


 Sign Out
Sign Out

Methotrexate injection may be given by the intramuscular, intravenous or intra-arterial route. The preserved formulation contains Benzyl Alcohol and must not be used for intrathecal or high dose therapy. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Choriocarcinoma and similar trophoblastic diseases: Methotrexate is administered orally or intramuscularly in doses of 15 to 30 mg daily for a five-day course. Such courses are usually repeated for 3 to 5 times as required, with rest periods of one or more weeks interposed between courses, until any manifesting toxic symptoms subside. The effectiveness of therapy is ordinarily evaluated by 24 hour quantitative analysis of urinary chorionic gonadotropin (hCG), which should return to normal or less than 50 IU/24 hr usually after the third or fourth course and usually be followed by a complete resolution of measurable lesions in 4 to 6 weeks. One to two courses of methotrexate after normalization of hCG is usually recommended. Before each course of the drug careful clinical assessment is essential. Cyclic combination therapy of methotrexate with other antitumor drugs has been reported as being useful.
Since hydatidiform mole may precede choriocarcinoma, prophylactic chemotherapy with methotrexate has been recommended.
Chorioadenoma destruens is considered to be an invasive form of hydatidiform mole. Methotrexate is administered in these disease states in doses similar to those recommended for choriocarcinoma.
Leukemia: Acute lymphoblastic leukemia in pediatric patients and young adolescents is the most responsive to present day chemotherapy. In young adults and older patients, clinical remission is more difficult to obtain and early relapse is more common.
Methotrexate alone or in combination with steroids was used initially for induction of remission in acute lymphoblastic leukemias. More recently corticosteroid therapy, in combination with other antileukemic drugs or in cyclic combinations with methotrexate included, has appeared to produce rapid and effective remissions. When used for induction, methotrexate in doses of 3.3 mg/m2 in combination with 60 mg/m2 of prednisone, given daily, produced remissions in 50% of patients treated, usually within a period of 4 to 6 weeks. Methotrexate in combination with other agents appears to be the drug of choice for securing maintenance of drug-induced remissions. When remission is achieved and supportive care has produced general clinical improvement, maintenance therapy is initiated, as follows: Methotrexate is administered 2 times weekly either by mouth or intramuscularly in total weekly doses of 30 mg/m2. It has also been given in doses of 2.5 mg/kg intravenously every 14 days. If and when relapse does occur, reinduction of remission can again usually be obtained by repeating the initial induction regimen.
A variety of combination chemotherapy regimens have been used for both induction and maintenance therapy in acute lymphoblastic leukemia. The physician should be familiar with the new advances in antileukemic therapy.
Meningeal Leukemia: In the treatment of prophylaxis of meningeal leukemia, methotrexate must be administered intrathecally. Preservative free methotrexate is diluted to a concentration of 1 mg/mL in an appropriate sterile, preservative free medium such as 0.9% Sodium Chloride Injection, USP.
The cerebrospinal fluid volume is dependent on age and not on body surface area. The CSF is at 40% of the adult volume at birth and reaches the adult volume in several years.
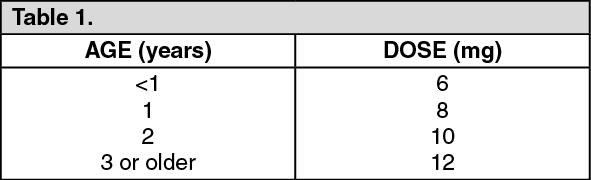
Intrathecal methotrexate administration at a dose of 12 mg/m2 (maximum 15 mg) has been reported to result in low CSF methotrexate concentrations and reduced efficacy in pediatric patients and high concentrations and neurotoxicity in adults. The following dosage regimen is based on age instead of body surface area: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn one study in patients under the age of 40, this dosage regimen appeared to result in more consistent CSF methotrexate concentrations and less neurotoxicity. Another study in pediatric patients with acute lymphocytic leukemia compared this regimen to a dose of 12 mg/m2 (maximum 15 mg), a significant reduction in the rate of CNS relapse was observed in the group whose dose was based on age. Because the CSF volume and turnover may decrease with age, a dose reduction may be indicated in elderly patients.
For treatment of meningeal leukemia, intrathecal methotrexate may be given at intervals of 2 to 5 days. However, administration at intervals of less than 1 week may result in increased subacute toxicity. Methotrexate is administered until the cell count of the cerebrospinal fluid returns to normal. At this point one additional dose is advisable. For prophylaxis against meningeal leukemia, the dosage is the same as for treatment except for the intervals of administration. On this subject, it is advisable for the physician to consult the medical literature.
Untoward side effects may occur with any given intrathecal injection and are commonly neurological in character. Large doses may cause convulsions. Methotrexate given by the intrathecal route appears significantly in the systemic circulation and may cause systemic methotrexate toxicity. Therefore, systemic antileukemic therapy with the drug should be appropriately adjusted, reduced or discontinued. Focal leukemic involvement of the central nervous system may not respond to intrathecal chemotherapy and is best treated with radiotherapy.
