


 Sign Out
Sign Out

The adverse reactions reported during clinical trials and/or post-marketing use with finasteride and/or finasteride at lower doses are listed in the following table. (See table.)
Frequency of adverse reactions is determined as follows: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data).
The frequency of adverse reactions reported during post-marketing use cannot be determined as they are derived from spontaneous reports.
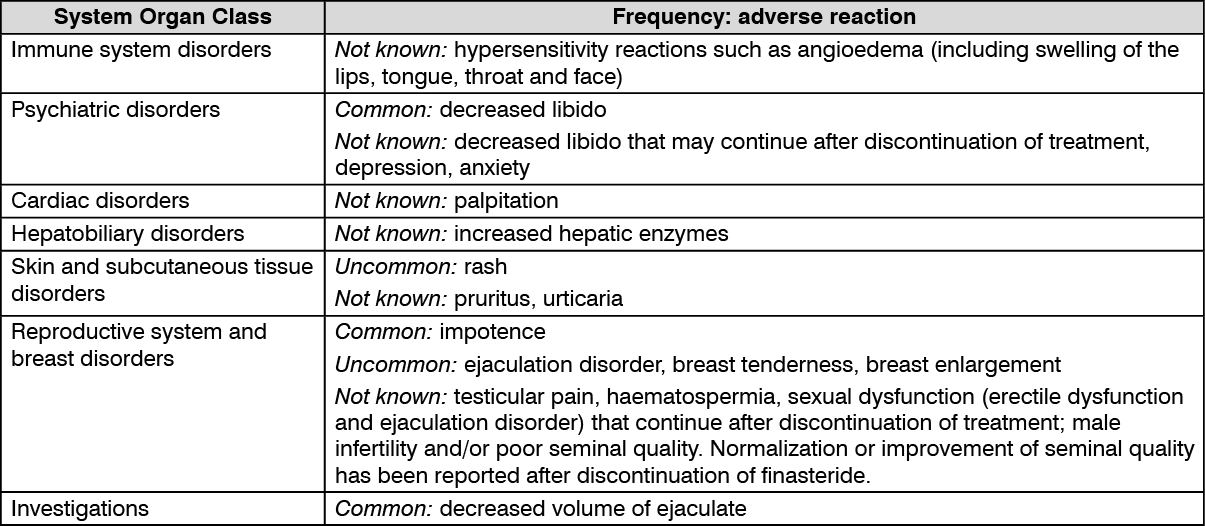 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn addition, the following has been reported in clinical trials and post-marketing use: male breast cancer (see Precautions).
Medical Therapy of Prostatic Symptoms (MTOPS): The MTOPS study compared finasteride 5 mg/day (n=768), doxazosin 4 or 8 mg/day (n=756), combination therapy of finasteride 5 mg/day and doxazosin 4 or 8 mg/day (n=786), and placebo (n=737). In this study, the safety and tolerability profile of the combination therapy was generally consistent with the profiles of the individual components. The incidence of ejaculation disorder in patients receiving combination therapy was comparable to the sum of incidences of this adverse experience of the two monotherapies.
Other Long-Term Data: In a 7-year placebo-controlled trial that enrolled 18,882 healthy men, of whom 9060 had prostate needle biopsy data available for analysis, prostate cancer was detected in 803 (18.4%) men receiving finasteride and 1147 (24.4%) men receiving placebo. A greater number of high-grade tumours (Gleason scores of 7-10) were detected on needle biopsy in patients in the finasteride group, 280 (6.4%) vs 237 (5.1%) men in the placebo group.
Additional analyses suggest that the increase in the prevalence of high-grade prostate cancer observed in the finasteride group may be explained by a detection bias due to the effect of finasteride on prostate volume. Of the total cases of prostate cancer diagnosed in this study, approximately 98% were classified as intracapsular (stage T1 or T2). The relationship between long-term use of finasteride and tumours with Gleason scores of 7-10 is unknown.
Laboratory Test Findings: Serum PSA concentration is correlated with patient age and prostatic volume, and prostatic volume is correlated with patient age. When PSA laboratory determinations are evaluated, consideration should be given to the fact that PSA levels are decreased in patients treated with finasteride (see Precautions). In most patients, a rapid decrease in PSA is seen within the first months of therapy, after which time PSA levels stabilise to a new baseline. The post-treatment baseline approximates half of the pre-treatment value. Therefore, in typical patients treated with finasteride for six months or more, PSA values should be doubled for comparison to normal ranges in untreated men.
For clinical interpretation, see Effects on prostate-specific antigen (PSA) and prostate cancer detection under Precautions.
No other difference was observed in patients treated with placebo or finasteride in standard laboratory tests.
View ADR Monitoring Form