov.hk
http://www.drugoffice.gov.hk
Contraindicated combinations: MAOIs (non-selective as well as selective A (moclobemide) and B (selegiline)): risk of "serotonin syndrome" (see Contraindications).
Inadvisable combinations: Sympathomimetic agents: Melitracen may potentiate the cardiovascular effects of adrenaline, ephedrine, isoprenaline, noradrenaline, phenylephrine, and phenylpropanolamine (e.g. as contained in local and general anaesthetics and nasal decongestants).
Adrenergic neurone blockers: Deanxit may counteract the antihypertensive effects of guanethidine, betanidine, reserpine, clonidine and methyldopa. It is advisable to review all antihypertensive therapy during treatment with tricyclic antidepressants.
Anticholinergic agents: Tricyclic antidepressants may potentiate the effects of these drugs on the eye, central nervous system, bowel and bladder; concomitant use of these should be avoided due to an increased risk of paralytic ileus, hyperpyrexia, etc.
Drugs which may increase the QT interval: Increases in the QT interval related to antipsychotic treatment may be exacerbated by the co-administration of other drugs known to significantly increase the QT interval. Co-administration of such drugs should be avoided. Relevant classes include: class Ia and III antiarrhythmics (e.g. quinidine, amiodarone, sotalol, dofetilide); some antipsychotics (e.g. thioridazine); some macrolides (e.g. erythromycin); some antihistamines (e.g. terfenadine, astemizole); some quinolone antibiotics (e.g. gatifloxacin, moxifloxacin).
The previously mentioned list is not exhaustive and other individual drugs known to significantly increase QT interval (e.g. cisapride, lithium) should be avoided.
Drugs known to cause electrolyte disturbances such as thiazide diuretics (hypokalaemia) and drugs known to increase the plasma concentration of flupentixol should also be used with caution as they may increase the risk of QT prolongation and malignant arrhythmias (see Precautions).
Combinations requiring precautions for use: CNS depressants: Deanxit may enhance the effects of alcohol, barbiturates and other CNS depressants.
Lithium: Concomitant use of Deanxit and lithium increases the risk of neurotoxicity.
Levodopa: Deanxit may reduce the effect of levodopa and increase the risk of cardiac side effects.
Precautions for disposal: Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Not applicable.
Do not store above 30°C.
Store in the original package in order to protect from light.
Shelf life: 2 years.
N06CA02 - melitracen and psycholeptics ; Belongs to the class of antidepressants in combination with psycholeptics.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