Lymphomas: In Burkitt's tumor, Stages I-II, methotrexate has produced prolonged remissions in some cases. Recommended dosage is 10 to 25 mg/day orally for 4 to 8 days. In Stage III, methotrexate is commonly given concomitantly with other antitumor agents. Treatment in all stages usually consists of several courses of the drug interposed with 7 to 10 day rest periods. Lymphosarcomas in Stage III may respond to combined drug therapy with methotrexate given in doses of 0.625 to 2.5 mg/kg daily.
Mycosis fungoides (cutaneous T cell lymphoma): Therapy with methotrexate as a single agent appears to produce clinical responses in up to 50% of patients treated. Dosage in early stages is usually 5 to 50 mg once weekly. Dose reduction or cessation is guided by patient response and hematologic monitoring. Methotrexate has also been administered twice weekly in doses ranging from 15 to 37.5 mg in patients who have responded poorly to weekly therapy. Combination chemotherapy regimens that include intravenous methotrexate administered at higher doses with leucovorin rescue have been utilized in advanced stages of the disease.
Osteosarcoma: An effective adjuvant chemotherapy regimen requires the administration of several cytotoxic chemotherapeutic agents. In addition to high-dose methotrexate with leucovorin rescue, these agents may include doxorubicin, cisplatin, and the combination of bleomycin, cyclophosphamide and dactinomycin (BCD) in the doses and schedule shown in the table as follows. The starting dose for high dose methotrexate treatment is 12 grams/m2. If this dose is not sufficient to produce a peak serum methotrexate concentration of 1,000 micromolar (10-3 mol/L) at the end of the methotrexate infusion, the dose may be escalated to 15 grams/m2 in subsequent treatments. If the patient is vomiting or is unable to tolerate oral medication, leucovorin is given IV or IM at the same dose and schedule. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen these higher doses of methotrexate are to be administered, the methotrexate safety with leucovorin rescue guidelines should be closely observed.
Guidelines for Methotrexate Therapy with Leucovorin Rescue: 1. Administration of methotrexate should be delayed until recovery if: The WBC count is less than 1500/microliter; The neutrophil count is less than 200/microliter; The platelet count is less than 75,000/microliter; The serum bilirubin level is greater than 1.2 mg/dL; The SGPT level is greater than 450 U; Mucositis is present, until there is evidence of healing; Persistent pleural effusion is present; this should be drained dry prior to infusion.
2. Adequate renal function must be documented.
a. Serum creatinine must be normal, and creatinine clearance must be greater than 60 mL/min, before initiation of therapy.
b. Serum creatinine must be measured prior to each subsequent course of therapy. If serum creatinine has increased by 50% or more compared to a prior value, the creatinine clearance must be measured and documented to be greater than 60 mL/min (even if the serum creatinine is still within the normal range).
3. Patients must be well hydrated, and must be treated with sodium bicarbonate for urinary alkalinization.
a. Administer 1,000 mL/m2 of intravenous fluid over 6 hours prior to initiation of the methotrexate infusion. Continue hydration at 125 mL/m2/hr (3 liters/m2/day) during the methotrexate infusion, and for 2 days after the infusion has been completed.
b. Alkalinize urine to maintain pH above 7.0 during methotrexate infusion and leucovorin calcium therapy. This can be accomplished by the administration of sodium bicarbonate orally or by incorporation into a separate intravenous solution.
4. Repeat serum creatinine and serum methotrexate 24 hours after starting methotrexate and at least once daily until the methotrexate level is below 5 x 10-8 mol/L (0.05 micromolar).
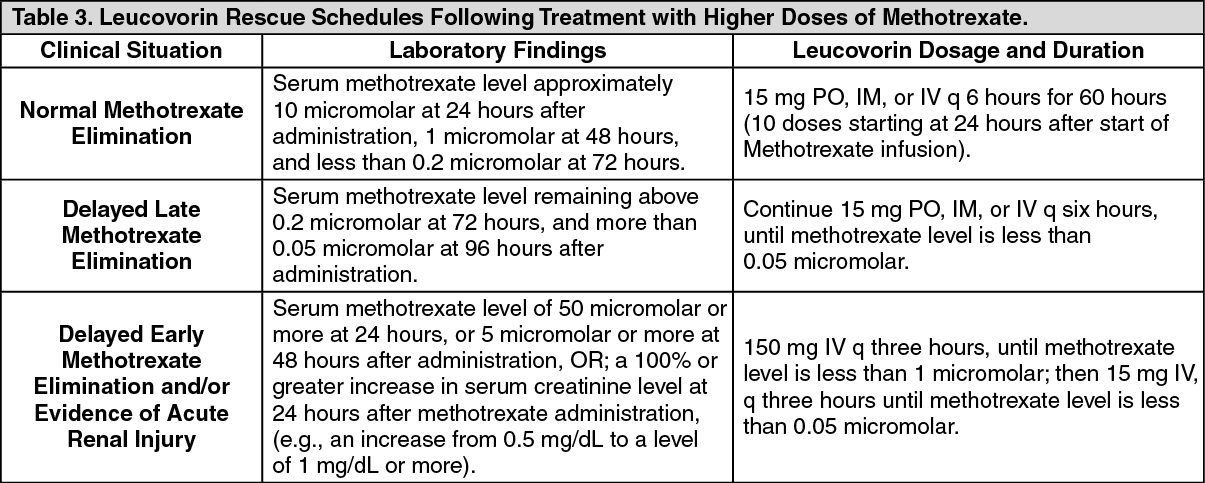
5. The table as follows provides guidelines for leucovorin calcium dosage based upon serum methotrexate levels. (See Table 3 as follows.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients who experience delayed early methotrexate elimination are likely to develop non reversible oliguric renal failure. In addition to appropriate leucovorin therapy, these patients require continuing hydration and urinary alkalinization, and close monitoring of fluid and electrolyte status, until the serum methotrexate level has fallen to below 0.05 micromolar and the renal failure has resolved. If necessary, acute, intermittent hemodialysis with a high-flux dialyzer may also be beneficial in these patients.
6. Some patients will have abnormalities in methotrexate elimination, or abnormalities in renal function following methotrexate administration, which are significant but less severe than the abnormalities described in the table as follows. These abnormalities may or may not be associated with significant clinical toxicity. If significant toxicity is observed, leucovorin rescue should be extended for an additional 24 hours (total 14 doses over 84 hours) in subsequent courses of therapy. The possibility that the patient is taking other medications which interact with methotrexate (e.g., medications which may interfere with methotrexate binding to serum albumin, or elimination) should always be reconsidered when laboratory abnormalities or clinical toxicities are observed.
CAUTION: Do Not Administer Leucovorin Intrathecally.
Psoriasis, Rheumatoid Arthritis, and Juvenile Rheumatoid Arthritis: Adult Rheumatoid Arthritis: Recommended Starting Dosage Schedules: 1. Single oral doses of 7.5 mg once weekly.†
2. Divided oral dosages of 2.5 mg at 12 hour intervals for 3 doses given as a course once weekly.†
† Methotrexate Sodium Tablets for oral administration are available.
Polyarticular-Course Juvenile Rheumatoid Arthritis: The recommended starting dose is 10 mg/m2 given once weekly.
For either adult RA or polyarticular-course JRA, dosages may be adjusted gradually to achieve an optimal response. Limited experience shows a significant increase in the incidence and severity of serious toxic reactions, especially bone marrow suppression, at doses greater than 20 mg/wk in adults. Although there is experience with doses up to 30 mg/m2/wk in children, there are too few published data to assess how doses over 20 mg/m2/wk might affect the risk of serious toxicity in children. Experience does suggest, however, that children receiving 20 to 30 mg/m2/wk (0.65 to 1.0 mg/kg/wk) may have better absorption and fewer gastrointestinal side effects if methotrexate is administered either intramuscularly or subcutaneously.
Therapeutic response usually begins within 3 to 6 weeks and the patient may continue to improve for another 12 weeks or more.
The optimal duration of therapy is unknown. Limited data available from long-term studies in adults indicate that the initial clinical improvement is maintained for at least two years with continued therapy. When methotrexate is discontinued, the arthritis usually worsens within 3 to 6 weeks.
The patient should be fully informed of the risks involved and should be under constant supervision of the physician.
Assessment of hematologic, hepatic, renal, and pulmonary function should be made by history, physical examination, and laboratory tests before beginning, periodically during, and before reinstituting methotrexate therapy. Appropriate steps should be taken to avoid conception during methotrexate therapy.
All schedules should be continually tailored to the individual patient. An initial test dose may be given prior to the regular dosing schedule to detect any extreme sensitivity to adverse effects. Maximal myelosuppression usually occurs in seven to ten days.
Psoriasis: Recommended Starting Dose Schedule: 1. Weekly single oral, IM or IV dosage schedule: 10 to 25 mg per week until adequate response is achieved. †
2. Divided oral dose schedule 2.5 mg at 12 hour intervals for three doses.†
† Methotrexate Sodium Tablets for oral administration are available.
Dosages in each schedule may be gradually adjusted to achieve optimal clinical response; 30 mg/week should not ordinarily be exceeded.
Once optimal clinical response has been achieved, each dosage schedule should be reduced to the lowest possible amount of drug and to the longest possible rest period. The use of methotrexate may permit the return to conventional topical therapy, which should be encouraged.
Dilution Instructions for Liquid Methotrexate Injection Product: If desired, the solution may be further diluted immediately prior to use with an appropriate sterile, preservative free medium such as 5% Dextrose Solution, USP or 0.9% Sodium Chloride Injection, USP.